Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Cargo Hold Cleaning Chemical RecommendationDokument1 SeiteCargo Hold Cleaning Chemical Recommendation123456Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Handymax Hold Cleaning KitDokument3 SeitenHandymax Hold Cleaning Kit123456Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Mcm-200 Telescopic Pole Water Jet Gun LatestDokument3 SeitenMcm-200 Telescopic Pole Water Jet Gun Latest123456Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Guidance On Eliminating Shipboard Harassment and BullyingDokument16 SeitenGuidance On Eliminating Shipboard Harassment and BullyingAnonymous LY6TDeNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- RCA Mini Guide PDFDokument15 SeitenRCA Mini Guide PDFIldzamar Haifa WardhaniNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Dunnage CalculatorDokument3 SeitenDunnage Calculator123456Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Japan P&I Bulletin Vol 19-20 2011Dokument19 SeitenJapan P&I Bulletin Vol 19-20 2011123456Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- RCA Mini Guide PDFDokument15 SeitenRCA Mini Guide PDFIldzamar Haifa WardhaniNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Terms of Implement BSCI Participants PDFDokument4 SeitenTerms of Implement BSCI Participants PDFvintecomNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- SOP QA 010 00 Handling of DeviationDokument17 SeitenSOP QA 010 00 Handling of Deviationnetelsrt129867% (3)
- ISO 9001 2015 Interpretation Guidance SampleDokument9 SeitenISO 9001 2015 Interpretation Guidance SampleIhabNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Customer Specific Requirment - 2021-22 - TML CSR Rev04Dokument5 SeitenCustomer Specific Requirment - 2021-22 - TML CSR Rev04Ali MujawarNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- ATS Supplier Survey EvaluationDokument26 SeitenATS Supplier Survey EvaluationAtul SanghaviNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Quick Response Quality Control As An Innovative ApDokument6 SeitenQuick Response Quality Control As An Innovative ApfatimaNoch keine Bewertungen
- (SOP16) LUS-HSE-SP2-453-002.04 - Internal Audit Procedure PDFDokument10 Seiten(SOP16) LUS-HSE-SP2-453-002.04 - Internal Audit Procedure PDFKien Trung NguyenNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- CAPA ProcedureDokument15 SeitenCAPA Proceduresudar1477Noch keine Bewertungen
- Purchasing Process in Prep For ISODokument4 SeitenPurchasing Process in Prep For ISObrecht1980Noch keine Bewertungen
- Migration Guide: ISO 45001 Occupational Health and Safety Management SystemsDokument17 SeitenMigration Guide: ISO 45001 Occupational Health and Safety Management SystemsShivam VermaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Iso 9004 2009 Compliance Audit Tool: 7.1 Using A Process ApproachDokument6 SeitenIso 9004 2009 Compliance Audit Tool: 7.1 Using A Process ApproachAyman Al-sayyedNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Eaton Global Supplier Excellence ManualDokument30 SeitenEaton Global Supplier Excellence Manualfdsa01100% (1)
- Oos MhraDokument30 SeitenOos MhraMostofa Rubal100% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- ISO 50001 Implementation Guide WebDokument12 SeitenISO 50001 Implementation Guide WebibnmosawiNoch keine Bewertungen
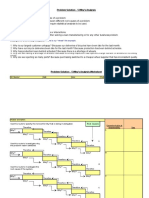
- 5 Whys Analysis SheetDokument3 Seiten5 Whys Analysis SheetbhushansalunkeNoch keine Bewertungen
- Quality Notification CAPADokument3 SeitenQuality Notification CAPAindravathiNoch keine Bewertungen
- Laboratory &: Controls ComplianceDokument16 SeitenLaboratory &: Controls CompliancemmmmmNoch keine Bewertungen
- Technical Guidance Document For Environmental Audit ReportsDokument15 SeitenTechnical Guidance Document For Environmental Audit ReportsNisa KgNoch keine Bewertungen
- Nonconformity ReportDokument3 SeitenNonconformity ReportkumaravNoch keine Bewertungen
- Deviation ManagementDokument43 SeitenDeviation ManagementAmit Mishra100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Ilac G13 08 2007Dokument35 SeitenIlac G13 08 2007sidiaissaouiNoch keine Bewertungen
- ISO 22000:2018 ChecklistDokument13 SeitenISO 22000:2018 Checklist996066274497% (30)
- (QSP-QA-08) Process For Internal Rejection HandelingDokument4 Seiten(QSP-QA-08) Process For Internal Rejection HandelingMUNENDRA SHAKYANoch keine Bewertungen
- PMP Application Project CalculationsDokument42 SeitenPMP Application Project CalculationsManoj SinghNoch keine Bewertungen
- Guidelines For Glass Manufacturers: Packaging MaterialsDokument23 SeitenGuidelines For Glass Manufacturers: Packaging MaterialskhalidasyNoch keine Bewertungen
- ICH Q10 Pharmaceutical Quality System Apr12Dokument8 SeitenICH Q10 Pharmaceutical Quality System Apr12geeenaaNoch keine Bewertungen
- Criteria For SQF Certification Bodies: 7th EditionDokument22 SeitenCriteria For SQF Certification Bodies: 7th EditionAlejandro Herrnsdorf-SakellaridisNoch keine Bewertungen
- US Vs Real Water: ComplaintDokument19 SeitenUS Vs Real Water: ComplaintTony OrtegaNoch keine Bewertungen
- PI - Standard - Feed Mill Standard - Issue 3.0 - 15-June-2020 PDFDokument28 SeitenPI - Standard - Feed Mill Standard - Issue 3.0 - 15-June-2020 PDFHelmut AlemánNoch keine Bewertungen
- 1 Kitchen Tech OH&S ManualDokument15 Seiten1 Kitchen Tech OH&S Manualjeromejaradan100% (2)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)