Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Small Animal Abdominal Ultrasonography - The SpleenDokument9 SeitenSmall Animal Abdominal Ultrasonography - The Spleenludiegues752Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDokument5 SeitenTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Radiology Packet 7 Congenital Cardiac DiseaseDokument27 SeitenRadiology Packet 7 Congenital Cardiac Diseaseludiegues752Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
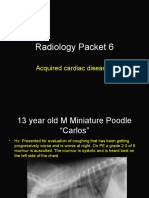
- Radiology Packet 6 Acquired Cardiac DiseasesDokument25 SeitenRadiology Packet 6 Acquired Cardiac Diseasesludiegues752Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Imaging Intestinal ObstructionDokument5 SeitenImaging Intestinal Obstructionludiegues752Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- (2012) Investigation and Management of Splenic Disease in DogsDokument8 Seiten(2012) Investigation and Management of Splenic Disease in Dogsludiegues752Noch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- (2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary MedicineDokument3 Seiten(2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary Medicineludiegues752Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Formulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy CatsDokument8 SeitenFormulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy Catsludiegues752Noch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- (2012) Investigation and Management of Splenic Disease in DogsDokument8 Seiten(2012) Investigation and Management of Splenic Disease in Dogsludiegues752Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- US Artifacts - University of ChicagoDokument101 SeitenUS Artifacts - University of Chicagoludiegues752Noch keine Bewertungen
- Radiology Packet 5: Heart Failure CasesDokument25 SeitenRadiology Packet 5: Heart Failure Casesludiegues752Noch keine Bewertungen
- Radiology Packet 4 Cardiac CasesDokument28 SeitenRadiology Packet 4 Cardiac Casesludiegues752Noch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- (2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary MedicineDokument3 Seiten(2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary Medicineludiegues752Noch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
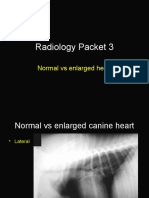
- Radiology Packet 3 Normal Vs Enlarged HeartDokument11 SeitenRadiology Packet 3 Normal Vs Enlarged Heartludiegues752Noch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- (2016) Ultrasonographic Features of Adrenal Gland Lesions in Dogs Can Aid in DiagnosisDokument9 Seiten(2016) Ultrasonographic Features of Adrenal Gland Lesions in Dogs Can Aid in Diagnosisludiegues752Noch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Ultrasonographic Evaluation of Adrenal Gland Size Compared To Body Weight in Normal DogsDokument10 SeitenUltrasonographic Evaluation of Adrenal Gland Size Compared To Body Weight in Normal Dogsludiegues752Noch keine Bewertungen
- (2017) Repetitive Ultrasonographic Assessment of Adrenal Size and Shape Changes - A Clue For An Asymptomatic Sex Hormone-Secreting AdenomaDokument5 Seiten(2017) Repetitive Ultrasonographic Assessment of Adrenal Size and Shape Changes - A Clue For An Asymptomatic Sex Hormone-Secreting Adenomaludiegues752Noch keine Bewertungen
- (2016) Associations Between Sex, Body Weight, Age, and US Determined Adrenal Thickness in Dogs With Non-Adrenal Gland IllnessDokument9 Seiten(2016) Associations Between Sex, Body Weight, Age, and US Determined Adrenal Thickness in Dogs With Non-Adrenal Gland Illnessludiegues752Noch keine Bewertungen
- (2016) Retrospective Study of Adrenal Gland US in Dogs With Normal and Abnormal ACTH Stimulation Test - Eric Lindquist PDFDokument6 Seiten(2016) Retrospective Study of Adrenal Gland US in Dogs With Normal and Abnormal ACTH Stimulation Test - Eric Lindquist PDFludiegues752Noch keine Bewertungen
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsDokument5 Seiten(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752Noch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The IntegumentDokument15 SeitenThe Integumentludiegues752Noch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- (2010) Ultrasonographic Evaluation of Adrenal Glands in Dogs With Primary Hypoadrenocorticism or Mimicking DiseasesDokument5 Seiten(2010) Ultrasonographic Evaluation of Adrenal Glands in Dogs With Primary Hypoadrenocorticism or Mimicking Diseasesludiegues752Noch keine Bewertungen
- Dermatology History FormDokument1 SeiteDermatology History Formludiegues752Noch keine Bewertungen
- Dog with Lung Mineralization from Steroid TherapyDokument4 SeitenDog with Lung Mineralization from Steroid Therapyludiegues752Noch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Alterations in The SkinDokument9 SeitenAlterations in The Skinludiegues752Noch keine Bewertungen
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Dokument8 SeitenSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- (1997) Ultrasonographic Adrenal Gland Measurements in Dogs Without Evidence of Adrenal DiseaseDokument7 Seiten(1997) Ultrasonographic Adrenal Gland Measurements in Dogs Without Evidence of Adrenal Diseaseludiegues752Noch keine Bewertungen
- (2015) Basics of Equine DermatologyDokument10 Seiten(2015) Basics of Equine Dermatologyludiegues752Noch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- (2012) Emerging Skin Conditions in CattleDokument9 Seiten(2012) Emerging Skin Conditions in Cattleludiegues752Noch keine Bewertungen
- Spleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical EhrlichiosisDokument5 SeitenSpleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical Ehrlichiosisludiegues752Noch keine Bewertungen
- IABPDokument88 SeitenIABPNavojit Chowdhury100% (1)
- TOP 5 Considerations for Anesthesia of a Geriatric PatientDokument5 SeitenTOP 5 Considerations for Anesthesia of a Geriatric PatientMabe AguirreNoch keine Bewertungen
- Di V V: Cardiomath Equations InfoDokument35 SeitenDi V V: Cardiomath Equations InfoMd. ashfaque Ahemmed khanNoch keine Bewertungen
- Abdominal Compartment Syndrome and Intra Abdominal.21 PDFDokument9 SeitenAbdominal Compartment Syndrome and Intra Abdominal.21 PDFFIA SlotNoch keine Bewertungen
- Funda ExamDokument17 SeitenFunda ExamMichael GustiloNoch keine Bewertungen
- General Appearance and Mental StatusDokument4 SeitenGeneral Appearance and Mental Statusmadamcloudnine100% (1)
- 2007 - Tu - Et - Al - 2007 - Revisiting The Relation Between Change and Initial ValueDokument15 Seiten2007 - Tu - Et - Al - 2007 - Revisiting The Relation Between Change and Initial ValueDanilo MoggiaNoch keine Bewertungen
- Case Study - Group2 - Semi FinalDokument41 SeitenCase Study - Group2 - Semi FinalKaye Marie MeloNoch keine Bewertungen
- Resuscitation Strategies For The Small Animal Trauma PatientDokument12 SeitenResuscitation Strategies For The Small Animal Trauma PatientCristhian Jover CastroNoch keine Bewertungen
- Chapter II: When To Use The Milk DietDokument11 SeitenChapter II: When To Use The Milk Dietgibrambo5770Noch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- BP 2017Dokument6 SeitenBP 2017Rafael MeloNoch keine Bewertungen
- Essential of Veterinary Surgery Venugopalan PDFDokument260 SeitenEssential of Veterinary Surgery Venugopalan PDFHassim M H S85% (34)
- Arterial Stiffness-1Dokument21 SeitenArterial Stiffness-1yoeldp100% (2)
- Biology Paper 1 November 1999Dokument30 SeitenBiology Paper 1 November 1999k391Noch keine Bewertungen
- Physical Fitness Readiness QuestionnaireDokument6 SeitenPhysical Fitness Readiness QuestionnaireMilbert Patun-ogNoch keine Bewertungen
- AP2 P3 Mar 2018 PDFDokument10 SeitenAP2 P3 Mar 2018 PDFkulsoomNoch keine Bewertungen
- Post Partum Depression Module 4Dokument11 SeitenPost Partum Depression Module 4Shean Y. LamosaoNoch keine Bewertungen
- Test For Two Relates SamplesDokument48 SeitenTest For Two Relates SamplesMiqz ZenNoch keine Bewertungen
- Antihypertensive Drugs.Dokument35 SeitenAntihypertensive Drugs.Abdul WahabNoch keine Bewertungen
- Colin BP S510 Patient Monitor User ManualDokument137 SeitenColin BP S510 Patient Monitor User ManualHussein MohamedNoch keine Bewertungen
- Medicare Review Finds Diets Ineffective Long TermDokument15 SeitenMedicare Review Finds Diets Ineffective Long TermRebecca ShaneNoch keine Bewertungen
- CMS Int. Med1 AnswersDokument15 SeitenCMS Int. Med1 AnswersDiego Al Gutierrez50% (2)
- Guyton and Hall Phisiology Textbook IndexDokument20 SeitenGuyton and Hall Phisiology Textbook Indexromila_ismail27% (15)
- Interact IIDokument7 SeitenInteract IIFitrah AfdhalNoch keine Bewertungen
- Nattokinase and Cardiovascular HealthDokument8 SeitenNattokinase and Cardiovascular HealthIhorNoch keine Bewertungen
- Jyotirmoy PathakDokument3 SeitenJyotirmoy PathakPankaj MaithaniNoch keine Bewertungen
- The Importance of Regular ExerciseDokument2 SeitenThe Importance of Regular ExerciseRedNoch keine Bewertungen
- New Drug HypertensionDokument23 SeitenNew Drug Hypertensiondwi kartikasariNoch keine Bewertungen
- Veterinary 3 Parameter Advisor Vital Signs MonitoDokument122 SeitenVeterinary 3 Parameter Advisor Vital Signs Monitosrgr2003Noch keine Bewertungen
- How To Control Hypertension (High Blood Pressure) - Nutrition StudiesDokument3 SeitenHow To Control Hypertension (High Blood Pressure) - Nutrition StudiesMatevž BrojanNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (402)