Das könnte Ihnen auch gefallen
- SOMATOM Definition As Operator Manual VB20x SAPEDM Definition-As-VB20A-Instructions-For-Use en 11432021.02Dokument644 SeitenSOMATOM Definition As Operator Manual VB20x SAPEDM Definition-As-VB20A-Instructions-For-Use en 11432021.02Ana Paula AlvesNoch keine Bewertungen
- Caring Design. Insightful Technology.: GE HealthcareDokument20 SeitenCaring Design. Insightful Technology.: GE HealthcareFunny Videos zNoch keine Bewertungen
- Environmental Product Declaration: SOMATOM Go - TopDokument11 SeitenEnvironmental Product Declaration: SOMATOM Go - TopStefan LaurentiuNoch keine Bewertungen
- Aperto LucentDokument2 SeitenAperto LucentnylashahidNoch keine Bewertungen
- SIMIND ManualDokument64 SeitenSIMIND ManualMariana CarvalhoNoch keine Bewertungen
- 0910 Prokop Cardiac CTDokument6 Seiten0910 Prokop Cardiac CTJohn RybackNoch keine Bewertungen
- Applicationguide Sensation10 Clinicalappl 1syngo 2006a 07-00209692Dokument196 SeitenApplicationguide Sensation10 Clinicalappl 1syngo 2006a 07-00209692Muhammad AhmadNoch keine Bewertungen
- Site Planning Siemens Biograph MCTDokument12 SeitenSite Planning Siemens Biograph MCTCarlos Larraín CastroNoch keine Bewertungen
- Magnetom Free - Max: From Concept To Product, A Brief History of The Drycool Magnet DevelopmentDokument5 SeitenMagnetom Free - Max: From Concept To Product, A Brief History of The Drycool Magnet DevelopmentVivien LenganiNoch keine Bewertungen
- MAGNETOM Symphony Tim Appl PacksDokument20 SeitenMAGNETOM Symphony Tim Appl PackshgaucherNoch keine Bewertungen
- Truebeam CollimationDokument6 SeitenTruebeam Collimationzhen yongjieNoch keine Bewertungen
- Syngo MR E11 OncoDokument64 SeitenSyngo MR E11 OncoLuís GuerraNoch keine Bewertungen
- ArcCHECK Reference Guide RevP JulyDokument248 SeitenArcCHECK Reference Guide RevP JulyGustavo Montalvo Ramírez100% (1)
- CT Acr 464 Phantom: Leverage A Sophisticated Design To Comply With Guidelines, and MoreDokument2 SeitenCT Acr 464 Phantom: Leverage A Sophisticated Design To Comply With Guidelines, and MoreRogelio Pérez Argüello50% (2)
- Elekta Versa HDDokument12 SeitenElekta Versa HDHaider RabeeNoch keine Bewertungen
- 736-424-G2 Varex NexusDR OperatorDokument304 Seiten736-424-G2 Varex NexusDR OperatorMariuszNoch keine Bewertungen
- Syngo MR E11 VascularDokument124 SeitenSyngo MR E11 VascularLuís GuerraNoch keine Bewertungen
- Corrective Maintenance Manual - Beam Physics System Elekta Digital Linear AcDokument189 SeitenCorrective Maintenance Manual - Beam Physics System Elekta Digital Linear AcQuyet PhungNoch keine Bewertungen
- Brochure CT Scan SOMATOM Perspective PDFDokument46 SeitenBrochure CT Scan SOMATOM Perspective PDFratna_fanoNoch keine Bewertungen
- 9 CT InstrumentationDokument72 Seiten9 CT InstrumentationYuda FhunkshyangNoch keine Bewertungen
- Siemens Somatom Sensation Cardiac A60 Users Manual 410406 PDFDokument128 SeitenSiemens Somatom Sensation Cardiac A60 Users Manual 410406 PDFronny sierraNoch keine Bewertungen
- AAPM 34 - MRI Acceptance TestDokument16 SeitenAAPM 34 - MRI Acceptance TestmahbodsedNoch keine Bewertungen
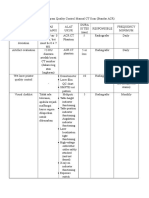
- Tabel QC CT ScanDokument6 SeitenTabel QC CT ScanbayuNoch keine Bewertungen
- Instruction Manual For Testing The Acr CT PhantomDokument16 SeitenInstruction Manual For Testing The Acr CT PhantomMuchti IndriyatiNoch keine Bewertungen
- MAMMOMAT 1000 / 3000 Nova: Universal Mammography System For Screening and DiagnosisDokument20 SeitenMAMMOMAT 1000 / 3000 Nova: Universal Mammography System For Screening and DiagnosisBartosz OgibowskiNoch keine Bewertungen
- Manual Medilink-90Dokument18 SeitenManual Medilink-90manuela HurtadoNoch keine Bewertungen
- Beam Quality Guidelines For TrueBeam-TrueBeam STx-EDGE-VitalBeamDokument18 SeitenBeam Quality Guidelines For TrueBeam-TrueBeam STx-EDGE-VitalBeamsenthilonco_21753387100% (1)
- RF-Amp S20 S21 Technical ManualDokument169 SeitenRF-Amp S20 S21 Technical ManualKIRILLNoch keine Bewertungen
- Plasma MRI Owner ManualDokument120 SeitenPlasma MRI Owner ManualNiteshNoch keine Bewertungen
- Synapse RIS Version 4-1Dokument46 SeitenSynapse RIS Version 4-1Oh Tiang HoeNoch keine Bewertungen
- CT B-iCT-64 BrochureDokument7 SeitenCT B-iCT-64 BrochureCao Minh TríNoch keine Bewertungen
- Huq CT SimulatorDokument65 SeitenHuq CT SimulatorEskadmas BelayNoch keine Bewertungen
- Brilliance iCT Confi GurationDokument12 SeitenBrilliance iCT Confi GurationpeymanNoch keine Bewertungen
- HTM Magazine PDFDokument68 SeitenHTM Magazine PDFcarlos duranNoch keine Bewertungen
- RSL-D-RS-7.0-SEG-EN-1.0-2017-12-08 RayStation 7 System Environment Guidelines PDFDokument42 SeitenRSL-D-RS-7.0-SEG-EN-1.0-2017-12-08 RayStation 7 System Environment Guidelines PDFAndres MoyaNoch keine Bewertungen
- FORM QC MRI AcceptTesting 0604Dokument4 SeitenFORM QC MRI AcceptTesting 0604Yuda FhunkshyangNoch keine Bewertungen
- Spesifikasi Siemens MRI AERA 1,5 TDokument2 SeitenSpesifikasi Siemens MRI AERA 1,5 TDr.gendjutNoch keine Bewertungen
- Supria 16 32 Brochure EN CP-414P EU Vers 2018 04Dokument9 SeitenSupria 16 32 Brochure EN CP-414P EU Vers 2018 04Ahmad AhmadNoch keine Bewertungen
- myQA Daily Users GuideDokument87 SeitenmyQA Daily Users GuideDaniela ZanchiNoch keine Bewertungen
- How and WhyDokument10 SeitenHow and WhyFauzan HerdianNoch keine Bewertungen
- Siemens Sensation CT ProtocolsDokument24 SeitenSiemens Sensation CT ProtocolsN AaNoch keine Bewertungen
- CT02-023 841 03 18 02Dokument163 SeitenCT02-023 841 03 18 02Ammar SaadNoch keine Bewertungen
- Synapse Mobility V. 7.1.3 User GuideDokument55 SeitenSynapse Mobility V. 7.1.3 User GuideOh Tiang HoeNoch keine Bewertungen
- MIM Service Manual v5 0Dokument374 SeitenMIM Service Manual v5 0Iranildo BarbosaNoch keine Bewertungen
- GEHealthcare Education TiP App Library CT AutomA SmartmA TheoryDokument5 SeitenGEHealthcare Education TiP App Library CT AutomA SmartmA Theoryfelix perezNoch keine Bewertungen
- Philips Azurion使用说明Dokument472 SeitenPhilips Azurion使用说明service iyadMedicalNoch keine Bewertungen
- 世界几大超声 (B超,彩超) 系统参数对比表格Dokument25 Seiten世界几大超声 (B超,彩超) 系统参数对比表格AnguschowNoch keine Bewertungen
- KKT Chillers PI ECO EngDokument2 SeitenKKT Chillers PI ECO EngjltenorioNoch keine Bewertungen
- Specification Z8Dokument17 SeitenSpecification Z8Radiologi JagakarsaNoch keine Bewertungen
- Manju Kiran.S: Presented ByDokument22 SeitenManju Kiran.S: Presented ByManju KiranNoch keine Bewertungen
- Toshiba Xario XG Yanamed PDFDokument6 SeitenToshiba Xario XG Yanamed PDFHassan bin QasimNoch keine Bewertungen
- Iacta 2011 Janak Mehta Award Winning PresentationDokument56 SeitenIacta 2011 Janak Mehta Award Winning PresentationDr.Sandeep Kumar KarNoch keine Bewertungen
- True Beam RTDokument33 SeitenTrue Beam RTdrpuneetseth4741Noch keine Bewertungen
- SUPRIA Vol61Dokument5 SeitenSUPRIA Vol61Dimas RiskyNoch keine Bewertungen
- Siemens CT - Low - Dose - GuideDokument66 SeitenSiemens CT - Low - Dose - GuideSyazwanee Nasir100% (1)
- Siemens Healthineers Somatom Go - All-Brochure IndiaDokument48 SeitenSiemens Healthineers Somatom Go - All-Brochure Indiadr_bassi100% (1)
- RayStation Brochure Ver3WEBDokument12 SeitenRayStation Brochure Ver3WEBSonik AlexNoch keine Bewertungen
- 3 D Abdominal OrgansDokument8 Seiten3 D Abdominal OrgansAndressa SilvaNoch keine Bewertungen
- Three-Dimensional Doppler Ultrasound in Gynecology: TechniqueDokument12 SeitenThree-Dimensional Doppler Ultrasound in Gynecology: Techniquesaeed hasan saeedNoch keine Bewertungen
- Clarity Viewer FeaturesDokument1 SeiteClarity Viewer FeaturesnikNoch keine Bewertungen
- Maya Technical Paper: How To Set Up and Optimise Alpha Planes When Using Mental Ray Tutorial KeyDokument12 SeitenMaya Technical Paper: How To Set Up and Optimise Alpha Planes When Using Mental Ray Tutorial KeyDayleSandersNoch keine Bewertungen
- DIP2 Image Enhancement1Dokument18 SeitenDIP2 Image Enhancement1Umar TalhaNoch keine Bewertungen
- Assignment 1 CV1 WS16/17: This Assignment Is Due On November 14th, 2016 at 12:00Dokument4 SeitenAssignment 1 CV1 WS16/17: This Assignment Is Due On November 14th, 2016 at 12:00Peter PanNoch keine Bewertungen
- Lecture 04Dokument32 SeitenLecture 04MaHedy AL HaSanNoch keine Bewertungen
- IS 2479 (1981) - Colour Code For The Identification of Aluminium and Aluminium Alloys For General Engineering PurposesDokument16 SeitenIS 2479 (1981) - Colour Code For The Identification of Aluminium and Aluminium Alloys For General Engineering Purposesprakashp111Noch keine Bewertungen
- Antialias Plugin TutorialDokument4 SeitenAntialias Plugin TutorialAbriel HaqqaniNoch keine Bewertungen
- Computed Tomography - An Overview: - Seeram: Chapter 1Dokument39 SeitenComputed Tomography - An Overview: - Seeram: Chapter 1kyuleen05Noch keine Bewertungen
- Mid Exam (Digital Image Processing)Dokument12 SeitenMid Exam (Digital Image Processing)Muhammad ShahzaibNoch keine Bewertungen
- Color TheorypdfDokument99 SeitenColor TheorypdfNews OffbeatNoch keine Bewertungen
- 5.discrete Wavelet Transform-Based Satellite Image Resolution EnhancementDokument8 Seiten5.discrete Wavelet Transform-Based Satellite Image Resolution EnhancementMenakha MohanNoch keine Bewertungen
- 5.VRAY FOR 3DSMAX (Sample Syllabus)Dokument3 Seiten5.VRAY FOR 3DSMAX (Sample Syllabus)Deepesh KumarNoch keine Bewertungen
- Image Compression TechniqueDokument18 SeitenImage Compression TechniqueNormaziah HanafiNoch keine Bewertungen
- Rajeev R Pillai Sarath J Pillai Nikhil S MenonDokument14 SeitenRajeev R Pillai Sarath J Pillai Nikhil S MenonRajeev R PillaiNoch keine Bewertungen
- Canon Printers Scanners Supplies Singapore Price List 2019Dokument34 SeitenCanon Printers Scanners Supplies Singapore Price List 2019Anchor Business & IT SolutionsNoch keine Bewertungen
- Cumulative Histogram EqualizationDokument14 SeitenCumulative Histogram EqualizationAnkit PrajapatiNoch keine Bewertungen
- Detection of Polycystic Ovary Syndrome From Ultrasound Images Using SIFT DescriptorsDokument5 SeitenDetection of Polycystic Ovary Syndrome From Ultrasound Images Using SIFT DescriptorsBONFRINGNoch keine Bewertungen
- Document Formats and Image Formats: James C. KingDokument32 SeitenDocument Formats and Image Formats: James C. Kingam30inNoch keine Bewertungen
- This Guide Is A Simple For The Illustration Produced During The Zbrush For Illustrators WorkshopDokument11 SeitenThis Guide Is A Simple For The Illustration Produced During The Zbrush For Illustrators WorkshopSebastián Crippa100% (2)
- LAB1Dokument7 SeitenLAB1Veera phanindraNoch keine Bewertungen
- Color Blind Painting Experience MethodolDokument5 SeitenColor Blind Painting Experience MethodolofFlickNoch keine Bewertungen
- LEE or PosterDokument1 SeiteLEE or Posterjavier_yosoyNoch keine Bewertungen
- Deblurring Text Images Via L - Regularized Intensity and Gradient PriorDokument8 SeitenDeblurring Text Images Via L - Regularized Intensity and Gradient PriorAsha simonNoch keine Bewertungen
- Daniel HailemichaelDokument108 SeitenDaniel HailemichaelHassenNoch keine Bewertungen
- Camcorder MiniDV ListDokument4 SeitenCamcorder MiniDV Listaurea_yansikuNoch keine Bewertungen
- Huffman Coding PaperDokument3 SeitenHuffman Coding Paperrohith4991Noch keine Bewertungen
- Ixell Catalogue 2018 PDFDokument89 SeitenIxell Catalogue 2018 PDFdan Paul67% (3)
- Image Resolution Guidelines - Nations Photo LabDokument4 SeitenImage Resolution Guidelines - Nations Photo LabPramod ShriwastavaNoch keine Bewertungen
- Assurance Ethics, Values & Good Governance Compress Edition PDFDokument216 SeitenAssurance Ethics, Values & Good Governance Compress Edition PDFanon_702955142Noch keine Bewertungen
- Amblyopia, A Multidisciplinary ApproachDokument161 SeitenAmblyopia, A Multidisciplinary ApproachTatianaGutuNoch keine Bewertungen
- The Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionVon EverandThe Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionBewertung: 4 von 5 Sternen4/5 (812)
- The Rise and Fall of the Dinosaurs: A New History of a Lost WorldVon EverandThe Rise and Fall of the Dinosaurs: A New History of a Lost WorldBewertung: 4 von 5 Sternen4/5 (597)
- Dark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseVon EverandDark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseBewertung: 3.5 von 5 Sternen3.5/5 (69)
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessVon EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessNoch keine Bewertungen
- Fire Season: Field Notes from a Wilderness LookoutVon EverandFire Season: Field Notes from a Wilderness LookoutBewertung: 4 von 5 Sternen4/5 (142)
- The Revolutionary Genius of Plants: A New Understanding of Plant Intelligence and BehaviorVon EverandThe Revolutionary Genius of Plants: A New Understanding of Plant Intelligence and BehaviorBewertung: 4.5 von 5 Sternen4.5/5 (137)
- The Best American Science And Nature Writing 2021Von EverandThe Best American Science And Nature Writing 2021Bewertung: 4 von 5 Sternen4/5 (8)
- When You Find Out the World Is Against You: And Other Funny Memories About Awful MomentsVon EverandWhen You Find Out the World Is Against You: And Other Funny Memories About Awful MomentsBewertung: 3.5 von 5 Sternen3.5/5 (13)
- World of Wonders: In Praise of Fireflies, Whale Sharks, and Other AstonishmentsVon EverandWorld of Wonders: In Praise of Fireflies, Whale Sharks, and Other AstonishmentsBewertung: 4 von 5 Sternen4/5 (223)
- Spoiled Rotten America: Outrages of Everyday LifeVon EverandSpoiled Rotten America: Outrages of Everyday LifeBewertung: 3 von 5 Sternen3/5 (19)
- The Other End of the Leash: Why We Do What We Do Around DogsVon EverandThe Other End of the Leash: Why We Do What We Do Around DogsBewertung: 5 von 5 Sternen5/5 (65)
- Come Back, Como: Winning the Heart of a Reluctant DogVon EverandCome Back, Como: Winning the Heart of a Reluctant DogBewertung: 3.5 von 5 Sternen3.5/5 (10)
- The Lives of Bees: The Untold Story of the Honey Bee in the WildVon EverandThe Lives of Bees: The Untold Story of the Honey Bee in the WildBewertung: 4.5 von 5 Sternen4.5/5 (44)
- The Hidden Life of Trees: What They Feel, How They CommunicateVon EverandThe Hidden Life of Trees: What They Feel, How They CommunicateBewertung: 4 von 5 Sternen4/5 (1003)
- Darwin's Doubt: The Explosive Origin of Animal Life and the Case for Intelligent DesignVon EverandDarwin's Doubt: The Explosive Origin of Animal Life and the Case for Intelligent DesignBewertung: 4 von 5 Sternen4/5 (19)
- Remnants of Ancient Life: The New Science of Old FossilsVon EverandRemnants of Ancient Life: The New Science of Old FossilsBewertung: 3 von 5 Sternen3/5 (3)
- The Soul of an Octopus: A Surprising Exploration into the Wonder of ConsciousnessVon EverandThe Soul of an Octopus: A Surprising Exploration into the Wonder of ConsciousnessBewertung: 4.5 von 5 Sternen4.5/5 (254)
- Ernst Haeckel's Art Forms in Nature: A Visual Masterpiece of the Natural WorldVon EverandErnst Haeckel's Art Forms in Nature: A Visual Masterpiece of the Natural WorldNoch keine Bewertungen
- Animals Make Us Human: Creating the Best Life for AnimalsVon EverandAnimals Make Us Human: Creating the Best Life for AnimalsBewertung: 4.5 von 5 Sternen4.5/5 (2)
- The Pleistocene Era: The History of the Ice Age and the Dawn of Modern HumansVon EverandThe Pleistocene Era: The History of the Ice Age and the Dawn of Modern HumansBewertung: 4 von 5 Sternen4/5 (5)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingVon EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingBewertung: 5 von 5 Sternen5/5 (5)
- Wayfinding: The Science and Mystery of How Humans Navigate the WorldVon EverandWayfinding: The Science and Mystery of How Humans Navigate the WorldBewertung: 4.5 von 5 Sternen4.5/5 (18)