Das könnte Ihnen auch gefallen
- Esophagus Supafirefly Plan ComparisonDokument5 SeitenEsophagus Supafirefly Plan Comparisonapi-426737835Noch keine Bewertungen
- 1 StfallevalDokument5 Seiten1 Stfallevalapi-432489466Noch keine Bewertungen
- 3d HN PlanDokument2 Seiten3d HN Planapi-426737835Noch keine Bewertungen
- Fall Aff Eval 3Dokument5 SeitenFall Aff Eval 3api-426737835Noch keine Bewertungen
- Craniospinal IrraditationDokument8 SeitenCraniospinal Irraditationapi-426737835Noch keine Bewertungen
- Fall Case Log TotalDokument2 SeitenFall Case Log Totalapi-426737835Noch keine Bewertungen
- Case Log Totals SummerDokument2 SeitenCase Log Totals Summerapi-426737835Noch keine Bewertungen
- Aff Eval 3Dokument5 SeitenAff Eval 3api-426737835Noch keine Bewertungen
- 1 StfallevalDokument5 Seiten1 Stfallevalapi-432489466Noch keine Bewertungen
- 2nd EvaluationDokument5 Seiten2nd Evaluationapi-491087286Noch keine Bewertungen
- Lung PaperDokument17 SeitenLung Paperapi-426737835Noch keine Bewertungen
- Affective Eval 1Dokument3 SeitenAffective Eval 1api-426737835Noch keine Bewertungen
- Extra Credit QuestionsDokument6 SeitenExtra Credit Questionsapi-334402872Noch keine Bewertungen
- Spring Case Log TotalsDokument2 SeitenSpring Case Log Totalsapi-426737835Noch keine Bewertungen
- Lit Review ActivityDokument9 SeitenLit Review Activityapi-426737835Noch keine Bewertungen
- Aff Eval 2 2Dokument3 SeitenAff Eval 2 2api-426737835Noch keine Bewertungen
- Aff Eval 3Dokument3 SeitenAff Eval 3api-426737835Noch keine Bewertungen
- Affective Eval 2Dokument3 SeitenAffective Eval 2api-426737835Noch keine Bewertungen
- Statistics Activity 2012 1Dokument5 SeitenStatistics Activity 2012 1api-203178352Noch keine Bewertungen
- Pelvis PP 2018 2Dokument12 SeitenPelvis PP 2018 2api-426737835Noch keine Bewertungen
- Practice Problems Week 4 2019 3Dokument3 SeitenPractice Problems Week 4 2019 3api-505214441Noch keine Bewertungen
- Pelvis Clinical Lab AssignmentDokument5 SeitenPelvis Clinical Lab Assignmentapi-426737835Noch keine Bewertungen
- Thorax PPDokument4 SeitenThorax PPapi-213055674Noch keine Bewertungen
- Abdomen PP 2014Dokument5 SeitenAbdomen PP 2014api-335978335Noch keine Bewertungen
- Head PP Rev 2017Dokument9 SeitenHead PP Rev 2017api-373037339Noch keine Bewertungen
- Sectional Anatomy Neck Practice ProblemsDokument4 SeitenSectional Anatomy Neck Practice Problemsapi-426737835Noch keine Bewertungen
- Practice Problems Chapters 6 8 1Dokument6 SeitenPractice Problems Chapters 6 8 1api-374655242Noch keine Bewertungen
- Safety in Radiation OncologyDokument3 SeitenSafety in Radiation Oncologyapi-426737835Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Diagnosis of Bronchial AsthmaDokument12 SeitenDiagnosis of Bronchial AsthmaVineet Mariyappan100% (1)
- Low Back Pain - Differential Diagnosis, Prognosis and TreatmentDokument4 SeitenLow Back Pain - Differential Diagnosis, Prognosis and TreatmentFifi TandionNoch keine Bewertungen
- NCP LeukemiaDokument3 SeitenNCP LeukemiaLuige Avila100% (5)
- Benign Prostatic Hyperplasia (BPH) : Hyperplasia: Diagnosis and Treatment (1994) Was The Starting Point ForDokument14 SeitenBenign Prostatic Hyperplasia (BPH) : Hyperplasia: Diagnosis and Treatment (1994) Was The Starting Point ForAnemiaHemolyticNoch keine Bewertungen
- Parking Placards Reg 3164Dokument2 SeitenParking Placards Reg 3164David BatesNoch keine Bewertungen
- (Essential Skills For Nurses Series) Philippa Sully - Joan Dallas-Essential Communication Skills For Nursing and Midwifery-Mosby - Elsevier (2010)Dokument250 Seiten(Essential Skills For Nurses Series) Philippa Sully - Joan Dallas-Essential Communication Skills For Nursing and Midwifery-Mosby - Elsevier (2010)library madaniNoch keine Bewertungen
- Annual Review of CyberTherapy and Telemedicine, Volume 2, Summer 2004Dokument206 SeitenAnnual Review of CyberTherapy and Telemedicine, Volume 2, Summer 2004Giuseppe Riva100% (2)
- Yip Et Al. - 2019 - Connectome-Based Prediction of Cocaine AbstinenceDokument9 SeitenYip Et Al. - 2019 - Connectome-Based Prediction of Cocaine AbstinencefacepalmerNoch keine Bewertungen
- Late Career Practitioner Policy SHC 10 13Dokument13 SeitenLate Career Practitioner Policy SHC 10 13Dani GintingNoch keine Bewertungen
- PL 100718Dokument101 SeitenPL 100718eka oktaviana hirdaNoch keine Bewertungen
- TommatisDokument9 SeitenTommatisAldo PrietoNoch keine Bewertungen
- Apps For AutismDokument1 SeiteApps For Autismapi-407131623Noch keine Bewertungen
- Good Will Hunting Thesis StatementsDokument5 SeitenGood Will Hunting Thesis Statementsafloihzesdawig100% (2)
- Blood DonationDokument76 SeitenBlood Donationlanie_bluegirl100% (1)
- URGE SURFING-DBT For Sub Use PDFDokument5 SeitenURGE SURFING-DBT For Sub Use PDFAmy Powers100% (1)
- A Case Based Guide To Clinical Endocrinology 3rd Edition 2022Dokument528 SeitenA Case Based Guide To Clinical Endocrinology 3rd Edition 2022Muhammad Ahmad bin makruf syammakuNoch keine Bewertungen
- Therapeutics PlanningDokument13 SeitenTherapeutics PlanningCésar Augusto Sánchez SolisNoch keine Bewertungen
- Park Young Guk - Photobiomodulation Light Accelerated Orthodontics To Reduce Treatment DurationDokument15 SeitenPark Young Guk - Photobiomodulation Light Accelerated Orthodontics To Reduce Treatment DurationsillyazianNoch keine Bewertungen
- Child PPT Conference MineDokument28 SeitenChild PPT Conference MineSeerat FatimaNoch keine Bewertungen
- Medical Gas TherapyDokument84 SeitenMedical Gas TherapyJohn Carlo TanNoch keine Bewertungen
- Centric & Protrusive RecordDokument51 SeitenCentric & Protrusive RecordHadil AltilbaniNoch keine Bewertungen
- Revista Chilena de Neuro-Psiquiatría: La Persona Del Terapeuta: Eje Fundamental de Todo Proceso TerapéuticoDokument13 SeitenRevista Chilena de Neuro-Psiquiatría: La Persona Del Terapeuta: Eje Fundamental de Todo Proceso TerapéuticocysagasNoch keine Bewertungen
- Interpersonal RelationshipsDokument51 SeitenInterpersonal RelationshipsNeeraj Bhardwaj86% (14)
- Breathing TherapyDokument8 SeitenBreathing Therapyzarrar100% (1)
- MPS Therapy Flyer April 10 2018Dokument8 SeitenMPS Therapy Flyer April 10 2018Neptune ShellNoch keine Bewertungen
- Anxiety ManagementDokument2 SeitenAnxiety ManagementYanira RiveraNoch keine Bewertungen
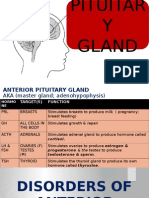
- Disorders of Pituitary GlandDokument34 SeitenDisorders of Pituitary GlandninaaltheaNoch keine Bewertungen
- Ift PDFDokument10 SeitenIft PDFJulyhathul KuraishiNoch keine Bewertungen
- Spine Care Technologies Inc. To Attend Arab Health2020 in Dubai, UAEDokument2 SeitenSpine Care Technologies Inc. To Attend Arab Health2020 in Dubai, UAEPR.comNoch keine Bewertungen
- IMCI Chart BookletDokument43 SeitenIMCI Chart Bookletmysticeyes_17100% (1)