Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Psych Drugs Cheat SheetDokument4 SeitenPsych Drugs Cheat SheetSunel100% (35)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Psychiatry - TreatmentDokument19 SeitenPsychiatry - TreatmentJYG100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Anatomy TerminologyDokument20 SeitenAnatomy Terminologykhabbab hussainNoch keine Bewertungen
- Basic Principles of Blending: Selecting Essential OilsDokument3 SeitenBasic Principles of Blending: Selecting Essential OilsRullya WindyaNoch keine Bewertungen
- Leaky Gut TreatmentDokument5 SeitenLeaky Gut Treatmentfsilassie8012Noch keine Bewertungen
- GERD (Gastroesophageal Reflux Disease)Dokument112 SeitenGERD (Gastroesophageal Reflux Disease)Mharj Alfelor Cecilio100% (7)
- Case Presentation OF: Iron Deficiency AnemiaDokument33 SeitenCase Presentation OF: Iron Deficiency Anemiaitshurt_teardrops100% (1)
- Cancer QuizDokument7 SeitenCancer QuizJoshua Flores Fernan100% (1)
- Neurogenic Shock in Critical Care NursingDokument25 SeitenNeurogenic Shock in Critical Care Nursingnaqib25100% (4)
- Brain Edema XVI - Translate Basic Science Into Clinical Practice by Richard L Applegate, Gang Chen, Hua Feng, John H. ZhangDokument376 SeitenBrain Edema XVI - Translate Basic Science Into Clinical Practice by Richard L Applegate, Gang Chen, Hua Feng, John H. ZhangAjie WitamaNoch keine Bewertungen
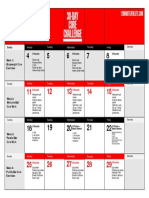
- Core Challenge Workout CalendarDokument1 SeiteCore Challenge Workout CalendarJYGNoch keine Bewertungen
- Opthalmology - Summary TableDokument4 SeitenOpthalmology - Summary TableJYGNoch keine Bewertungen
- Serotonin SyndromeDokument1 SeiteSerotonin SyndromeJYGNoch keine Bewertungen
- Syncope AlgorithmDokument1 SeiteSyncope AlgorithmJYGNoch keine Bewertungen
- OBSGYN - Shoulder DystociaDokument6 SeitenOBSGYN - Shoulder DystociaJYGNoch keine Bewertungen
- Background: Alpha-1 Antitrypsin DeficiencyDokument2 SeitenBackground: Alpha-1 Antitrypsin DeficiencyJYGNoch keine Bewertungen
- List of SymptomsDokument2 SeitenList of SymptomsJYGNoch keine Bewertungen
- List of SymptomsDokument2 SeitenList of SymptomsJYGNoch keine Bewertungen
- Drug Name Function Mechanism of ActionDokument1 SeiteDrug Name Function Mechanism of ActionJYGNoch keine Bewertungen
- Prevalence of Cusp of Carabelli in Permanent Teeth in A Group of Dental Student of School of Dentistry at University of SulaimaniDokument2 SeitenPrevalence of Cusp of Carabelli in Permanent Teeth in A Group of Dental Student of School of Dentistry at University of SulaimaniIOSRjournalNoch keine Bewertungen
- LAB 4 - StreptococcusDokument31 SeitenLAB 4 - Streptococcussajad abasNoch keine Bewertungen
- Presentation On Hysterosalpingography: BY Mahmud M Alkali I.D: 12/01/09/069 Radiography, Unimaid. 2014/2015 SESSIONDokument23 SeitenPresentation On Hysterosalpingography: BY Mahmud M Alkali I.D: 12/01/09/069 Radiography, Unimaid. 2014/2015 SESSIONMubarak M AlkaliNoch keine Bewertungen
- Fon by SatarDokument40 SeitenFon by SatarAqib SatarNoch keine Bewertungen
- Family Health Survey ToolDokument7 SeitenFamily Health Survey ToolReniella HidalgoNoch keine Bewertungen
- Claim IntimationDokument2 SeitenClaim IntimationSyed's Way PoolNoch keine Bewertungen
- Patient Education: Colic (Excessive Crying) in Infants (Beyond The Basics)Dokument15 SeitenPatient Education: Colic (Excessive Crying) in Infants (Beyond The Basics)krh5fnjnprNoch keine Bewertungen
- 1ST Module Physical EducationDokument2 Seiten1ST Module Physical EducationKirs MreyNoch keine Bewertungen
- SMH Annual Report 2016Dokument12 SeitenSMH Annual Report 2016Chelsey BoyleNoch keine Bewertungen
- Genre AnalysisDokument9 SeitenGenre Analysisapi-313293562Noch keine Bewertungen
- SECOND Semester, AY 2022-2023: Mission VisionDokument34 SeitenSECOND Semester, AY 2022-2023: Mission Visionjeyyy BonesssNoch keine Bewertungen
- Strabismus and Eye Muscle SurgeryDokument68 SeitenStrabismus and Eye Muscle SurgeryOpeyemi IdaeworNoch keine Bewertungen
- Vertical Farming-EENADU - My Simple Innovative and Cost Effective Method & OthersDokument34 SeitenVertical Farming-EENADU - My Simple Innovative and Cost Effective Method & OthersAnumakonda JagadeeshNoch keine Bewertungen
- GuiademedicamentosDokument59 SeitenGuiademedicamentospaolarestauroNoch keine Bewertungen
- Hazard Identification and Risk AssesmentDokument4 SeitenHazard Identification and Risk AssesmentsuyatnofkmundipNoch keine Bewertungen
- VSR 421Dokument2 SeitenVSR 421AdarshBijapur0% (1)
- UT Dallas Syllabus For Biol1318.001 05f Taught by Lee Bulla (Bulla)Dokument1 SeiteUT Dallas Syllabus For Biol1318.001 05f Taught by Lee Bulla (Bulla)UT Dallas Provost's Technology GroupNoch keine Bewertungen
- Blood Gas Report Siemens RL 348EX-UpdateDokument2 SeitenBlood Gas Report Siemens RL 348EX-UpdateLaboratorium RS Royal ProgressNoch keine Bewertungen
- Chart AuditDokument3 SeitenChart AuditAnonymous WJtqIhhvPNoch keine Bewertungen
- TAPSE AgainDokument8 SeitenTAPSE Againomotola ajayiNoch keine Bewertungen
- Blood Pressure ChartDokument7 SeitenBlood Pressure ChartsolomwanNoch keine Bewertungen