Das könnte Ihnen auch gefallen
- Ok Ok Notes PediaDokument14 SeitenOk Ok Notes PediaChristian PasicolanNoch keine Bewertungen
- Problem Set: The Endocrine SystemDokument6 SeitenProblem Set: The Endocrine SystemMyshaM0990% (3)
- Dr. Shehla Jamal Assistant Professor: OBG S M S & RDokument69 SeitenDr. Shehla Jamal Assistant Professor: OBG S M S & RAppy LoveNoch keine Bewertungen
- 3 AmenorrrheaDokument29 Seiten3 AmenorrrheaKilp MosesNoch keine Bewertungen
- AmenorrheaDokument55 SeitenAmenorrheaAla AbushehabNoch keine Bewertungen
- AmenorrheaDokument26 SeitenAmenorrheaThatStudentNoch keine Bewertungen
- 2 AmenorrheaDokument41 Seiten2 AmenorrheaKilp MosesNoch keine Bewertungen
- Primary Amenorrhoea 2Dokument42 SeitenPrimary Amenorrhoea 2sivaNoch keine Bewertungen
- Clinical Guidelines ForDokument54 SeitenClinical Guidelines ForHenry SudharsonoNoch keine Bewertungen
- AmenorrheaDokument41 SeitenAmenorrheaBonitavanyNoch keine Bewertungen
- Perdarahan Uterus DisfungsionalDokument22 SeitenPerdarahan Uterus DisfungsionalAggiFitiyaningsihNoch keine Bewertungen
- Amen or RheaDokument41 SeitenAmen or Rheakhadzx100% (2)
- AmenorrheaDokument41 SeitenAmenorrheadoraNoch keine Bewertungen
- An Overview in InfertilityDokument50 SeitenAn Overview in InfertilityNi Wayan Yunita SariNoch keine Bewertungen
- Infertility in Male and FemaleDokument27 SeitenInfertility in Male and FemaleDanai JanuaritaNoch keine Bewertungen
- Biochemical Investigation of Infertile Couple-My PresentationDokument91 SeitenBiochemical Investigation of Infertile Couple-My PresentationOlukoyejo OluwaboriNoch keine Bewertungen
- 2.1.6.2 Amenorea Dan DismenoreaDokument21 Seiten2.1.6.2 Amenorea Dan DismenoreaRahmatia SyukrinaNoch keine Bewertungen
- Menstrual Disorders and PCOS Webinar EMBRYO FKUI 2022Dokument49 SeitenMenstrual Disorders and PCOS Webinar EMBRYO FKUI 2022angelinputri100% (1)
- InfertilityDokument18 SeitenInfertilityphuyalaryan666Noch keine Bewertungen
- Chapter 27. Amenorrhea: Berek & Novak's Gynecology 14 Edition (P 1035 1068) R3 Jung Mi ByunDokument95 SeitenChapter 27. Amenorrhea: Berek & Novak's Gynecology 14 Edition (P 1035 1068) R3 Jung Mi Byunhossam626Noch keine Bewertungen
- Amenorrhea: Oleh Dr. H M A Ashari SpogDokument29 SeitenAmenorrhea: Oleh Dr. H M A Ashari SpogsiTengilNoch keine Bewertungen
- AmenorrhoeaDokument38 SeitenAmenorrhoeaheydydNoch keine Bewertungen
- 4.primary - Secondary AmenorrheaDokument5 Seiten4.primary - Secondary AmenorrheaAhmed Al GhaithiNoch keine Bewertungen
- Physiology of Female ReproductionDokument3 SeitenPhysiology of Female ReproductionAntoine JeriNoch keine Bewertungen
- Amenorrhea: Oleh Dr. H M A Ashari Spog (K)Dokument29 SeitenAmenorrhea: Oleh Dr. H M A Ashari Spog (K)Devi SuryandariNoch keine Bewertungen
- Amenorrhea ImprovedDokument3 SeitenAmenorrhea ImprovedCriselda Charisse ReganionNoch keine Bewertungen
- Amen or RheaDokument34 SeitenAmen or RheaAsma Naseer CheemaNoch keine Bewertungen
- 4.4 (Amenorrhea) University of AlexanderDokument28 Seiten4.4 (Amenorrhea) University of AlexanderAnonymous XSXlZJvyWNoch keine Bewertungen
- Seminar: Guide: Co-Guide: Pramoted byDokument35 SeitenSeminar: Guide: Co-Guide: Pramoted byDhara MeenaNoch keine Bewertungen
- Shigref MushtaqDokument28 SeitenShigref Mushtaqeisha aliNoch keine Bewertungen
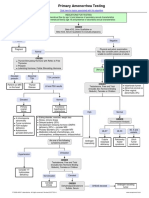
- Primary Amenorrhea Testing AlgorithmDokument1 SeitePrimary Amenorrhea Testing AlgorithmGabriella AguirreNoch keine Bewertungen
- Primary Amenorrhea Testing AlgorithmDokument1 SeitePrimary Amenorrhea Testing AlgorithmfarmasiNoch keine Bewertungen
- Amenorrhea PDFDokument5 SeitenAmenorrhea PDFKenneth Robin CarbonellNoch keine Bewertungen
- Gynecology - Secondary AmenorrheaDokument2 SeitenGynecology - Secondary AmenorrheaAnsley MadalaNoch keine Bewertungen
- OB 2nd SGDDokument4 SeitenOB 2nd SGDJxyp MundoNoch keine Bewertungen
- Precociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Dokument31 SeitenPrecociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Priya RaviNoch keine Bewertungen
- Ambiguous GenitaliaDokument16 SeitenAmbiguous Genitaliamohdmaghyreh100% (1)
- Primary Amenorrhea: Rabika Almina RabiaDokument30 SeitenPrimary Amenorrhea: Rabika Almina RabiaAlmina RehmanNoch keine Bewertungen
- First Aid For The OBS&GYN Clerkship CH 17 (Amenorrhea)Dokument9 SeitenFirst Aid For The OBS&GYN Clerkship CH 17 (Amenorrhea)黃芳昌Noch keine Bewertungen
- Amenorrhea - Algorithm & DifferentialsDokument9 SeitenAmenorrhea - Algorithm & DifferentialsItharshan IndreswaranNoch keine Bewertungen
- Infertility 001Dokument257 SeitenInfertility 001Habtamu Nigussie100% (1)
- Laboratory and Radiographic Tests For Ambiguous GenitaliaDokument8 SeitenLaboratory and Radiographic Tests For Ambiguous GenitaliaMaria Lucia RossiNoch keine Bewertungen
- Simplifikasi Amenore: Hanom Husni SyamDokument30 SeitenSimplifikasi Amenore: Hanom Husni Syamamarendra WardhanaNoch keine Bewertungen
- Infertility: Villanueva, Ian Joseph Virata, Marc Jenaro Yabuki, Ukari Yambot, Kathleen KayDokument13 SeitenInfertility: Villanueva, Ian Joseph Virata, Marc Jenaro Yabuki, Ukari Yambot, Kathleen KayBea SamonteNoch keine Bewertungen
- Obstetrics & Gynecology NotesDokument7 SeitenObstetrics & Gynecology NotesMary Ella WoodNoch keine Bewertungen
- AmenorrheaDokument41 SeitenAmenorrheaarfahregarNoch keine Bewertungen
- Laboratory Tests For EndocrinologyDokument6 SeitenLaboratory Tests For EndocrinologyAnastasia100% (1)
- Amenorrhea & Heavy Menstrual BleedingDokument22 SeitenAmenorrhea & Heavy Menstrual BleedingJanesel Plariza PanerioNoch keine Bewertungen
- Secondary Amenorrhea: DR Hanaa AlaniDokument44 SeitenSecondary Amenorrhea: DR Hanaa AlaniAakashNoch keine Bewertungen
- AmenorrheaDokument41 SeitenAmenorrheaDewi Felayati Gusni100% (2)
- Amenorrhea: DR - Muhammad Rusda, SP - OG (K)Dokument41 SeitenAmenorrhea: DR - Muhammad Rusda, SP - OG (K)sridhaniNoch keine Bewertungen
- AmenorrheaDokument13 SeitenAmenorrheaJanesel Plariza PanerioNoch keine Bewertungen
- IVF Infertility Treatment IndiaDokument26 SeitenIVF Infertility Treatment India24x7emarketing100% (1)
- Amenorrhea WorkupDokument10 SeitenAmenorrhea WorkupHaoKeat HoeNoch keine Bewertungen
- Homoeopathic Management of InfertilityDokument92 SeitenHomoeopathic Management of InfertilityDrSaji86% (7)
- Hyper Pro Lac Tine MiaDokument47 SeitenHyper Pro Lac Tine Miakharbosham100% (3)
- Amenorrhoea Primary & SecondaryDokument24 SeitenAmenorrhoea Primary & SecondaryAnushaAgrawalNoch keine Bewertungen
- Assesment of Amen or RheaDokument49 SeitenAssesment of Amen or Rheakhadzx100% (2)
- Laboratory Investigation of Amenorrhea:: DefinitionsDokument8 SeitenLaboratory Investigation of Amenorrhea:: DefinitionsAmelia SetiawatiNoch keine Bewertungen
- Obstetrics & Gynecology: Original Review & Revision HyderabadDokument739 SeitenObstetrics & Gynecology: Original Review & Revision Hyderabad24k.avinashNoch keine Bewertungen
- AMENORRHOEADokument16 SeitenAMENORRHOEAdrravindermehetreyNoch keine Bewertungen
- 2019 PPMP and App-Non Cse FormDokument8 Seiten2019 PPMP and App-Non Cse FormChristian PasicolanNoch keine Bewertungen
- Physics of RadiologyDokument9 SeitenPhysics of RadiologyChristian PasicolanNoch keine Bewertungen
- Lec 4 Platelet and CoagulationDokument17 SeitenLec 4 Platelet and CoagulationChristian PasicolanNoch keine Bewertungen
- Narag, MarkDokument64 SeitenNarag, MarkChristian PasicolanNoch keine Bewertungen
- ENDOMETRIOSISDokument5 SeitenENDOMETRIOSISChristian PasicolanNoch keine Bewertungen
- Pediatrics Tckler-3 PDFDokument100 SeitenPediatrics Tckler-3 PDFChristian PasicolanNoch keine Bewertungen
- Cagayan Valley Medical Center Carig Sur, Tuguegarao City CagayanDokument8 SeitenCagayan Valley Medical Center Carig Sur, Tuguegarao City CagayanChristian PasicolanNoch keine Bewertungen
- Pedia OncoDokument8 SeitenPedia OncoChristian PasicolanNoch keine Bewertungen
- Pedia Tickler Cont 20190210175903 PDFDokument80 SeitenPedia Tickler Cont 20190210175903 PDFChristian PasicolanNoch keine Bewertungen
- LeukemiaDokument33 SeitenLeukemiaChristian PasicolanNoch keine Bewertungen
- Cagayan State University - College of Information TechnologyDokument26 SeitenCagayan State University - College of Information TechnologyChristian Pasicolan50% (2)
- WRUV7926Dokument3 SeitenWRUV7926rajashekarcse533Noch keine Bewertungen
- Sonography of Normal and Abnormal Thyroid and Parathyroid Glands PDFDokument15 SeitenSonography of Normal and Abnormal Thyroid and Parathyroid Glands PDFJheyson Javier Barrios PereiraNoch keine Bewertungen
- Science 3 DLP 7 - Parts of The Skin and Their FunctionsDokument12 SeitenScience 3 DLP 7 - Parts of The Skin and Their FunctionsEmily DaymielNoch keine Bewertungen
- Biology NEET-11 EM: Chemical Control & Co-OrdinationDokument1 SeiteBiology NEET-11 EM: Chemical Control & Co-Ordinationnileshsaini2006Noch keine Bewertungen
- 123 Sur HypoparathyroidismDokument3 Seiten123 Sur HypoparathyroidismHurryNoch keine Bewertungen
- LEC 01 - Principles of EndocrinologyDokument44 SeitenLEC 01 - Principles of EndocrinologyIoana Cozma100% (1)
- Laporan PhyxioEx METEND - Rohid AlfazonDokument27 SeitenLaporan PhyxioEx METEND - Rohid AlfazonZayne GamingNoch keine Bewertungen
- Adrenal Gland 111Dokument28 SeitenAdrenal Gland 111Renz OrtegaNoch keine Bewertungen
- Anatomy and Physiology OvaryDokument6 SeitenAnatomy and Physiology OvaryFretchell Aripal MontesNoch keine Bewertungen
- CH 3 Form 5Dokument30 SeitenCH 3 Form 5Noor Amira RamliNoch keine Bewertungen
- Tyroid Drug - ppt3Dokument15 SeitenTyroid Drug - ppt3nurliah armandNoch keine Bewertungen
- Sinadinos Christa - Herbal Support For HypothyroidismDokument11 SeitenSinadinos Christa - Herbal Support For HypothyroidismDiah Siti FatimahNoch keine Bewertungen
- Diagnosis of HypothyroidismDokument10 SeitenDiagnosis of HypothyroidismHanzla IrfanNoch keine Bewertungen
- Thyroid Tietz Textbook 2012 PDFDokument21 SeitenThyroid Tietz Textbook 2012 PDFIvana BajunovicNoch keine Bewertungen
- Tulajabahvani StotrDokument2 SeitenTulajabahvani StotrHema DhaneNoch keine Bewertungen
- Puberty Below: Role of HormonesDokument3 SeitenPuberty Below: Role of HormonesCyril CauilanNoch keine Bewertungen
- Lesson Plan 2020-2021Dokument7 SeitenLesson Plan 2020-2021MELIE BAGARESNoch keine Bewertungen
- Diagestive, Urinary and Reproductive SystemDokument39 SeitenDiagestive, Urinary and Reproductive SystemCarolina Calle HerreraNoch keine Bewertungen
- Shashikant PDFDokument4 SeitenShashikant PDFAacharya Shashikant VashishthNoch keine Bewertungen
- Diagnosis and Treatment of Primary AldosteronismDokument17 SeitenDiagnosis and Treatment of Primary AldosteronismcastillojessNoch keine Bewertungen
- Sidney H. Ingbar (Editor), Sidney C. Werner (Editor) by Lippincott Williams & Wilkins PublishersDokument10 SeitenSidney H. Ingbar (Editor), Sidney C. Werner (Editor) by Lippincott Williams & Wilkins Publishersbyrock66Noch keine Bewertungen
- EndocrinologyDokument57 SeitenEndocrinologyeleonora rosaNoch keine Bewertungen
- Hypophysis CerebriDokument21 SeitenHypophysis CerebriAli Akand AsifNoch keine Bewertungen
- Disorders of The Endocrine SystemDokument84 SeitenDisorders of The Endocrine Systemcy lifeNoch keine Bewertungen
- Anatomy and PhysiologyDokument10 SeitenAnatomy and PhysiologyBurni GuevaraNoch keine Bewertungen
- Endocrine System Function and AssessmentDokument3 SeitenEndocrine System Function and Assessmentbomoore79Noch keine Bewertungen
- Ip Lot 40380Dokument1 SeiteIp Lot 40380MaherNoch keine Bewertungen
- CC Chatterjee's Human Physiology 12th Volume 2Dokument7 SeitenCC Chatterjee's Human Physiology 12th Volume 2food onNoch keine Bewertungen
- Hypopituitarism - ThomasDokument40 SeitenHypopituitarism - ThomasguidanceNoch keine Bewertungen