Das könnte Ihnen auch gefallen
- Mesenteric TorsionDokument2 SeitenMesenteric TorsionEmerson SiqueiraNoch keine Bewertungen
- PIIS0749073923000184Dokument14 SeitenPIIS0749073923000184Allende Tellechea CarrilloNoch keine Bewertungen
- Single Incision, Laparoscopic-Assisted Ovariohysterectomy For Mucometra and Pyometra in DogsDokument5 SeitenSingle Incision, Laparoscopic-Assisted Ovariohysterectomy For Mucometra and Pyometra in Dogsalfi fadilah alfidruNoch keine Bewertungen
- Nueva Tec Ovh VacasDokument8 SeitenNueva Tec Ovh VacasAndres Luna MendezNoch keine Bewertungen
- Estudio Endoscopico-Patologico en Estenosis Pilorica Adquirida en GatosDokument8 SeitenEstudio Endoscopico-Patologico en Estenosis Pilorica Adquirida en GatosTatiana Ramirez SibocheNoch keine Bewertungen
- Ultrasound Assessment of Gastric Content and VolumeDokument8 SeitenUltrasound Assessment of Gastric Content and VolumeeryxspNoch keine Bewertungen
- Tema 4 - Artículo 1 - Santl 1998Dokument12 SeitenTema 4 - Artículo 1 - Santl 1998Nieves Anais Bustinza PahuaraNoch keine Bewertungen
- Surgical Treatment of Displaced Abomasum in Cattle Using Ljubljana MethodDokument8 SeitenSurgical Treatment of Displaced Abomasum in Cattle Using Ljubljana MethodIkhwanul KhairiaNoch keine Bewertungen
- Feline Abdominal Ultrasonography: What'S Normal? What'S Abnormal?Dokument8 SeitenFeline Abdominal Ultrasonography: What'S Normal? What'S Abnormal?Ветеринарная хирургия Dvm Тозлиян И. А.Noch keine Bewertungen
- Estimating The Outcome of Umbilical Diseases Based On Clinical Examination in Calves: 322 CasesDokument5 SeitenEstimating The Outcome of Umbilical Diseases Based On Clinical Examination in Calves: 322 CasesFathurrahman Maulana RifqiNoch keine Bewertungen
- Ocus - Group - On - Laparoscopic - Colectomy - Education - As - Endorsed - by - The - Ascrs - and - SagesDokument5 SeitenOcus - Group - On - Laparoscopic - Colectomy - Education - As - Endorsed - by - The - Ascrs - and - SagesIfeanyichukwu OgbonnayaNoch keine Bewertungen
- Barbosa 2013Dokument6 SeitenBarbosa 2013Letícia InamassuNoch keine Bewertungen
- Video Capsule EndosDokument3 SeitenVideo Capsule EndosRobert GodeanuNoch keine Bewertungen
- Role of Laparoscopy in Diagnosis and Management ofDokument11 SeitenRole of Laparoscopy in Diagnosis and Management ofAristoteles Esteban Cine VelazquezNoch keine Bewertungen
- Faciolasis PDFDokument6 SeitenFaciolasis PDFMuhammad FaridNoch keine Bewertungen
- 175 Ultrasound in Pregnancy PDFDokument16 Seiten175 Ultrasound in Pregnancy PDFNestor FerrerNoch keine Bewertungen
- Elipse Balloon The Pitfalls of Excessive SimplicityDokument3 SeitenElipse Balloon The Pitfalls of Excessive SimplicityTony Miguel Saba SabaNoch keine Bewertungen
- Laparoscopicdiagnosisofpancreaticdiseaseindogsandcats: C.B. Webb and C. TrottDokument4 SeitenLaparoscopicdiagnosisofpancreaticdiseaseindogsandcats: C.B. Webb and C. TrottElizabeth KezdamNoch keine Bewertungen
- International Journal of Surgery: ReviewDokument14 SeitenInternational Journal of Surgery: ReviewRizka Desti AyuniNoch keine Bewertungen
- Wriggley Ultrasound1 The Focused Assessment With Sonography For TraumaDokument5 SeitenWriggley Ultrasound1 The Focused Assessment With Sonography For TraumaCabinet VeterinarNoch keine Bewertungen
- Theriogenology: Elaine M.U. Gil, Daniela A.A. Garcia, Tilde R. FroesDokument6 SeitenTheriogenology: Elaine M.U. Gil, Daniela A.A. Garcia, Tilde R. FroesIngrid MachadoNoch keine Bewertungen
- EndoscopyNovianaetal2017JKH PDFDokument6 SeitenEndoscopyNovianaetal2017JKH PDFJuni ClaudiaNoch keine Bewertungen
- Dte 03 121Dokument5 SeitenDte 03 121Buntoro Indra DNoch keine Bewertungen
- Esmaeili 2010Dokument4 SeitenEsmaeili 2010asepNoch keine Bewertungen
- LeíomaDokument6 SeitenLeíomaStephanie OdriozolaNoch keine Bewertungen
- Contents - 2016 - Veterinary Clinics of North America Food Animal Practice PDFDokument4 SeitenContents - 2016 - Veterinary Clinics of North America Food Animal Practice PDFfelipeNoch keine Bewertungen
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsDokument5 Seiten(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752Noch keine Bewertungen
- 10 1155@2016@2632368Dokument12 Seiten10 1155@2016@2632368Ayu AmaliaNoch keine Bewertungen
- Comparison of Two Techniques For A Comprehensive Gut Histopathological Analysis: Swiss Roll Versus Intestine StripsDokument8 SeitenComparison of Two Techniques For A Comprehensive Gut Histopathological Analysis: Swiss Roll Versus Intestine StripsKX DigitalNoch keine Bewertungen
- Rumenotomy and Rumenostomy: Indications and OutcomesDokument3 SeitenRumenotomy and Rumenostomy: Indications and OutcomesPutraChaniagoNoch keine Bewertungen
- Chervier - FeverDokument4 SeitenChervier - FeverChristian De LeonNoch keine Bewertungen
- Viabilidad Fetal Bucca2005Dokument16 SeitenViabilidad Fetal Bucca2005kaathydanieelaNoch keine Bewertungen
- Reproduction in Domestic AnimalsVon EverandReproduction in Domestic AnimalsH. H. ColeNoch keine Bewertungen
- Couturier, Vru, 2012Dokument6 SeitenCouturier, Vru, 2012stylianos kontosNoch keine Bewertungen
- Wale 2016Dokument12 SeitenWale 2016Radiologi RSPDNoch keine Bewertungen
- Primary Abdominal Ectopic Pregnancy: A Case Report: Cases Journal August 2009Dokument5 SeitenPrimary Abdominal Ectopic Pregnancy: A Case Report: Cases Journal August 2009Sha AbdulaNoch keine Bewertungen
- Colic Surgery Recent Upda - 2023 - Veterinary Clinics of North America EquineDokument14 SeitenColic Surgery Recent Upda - 2023 - Veterinary Clinics of North America EquinediazsunshineNoch keine Bewertungen
- OHT Flank ApproachDokument6 SeitenOHT Flank ApproachMarinaJiménezNoch keine Bewertungen
- Volume Imaging in The Abdomen With Ultrasound: How We Do ItDokument7 SeitenVolume Imaging in The Abdomen With Ultrasound: How We Do Itlehoainam8744Noch keine Bewertungen
- Pancreas: Thomas G. Nyland - John S. MattoonDokument1 SeitePancreas: Thomas G. Nyland - John S. MattoonpedroNoch keine Bewertungen
- UltrasonographyDokument21 SeitenUltrasonographyChecko LatteNoch keine Bewertungen
- Diagnosis and Treatment of Ovarian Remnant Syndrome PDFDokument10 SeitenDiagnosis and Treatment of Ovarian Remnant Syndrome PDFIaSoftNoch keine Bewertungen
- Transplante de Intestino Delgado em Ratos Não-Isogênicos: Small Bowel Transplantation in Outbred RatsDokument7 SeitenTransplante de Intestino Delgado em Ratos Não-Isogênicos: Small Bowel Transplantation in Outbred RatsCLPHtheoryNoch keine Bewertungen
- 1 PBDokument6 Seiten1 PBrizalakbarsyaNoch keine Bewertungen
- Dayle, Vru, 2006Dokument5 SeitenDayle, Vru, 2006stylianos kontosNoch keine Bewertungen
- A Retrospective Study On Traumatic Diaphragmatic Hernias in CatsDokument6 SeitenA Retrospective Study On Traumatic Diaphragmatic Hernias in CatsjaciaraNoch keine Bewertungen
- ABRAVAS 5 de 9 - Hernandez Divers 2007 Liver BXDokument5 SeitenABRAVAS 5 de 9 - Hernandez Divers 2007 Liver BXCamilo SantanderNoch keine Bewertungen
- MKH2678 461a3f6710fullabstractDokument11 SeitenMKH2678 461a3f6710fullabstractAlbarido MuhammadNoch keine Bewertungen
- Ovarian Ultrasonography and Follow of Estrus in The Bitch and QueenDokument8 SeitenOvarian Ultrasonography and Follow of Estrus in The Bitch and QueenTere GarzónNoch keine Bewertungen
- Ovrio Salpingo Histerectomiavideolaparoscpicaemgatosdomsticos TcnicacomdoisportaisDokument6 SeitenOvrio Salpingo Histerectomiavideolaparoscpicaemgatosdomsticos TcnicacomdoisportaisDra MeiNoch keine Bewertungen
- Comparison of RX Us For Diagnosing Small-Intestinal Mechanical Obstruction in Vomiting DogsDokument8 SeitenComparison of RX Us For Diagnosing Small-Intestinal Mechanical Obstruction in Vomiting DogsVanesa CaceresNoch keine Bewertungen
- Laparohysterectomy Uterine: ImmunoefficiencyDokument2 SeitenLaparohysterectomy Uterine: ImmunoefficiencyAdheSeoNoch keine Bewertungen
- Jurnal USG Normal Babi Jantan (ULTRASOUND IMAGING OF THE SPLEEN, STOMACH, LIVER, KIDNEYS, BLADDER, AND PROSTATE IN PIGLETS (Sus Scrofa Domestica) )Dokument9 SeitenJurnal USG Normal Babi Jantan (ULTRASOUND IMAGING OF THE SPLEEN, STOMACH, LIVER, KIDNEYS, BLADDER, AND PROSTATE IN PIGLETS (Sus Scrofa Domestica) )ShintaNoch keine Bewertungen
- White 2015Dokument11 SeitenWhite 2015Flavio RibeiroNoch keine Bewertungen
- A Cog Practice Bulletin 175 Ultrasound in PregnancyDokument16 SeitenA Cog Practice Bulletin 175 Ultrasound in Pregnancyansel7Noch keine Bewertungen
- Diagnostic Ultrasonography in Cattle With Diseases of The Mammary GlandDokument8 SeitenDiagnostic Ultrasonography in Cattle With Diseases of The Mammary GlandJessica AlejandraNoch keine Bewertungen
- Laparoscopic Ovariectomy in Small AnimalsDokument9 SeitenLaparoscopic Ovariectomy in Small AnimalsIván A. P-BetancurtNoch keine Bewertungen
- ContentServer - Asp 9Dokument7 SeitenContentServer - Asp 9AlanGonzalezNoch keine Bewertungen
- Role of Early Ultrasound in Detecting Inflammatory Intestinal Disorders and Identifying Their Anatomical Location Within The Bowel - 2003Dokument8 SeitenRole of Early Ultrasound in Detecting Inflammatory Intestinal Disorders and Identifying Their Anatomical Location Within The Bowel - 2003Сергей СадовниковNoch keine Bewertungen
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDokument5 SeitenTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752Noch keine Bewertungen
- US Artifacts - University of ChicagoDokument101 SeitenUS Artifacts - University of Chicagoludiegues752Noch keine Bewertungen
- Formulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy CatsDokument8 SeitenFormulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy Catsludiegues752Noch keine Bewertungen
- Small Animal Abdominal Ultrasonography - The SpleenDokument9 SeitenSmall Animal Abdominal Ultrasonography - The Spleenludiegues752Noch keine Bewertungen
- Imaging Intestinal ObstructionDokument5 SeitenImaging Intestinal Obstructionludiegues752Noch keine Bewertungen
- Radiology Packet 5 Heart FailureDokument25 SeitenRadiology Packet 5 Heart Failureludiegues752Noch keine Bewertungen
- Radiology Packet 4 Cardiac EnlargementDokument28 SeitenRadiology Packet 4 Cardiac Enlargementludiegues752Noch keine Bewertungen
- Alterations in The SkinDokument9 SeitenAlterations in The Skinludiegues752Noch keine Bewertungen
- Radiology Packet 7 Congenital Cardiac DiseaseDokument27 SeitenRadiology Packet 7 Congenital Cardiac Diseaseludiegues752Noch keine Bewertungen
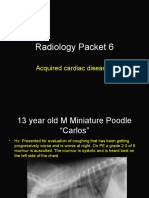
- Radiology Packet 6 Acquired Cardiac DiseasesDokument25 SeitenRadiology Packet 6 Acquired Cardiac Diseasesludiegues752Noch keine Bewertungen
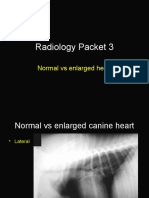
- Radiology Packet 3 Normal Vs Enlarged HeartDokument11 SeitenRadiology Packet 3 Normal Vs Enlarged Heartludiegues752Noch keine Bewertungen
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsDokument5 Seiten(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752Noch keine Bewertungen
- Case Report: Rapport de CasDokument4 SeitenCase Report: Rapport de Casludiegues752Noch keine Bewertungen
- The IntegumentDokument15 SeitenThe Integumentludiegues752Noch keine Bewertungen
- (2015) Basics of Equine DermatologyDokument10 Seiten(2015) Basics of Equine Dermatologyludiegues752Noch keine Bewertungen
- Spleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical EhrlichiosisDokument5 SeitenSpleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical Ehrlichiosisludiegues752Noch keine Bewertungen
- Derm History FormDokument1 SeiteDerm History Formludiegues752Noch keine Bewertungen
- (2015) Part 1 - Basics of Ultrasound Transducers & Image FormationDokument4 Seiten(2015) Part 1 - Basics of Ultrasound Transducers & Image Formationludiegues752Noch keine Bewertungen
- (2016) Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 1Dokument7 Seiten(2016) Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 1ludiegues752100% (1)
- Abdominal Ultrasonographic Findings Associated With Feline Infectious Peritonitis PDFDokument73 SeitenAbdominal Ultrasonographic Findings Associated With Feline Infectious Peritonitis PDFludiegues752Noch keine Bewertungen
- Ultrasonographic Differences Between Dogs and CatsDokument13 SeitenUltrasonographic Differences Between Dogs and Catsludiegues752Noch keine Bewertungen
- Ultrasound of The Thorax (Noncardiac)Dokument13 SeitenUltrasound of The Thorax (Noncardiac)ludiegues752Noch keine Bewertungen
- Nodular Fat Necrosis in The Feline and Canine AbdomenDokument5 SeitenNodular Fat Necrosis in The Feline and Canine Abdomenludiegues752Noch keine Bewertungen
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Dokument8 SeitenSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- Parasitology Case Presentation: Group 3Dokument42 SeitenParasitology Case Presentation: Group 3Christine Joy LegaspiNoch keine Bewertungen
- DictTheSwatowDialect FieldeDokument648 SeitenDictTheSwatowDialect FieldeKH QuahNoch keine Bewertungen
- The Excretory SystemDokument3 SeitenThe Excretory SystemMelvel John Nobleza AmarilloNoch keine Bewertungen
- Potasio 2015Dokument13 SeitenPotasio 2015Santiago Basto CruzNoch keine Bewertungen
- MaternityDokument91 SeitenMaternityAnonymous D8KswoNoch keine Bewertungen
- 05 06 Drawing CipDokument11 Seiten05 06 Drawing Cipapi-266268092Noch keine Bewertungen
- D&D 4E UnderdarkDokument161 SeitenD&D 4E UnderdarkNickTheRookie100% (6)
- History of NeuroscienceDokument17 SeitenHistory of NeurosciencerazorviperNoch keine Bewertungen
- Animal NutritionDokument6 SeitenAnimal NutritionMeily ZoelNoch keine Bewertungen
- Maham's Pre-Midterm Path NotesDokument190 SeitenMaham's Pre-Midterm Path NotesVishal100% (1)
- Pex 09 06Dokument4 SeitenPex 09 06Illich Ramirez Tanta100% (2)
- Combur 10 Test UX 11544373Dokument2 SeitenCombur 10 Test UX 11544373anon_65360249Noch keine Bewertungen
- Trabecular Hepatocellular Carcinoma in A DogDokument2 SeitenTrabecular Hepatocellular Carcinoma in A Dogpradeep. mampilliNoch keine Bewertungen
- Chapter 41, Pages 527-537: Transport of Oxygen and Carbon Dioxide in Blood and Tissue FluidsDokument46 SeitenChapter 41, Pages 527-537: Transport of Oxygen and Carbon Dioxide in Blood and Tissue FluidsAlia HaiderNoch keine Bewertungen
- Common Medical AbbriviationDokument13 SeitenCommon Medical AbbriviationADAMU LAWALNoch keine Bewertungen
- Perioperative Patient CareDokument6 SeitenPerioperative Patient CareClark LlameraNoch keine Bewertungen
- Pathology, Lecture 6 (Lecture Notes)Dokument18 SeitenPathology, Lecture 6 (Lecture Notes)Ali Al-Qudsi100% (1)
- The Circulatory System P2Dokument17 SeitenThe Circulatory System P2Kristal CampbellNoch keine Bewertungen
- Wednesday - Session A01 - Arello - Basic Suturing Skills and TechniquesDokument30 SeitenWednesday - Session A01 - Arello - Basic Suturing Skills and TechniquesSuresh Thapa ChhetriNoch keine Bewertungen
- Whooping Cough LectureDokument37 SeitenWhooping Cough LecturePriyanshu MNoch keine Bewertungen
- Wild Animals Reading Writing WorksheetDokument2 SeitenWild Animals Reading Writing WorksheetRRKATANoch keine Bewertungen
- (Vampire Library) Stuart A. Kallen - Vampire History and Lore-ReferencePoint Press (2011)Dokument80 Seiten(Vampire Library) Stuart A. Kallen - Vampire History and Lore-ReferencePoint Press (2011)Jerry KanneNoch keine Bewertungen
- 041 LiverDokument3 Seiten041 Liveraistina100% (1)
- Tula at Reviewer For PrintDokument14 SeitenTula at Reviewer For PrintMariejho GensayaNoch keine Bewertungen
- Nodal Stations of The AbdomenDokument8 SeitenNodal Stations of The Abdomenborst0% (1)
- Yoga Basics For Men PDFDokument47 SeitenYoga Basics For Men PDFfludor100% (1)
- Nursing Care Process Assessment Nursing Diagnosis ObjectiveDokument6 SeitenNursing Care Process Assessment Nursing Diagnosis ObjectiveKMNoch keine Bewertungen
- Assessment of The Ear, Nose and ThroatDokument40 SeitenAssessment of The Ear, Nose and Throatsnickers_j100% (3)
- GuppyDokument2 SeitenGuppymartynunez12345Noch keine Bewertungen
- Decalcifiying Pineal GlandDokument8 SeitenDecalcifiying Pineal Glandsonden_291% (11)