Das könnte Ihnen auch gefallen
- Manual Aspiration Thrombectomy in Acute Myocardial Infarction: A Clinical ExperienceDokument9 SeitenManual Aspiration Thrombectomy in Acute Myocardial Infarction: A Clinical ExperienceArdiana FirdausNoch keine Bewertungen
- 4Dokument15 Seiten4savitageraNoch keine Bewertungen
- Anaesthesia 1Dokument9 SeitenAnaesthesia 1Sreekanth JangamNoch keine Bewertungen
- 02art8090web PDFDokument9 Seiten02art8090web PDFSyilla PriscilliaNoch keine Bewertungen
- Revista de RevistaDokument11 SeitenRevista de RevistaMiguel Angel Tipiani MallmaNoch keine Bewertungen
- Clinical Applications of High-Sensitivity Troponin Testing From Diagnosis To PrognosisDokument15 SeitenClinical Applications of High-Sensitivity Troponin Testing From Diagnosis To PrognosissunhaolanNoch keine Bewertungen
- Tactics 2001 NejmDokument9 SeitenTactics 2001 NejmGustavo Reyes QuezadaNoch keine Bewertungen
- Risk of Early Bleeding With Dual Antiplatelet Therapy in Acute Stroke and Transient Ischemic Attack Regardless of NIHSS AdmissionDokument6 SeitenRisk of Early Bleeding With Dual Antiplatelet Therapy in Acute Stroke and Transient Ischemic Attack Regardless of NIHSS AdmissionAhmad AnshoriNoch keine Bewertungen
- HHS Public AccessDokument19 SeitenHHS Public AccesssarahNoch keine Bewertungen
- 1.kamper Et al-2017-COHORT-Evaluation of Therapy and Management Outcome in Takotsubo SyndromeDokument9 Seiten1.kamper Et al-2017-COHORT-Evaluation of Therapy and Management Outcome in Takotsubo SyndromeHi GamingNoch keine Bewertungen
- Hypertension Arterielle 2016Dokument5 SeitenHypertension Arterielle 2016Nabil YahioucheNoch keine Bewertungen
- Eco in Cardiac Sugrery Anesthesic 1-s2.0-S1053077020305875-MainDokument11 SeitenEco in Cardiac Sugrery Anesthesic 1-s2.0-S1053077020305875-MainCésar Marriaga ZárateNoch keine Bewertungen
- 1 s2.0 S0929664617300487 MainDokument8 Seiten1 s2.0 S0929664617300487 MainSuryati HusinNoch keine Bewertungen
- Cardiac Myosin-Binding Protein C To Diagnose Acute Myocardial Infarction in The Pre-Hospital SettingDokument42 SeitenCardiac Myosin-Binding Protein C To Diagnose Acute Myocardial Infarction in The Pre-Hospital SettingSNoch keine Bewertungen
- HRT 09000902Dokument6 SeitenHRT 09000902boynextdoorpkyNoch keine Bewertungen
- AINES e Clinical OutcomesDokument23 SeitenAINES e Clinical Outcomesdiogofc123Noch keine Bewertungen
- Troponina predicción oclusión totalDokument5 SeitenTroponina predicción oclusión totalmanuel-gnNoch keine Bewertungen
- EMS Management of Acute Stroke-Prehospital Triage (Resource Document To NAEMSP Position Statement)Dokument6 SeitenEMS Management of Acute Stroke-Prehospital Triage (Resource Document To NAEMSP Position Statement)Allencia NauweNoch keine Bewertungen
- Identificacion Choque Cardiogenico ERDokument9 SeitenIdentificacion Choque Cardiogenico ERZai RojasNoch keine Bewertungen
- Withholding Versus Continuing Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Before Noncardiac SurgeryDokument12 SeitenWithholding Versus Continuing Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Before Noncardiac SurgerymomoNoch keine Bewertungen
- Main 10Dokument11 SeitenMain 10pokharelriwaj82Noch keine Bewertungen
- 15Dokument14 Seiten15savitageraNoch keine Bewertungen
- Ijmsv 14 P 1241Dokument10 SeitenIjmsv 14 P 1241Milan PetrikNoch keine Bewertungen
- In-Hospital Stroke Recurrence and Stroke After Transient Ischemic AttackDokument15 SeitenIn-Hospital Stroke Recurrence and Stroke After Transient Ischemic AttackferrevNoch keine Bewertungen
- Madit CRTNEJMseot 09Dokument10 SeitenMadit CRTNEJMseot 09binh doNoch keine Bewertungen
- Early Invasive Strategy For non-ST Elevation Acute Coronary Syndrome: A Meta-Analysis of Randomized, Controlled TrialsDokument13 SeitenEarly Invasive Strategy For non-ST Elevation Acute Coronary Syndrome: A Meta-Analysis of Randomized, Controlled TrialssavitageraNoch keine Bewertungen
- Heart J: Outcome of Primary Percutaneous Coronary Intervention With Early and Late ST Resolution - Earlier Is Better!Dokument6 SeitenHeart J: Outcome of Primary Percutaneous Coronary Intervention With Early and Late ST Resolution - Earlier Is Better!ayesha FalakNoch keine Bewertungen
- Archivos - CT Angiography Followed by InvasiveDokument10 SeitenArchivos - CT Angiography Followed by InvasiveGiselle LeonNoch keine Bewertungen
- J Jvca 2015 03 020Dokument6 SeitenJ Jvca 2015 03 020Andres Rojas JerezNoch keine Bewertungen
- Initial Diagnosis and Management of Acutely Elevated Intracranial PressureDokument8 SeitenInitial Diagnosis and Management of Acutely Elevated Intracranial PressureGlessin MurilloNoch keine Bewertungen
- Timing of Revascularization in Patients With Transient ST Segment Elevation Myocardial Infarction A Randomized Clinical TrialDokument9 SeitenTiming of Revascularization in Patients With Transient ST Segment Elevation Myocardial Infarction A Randomized Clinical TrialWelly WijayaNoch keine Bewertungen
- Transient Stemi PDFDokument9 SeitenTransient Stemi PDFsheilaNoch keine Bewertungen
- Initial Invasive or Conservative Strategy For Stable Coronary DiseaseDokument12 SeitenInitial Invasive or Conservative Strategy For Stable Coronary DiseaseDrMarcus KeyboardNoch keine Bewertungen
- 2013 - STEMI - Future Strategies - LancetDokument14 Seiten2013 - STEMI - Future Strategies - LancetMichail PapafaklisNoch keine Bewertungen
- Cardiac Troponins For The Diagnosis of Acute Myocardial Infarction in Chronic Kidney Disease PDFDokument24 SeitenCardiac Troponins For The Diagnosis of Acute Myocardial Infarction in Chronic Kidney Disease PDFDaniel Hernando Rodriguez PeraltaNoch keine Bewertungen
- Rory Hachamovitch, MD, MSC Sean W. Hayes, MD John D. Friedman, MD Ishac Cohen, PHD Daniel S. Berman, MDDokument8 SeitenRory Hachamovitch, MD, MSC Sean W. Hayes, MD John D. Friedman, MD Ishac Cohen, PHD Daniel S. Berman, MDFarah SukmanaNoch keine Bewertungen
- Cetin 2016Dokument10 SeitenCetin 2016Della Puspita SariNoch keine Bewertungen
- Fibrinolitik UnsratDokument7 SeitenFibrinolitik UnsratOtherside OfmeNoch keine Bewertungen
- 1 SM PDFDokument7 Seiten1 SM PDFNofri antsNoch keine Bewertungen
- 1-s2.0-S1071916423003068-mainDokument13 Seiten1-s2.0-S1071916423003068-mainevelyn.minichNoch keine Bewertungen
- Prospective Randomized Evaluation of Preoperative Angiotensin-Converting Enzyme Inhibition (PREOP-ACEI)Dokument7 SeitenProspective Randomized Evaluation of Preoperative Angiotensin-Converting Enzyme Inhibition (PREOP-ACEI)andiNoch keine Bewertungen
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDokument6 SeitenPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNoch keine Bewertungen
- Dogan 2012Dokument7 SeitenDogan 2012Davy JonesNoch keine Bewertungen
- Stenting Versus Aggressive Medical Therapy For Intracranial Arterial StenosisDokument11 SeitenStenting Versus Aggressive Medical Therapy For Intracranial Arterial StenosisariNoch keine Bewertungen
- Salim 2009Dokument6 SeitenSalim 2009raden chandrajaya listiandokoNoch keine Bewertungen
- Use of CT To Guide ManagementDokument10 SeitenUse of CT To Guide ManagementnatayaregizaNoch keine Bewertungen
- Chapter IDokument36 SeitenChapter INaily Nuzulur RohmahNoch keine Bewertungen
- Higher Troponin Levels Linked to Embolic StrokesDokument7 SeitenHigher Troponin Levels Linked to Embolic StrokesafbmgNoch keine Bewertungen
- Abstrak IsicamDokument22 SeitenAbstrak IsicambgusjklNoch keine Bewertungen
- Mortality Rates in Patients With ST-elevation vs. non-ST-elevation Acute Myocardial Infarction: Observations From An Unselected CohortDokument9 SeitenMortality Rates in Patients With ST-elevation vs. non-ST-elevation Acute Myocardial Infarction: Observations From An Unselected CohortsavitageraNoch keine Bewertungen
- biomedicines-11-00979Dokument10 Seitenbiomedicines-11-00979akinaNoch keine Bewertungen
- Randomized Trial of Primary PCI With or Without Routine Manual ThrombectomyDokument15 SeitenRandomized Trial of Primary PCI With or Without Routine Manual ThrombectomyTony Santos'sNoch keine Bewertungen
- Tumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupDokument5 SeitenTumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupMikhail PisarevNoch keine Bewertungen
- Race Ii 2010 NejmDokument11 SeitenRace Ii 2010 NejmAxel Hiram Hernandez PinedaNoch keine Bewertungen
- Case Series - Acute Coronary SyndromeDokument18 SeitenCase Series - Acute Coronary SyndromenikNoch keine Bewertungen
- Antiplatelet Discontinuation Practices in CAD Patients Undergoing SurgeryDokument2 SeitenAntiplatelet Discontinuation Practices in CAD Patients Undergoing SurgeryRakhmat RamadhaniNoch keine Bewertungen
- Acute Coronary Syndromes Without ST-Segment Elevation - What Is The Role of Early Intervention?Dokument3 SeitenAcute Coronary Syndromes Without ST-Segment Elevation - What Is The Role of Early Intervention?Rui FonteNoch keine Bewertungen
- Yamamoto Et Al 2019 Clinical and Laboratory Predictors For Plaque Erosion in Patients With Acute Coronary SyndromesDokument18 SeitenYamamoto Et Al 2019 Clinical and Laboratory Predictors For Plaque Erosion in Patients With Acute Coronary SyndromesMarcellia AngelinaNoch keine Bewertungen
- (19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeDokument7 Seiten(19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeRandy Reina RiveroNoch keine Bewertungen
- Acute Stroke Management in the Era of ThrombectomyVon EverandAcute Stroke Management in the Era of ThrombectomyEdgar A. SamaniegoNoch keine Bewertungen
- International Journal of Women's Dermatology: P.E. Grimes, MD, M.M. Miller, BSDokument6 SeitenInternational Journal of Women's Dermatology: P.E. Grimes, MD, M.M. Miller, BSSabariaNoch keine Bewertungen
- Bacterial Vaginosis: A Critical Analysis of Current KnowledgeDokument9 SeitenBacterial Vaginosis: A Critical Analysis of Current KnowledgeSabariaNoch keine Bewertungen
- KortikoDokument5 SeitenKortikoSabariaNoch keine Bewertungen
- Ejm 70893 Original Article YavuzDokument5 SeitenEjm 70893 Original Article YavuzSabariaNoch keine Bewertungen
- Bacterial Vaginosis: A Critical Analysis of Current KnowledgeDokument9 SeitenBacterial Vaginosis: A Critical Analysis of Current KnowledgeSabariaNoch keine Bewertungen
- 10 1111-1471-0528 14209figure142090001Dokument1 Seite10 1111-1471-0528 14209figure142090001SabariaNoch keine Bewertungen
- 10 1111-1471-0528 14209figure142090001Dokument1 Seite10 1111-1471-0528 14209figure142090001SabariaNoch keine Bewertungen
- Pityriasis Rosea An Update On Etiopathogenesis and Management of Difficult Aspects PDFDokument10 SeitenPityriasis Rosea An Update On Etiopathogenesis and Management of Difficult Aspects PDFketutwidakomalasariNoch keine Bewertungen
- Clinical and Molecular Aspects of Vitiligo TreatmentsDokument15 SeitenClinical and Molecular Aspects of Vitiligo TreatmentsSabariaNoch keine Bewertungen
- The Effect of Tinea Versicolor On Thioldisulphide PDFDokument5 SeitenThe Effect of Tinea Versicolor On Thioldisulphide PDFVera VebriNoch keine Bewertungen
- BPJ Vol 11 No 1 P 167-170Dokument5 SeitenBPJ Vol 11 No 1 P 167-170SabariaNoch keine Bewertungen
- Dermoscopic Pattern of Pityriasis Versicolor: Clinical, Cosmetic and Investigational Dermatology DoveDokument7 SeitenDermoscopic Pattern of Pityriasis Versicolor: Clinical, Cosmetic and Investigational Dermatology DoveSabariaNoch keine Bewertungen
- Determinants of Pityriasis Alba in Egyptian School ChildrenDokument7 SeitenDeterminants of Pityriasis Alba in Egyptian School ChildrenSabariaNoch keine Bewertungen
- Pityriasis Rosea: A Comprehensive ClassificationDokument13 SeitenPityriasis Rosea: A Comprehensive ClassificationaaNoch keine Bewertungen
- Etm 17 02 1039Dokument6 SeitenEtm 17 02 1039SabariaNoch keine Bewertungen
- Severe Herpes Zoster Following Varicella Vaccination in Immunocompetent Young ChildrenDokument5 SeitenSevere Herpes Zoster Following Varicella Vaccination in Immunocompetent Young ChildrenSabariaNoch keine Bewertungen
- Efusi PleuraDokument15 SeitenEfusi PleuraAnonymous KPhTy0CENoch keine Bewertungen
- Typhoid Fever: Clinical Presentation and Associated Factors in Febrile Patients Visiting Shashemene Referral Hospital, Southern EthiopiaDokument6 SeitenTyphoid Fever: Clinical Presentation and Associated Factors in Febrile Patients Visiting Shashemene Referral Hospital, Southern EthiopiaSabariaNoch keine Bewertungen
- Severe Herpes Zoster Following Varicella Vaccination in Immunocompetent Young ChildrenDokument5 SeitenSevere Herpes Zoster Following Varicella Vaccination in Immunocompetent Young ChildrenSabariaNoch keine Bewertungen
- Bacterial Vaginosis: A Critical Analysis of Current KnowledgeDokument1 SeiteBacterial Vaginosis: A Critical Analysis of Current KnowledgeSabariaNoch keine Bewertungen
- Zinc Deficiency in Children With Dengue Viral InfectionDokument5 SeitenZinc Deficiency in Children With Dengue Viral InfectionSabariaNoch keine Bewertungen
- Obesity in Individuals With Schizophrenia: A Case Controlled Study in ScotlandDokument3 SeitenObesity in Individuals With Schizophrenia: A Case Controlled Study in ScotlandSabariaNoch keine Bewertungen
- Sensitive Mirna Markers For The Detection and Management of Nstemi Acute Myocardial Infarction PatientsDokument10 SeitenSensitive Mirna Markers For The Detection and Management of Nstemi Acute Myocardial Infarction PatientsSabariaNoch keine Bewertungen
- International Journal of Women's Dermatology: P.E. Grimes, MD, M.M. Miller, BSDokument6 SeitenInternational Journal of Women's Dermatology: P.E. Grimes, MD, M.M. Miller, BSSabariaNoch keine Bewertungen
- Bacterial Vaginosis: A Critical Analysis of Current KnowledgeDokument9 SeitenBacterial Vaginosis: A Critical Analysis of Current KnowledgeSabariaNoch keine Bewertungen
- Chapter IIDokument6 SeitenChapter IISabariaNoch keine Bewertungen
- Zinc Deficiency in Children With Dengue Viral InfectionDokument5 SeitenZinc Deficiency in Children With Dengue Viral InfectionSabariaNoch keine Bewertungen
- PCI StrategyDokument14 SeitenPCI StrategyJason WinathaNoch keine Bewertungen
- Infectious Pleural Effusion Status and Treatment Progress: Wei Yang, Bo Zhang, Ze-Ming ZhangDokument10 SeitenInfectious Pleural Effusion Status and Treatment Progress: Wei Yang, Bo Zhang, Ze-Ming ZhangNengLukmanNoch keine Bewertungen
- Sensitive Mirna Markers For The Detection and Management of Nstemi Acute Myocardial Infarction PatientsDokument10 SeitenSensitive Mirna Markers For The Detection and Management of Nstemi Acute Myocardial Infarction PatientsSabariaNoch keine Bewertungen
- Echocardiogram Guide: Types, Procedure, ResultsDokument23 SeitenEchocardiogram Guide: Types, Procedure, ResultsKarl RobleNoch keine Bewertungen
- Approach To Patient With Dyspnea & Ankle Swellling: Dr. Mudhafar Barzani MBCHB, DM, PHD, FRCP Ass. Prof. in CardiologyDokument55 SeitenApproach To Patient With Dyspnea & Ankle Swellling: Dr. Mudhafar Barzani MBCHB, DM, PHD, FRCP Ass. Prof. in CardiologyDarawan MirzaNoch keine Bewertungen
- Aubf Lec Atn ScriptDokument1 SeiteAubf Lec Atn ScriptVince RomanoNoch keine Bewertungen
- Intensive Care Unit Arrhythmias: S.M. HollenbergDokument13 SeitenIntensive Care Unit Arrhythmias: S.M. HollenbergEvita FebriyantiNoch keine Bewertungen
- (Tips and Tricks) Shuvanan Ray - Tips and Tricks in Interventional Cardiology-Jaypee Brothers Medical Publishers (2015)Dokument204 Seiten(Tips and Tricks) Shuvanan Ray - Tips and Tricks in Interventional Cardiology-Jaypee Brothers Medical Publishers (2015)TRẦN VIẾT AN100% (1)
- Лекция 7Dokument76 SeitenЛекция 7ramtin malekshahiNoch keine Bewertungen
- ACLS 2015 Guidelines for Cardiac Arrest ManagementDokument13 SeitenACLS 2015 Guidelines for Cardiac Arrest ManagementI Gede Aditya100% (5)
- Pulmonary HypertensionDokument1 SeitePulmonary HypertensionSa KhunNoch keine Bewertungen
- 9 - Series 2022Dokument8 Seiten9 - Series 2022Vijay UNoch keine Bewertungen
- Acute Renal FailureDokument21 SeitenAcute Renal Failureاحمد الهاشميNoch keine Bewertungen
- Pathophysiology of ESRDDokument3 SeitenPathophysiology of ESRDjake90210100% (1)
- Assigning Patients After AngiographyDokument47 SeitenAssigning Patients After Angiographydotleds100% (1)
- (PCOL) Cardio and Renal Drugs - Test BankDokument20 Seiten(PCOL) Cardio and Renal Drugs - Test BankGriselle GomezNoch keine Bewertungen
- Epidemiology of Chronic Kidney Disease An U - 2022 - Kidney International SupplDokument5 SeitenEpidemiology of Chronic Kidney Disease An U - 2022 - Kidney International SupplSol anonimoNoch keine Bewertungen
- Lecture 3 PDFDokument24 SeitenLecture 3 PDFAya MuhannadNoch keine Bewertungen
- ECG Criteria to Distinguish Left vs. Right Ventricular Outflow Tract ArrhythmiasDokument8 SeitenECG Criteria to Distinguish Left vs. Right Ventricular Outflow Tract ArrhythmiasAbrudan GabrielNoch keine Bewertungen
- 1st, 2nd, 3rd Degree AV BLockDokument8 Seiten1st, 2nd, 3rd Degree AV BLockladydreamer_92Noch keine Bewertungen
- Viskin Et Al 2021 Polymorphic Ventricular Tachycardia Terminology Mechanism Diagnosis and Emergency TherapyDokument17 SeitenViskin Et Al 2021 Polymorphic Ventricular Tachycardia Terminology Mechanism Diagnosis and Emergency TherapyMey TalabessyNoch keine Bewertungen
- Rheumatic Fever and Heart DiseaseDokument30 SeitenRheumatic Fever and Heart DiseaseerikarobertNoch keine Bewertungen
- Acut Coronary SyndromeDokument65 SeitenAcut Coronary SyndromeArys SetiawanNoch keine Bewertungen
- Approach To Renal BiopsyDokument77 SeitenApproach To Renal BiopsySandeep Kumar VushikamallaNoch keine Bewertungen
- Acute Glomerulonephritis (AGN) Causes and SymptomsDokument25 SeitenAcute Glomerulonephritis (AGN) Causes and SymptomsAradhanaRamchandaniNoch keine Bewertungen
- CD Im PrimerDokument28 SeitenCD Im PrimerTiagogiesteiraNoch keine Bewertungen
- Aki & CKDDokument61 SeitenAki & CKDChengzhi KhorNoch keine Bewertungen
- What Causes Chronic Kidney Disease (CKD) ?Dokument4 SeitenWhat Causes Chronic Kidney Disease (CKD) ?siti fatmawatiNoch keine Bewertungen
- Systemic Hypertension Mechanisms and DiagnosisDokument40 SeitenSystemic Hypertension Mechanisms and DiagnosisChayagon MongkonsawatNoch keine Bewertungen
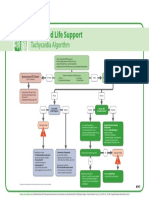
- Poster 10 ALS-TACH 01 01 ENG V20100927Dokument1 SeitePoster 10 ALS-TACH 01 01 ENG V20100927Andy XiaoNoch keine Bewertungen
- Diuretic Usage in Chronic Heart Failure PatientDokument1 SeiteDiuretic Usage in Chronic Heart Failure Patientmuh_alatas40Noch keine Bewertungen
- VVIR Vs DDDRDokument2 SeitenVVIR Vs DDDRNITACORDEIRONoch keine Bewertungen
- Pulmonary Atresia With An Intact Ventricular Septum: Preoperative Physiology, Imaging, and ManagementDokument12 SeitenPulmonary Atresia With An Intact Ventricular Septum: Preoperative Physiology, Imaging, and ManagementGusti Ayu Radhitia OctaviaNoch keine Bewertungen