Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Sanjeevini All CardsDokument35 SeitenSanjeevini All Cardskwag83% (6)
- Saudi Council ExaminationDokument15 SeitenSaudi Council Examinationdedxdreamth95% (40)
- Abdominal Ultrasonographic Findings Associated With Feline Infectious Peritonitis PDFDokument73 SeitenAbdominal Ultrasonographic Findings Associated With Feline Infectious Peritonitis PDFludiegues752Noch keine Bewertungen
- (2015) Basics of Equine DermatologyDokument10 Seiten(2015) Basics of Equine Dermatologyludiegues752Noch keine Bewertungen
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Dokument8 SeitenSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- Nipah Virus: AN Emerging ThreatDokument11 SeitenNipah Virus: AN Emerging ThreatJayaraj RNoch keine Bewertungen
- Compendium Revised Jan 2018Dokument53 SeitenCompendium Revised Jan 2018Grace Membrebe100% (1)
- Formulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy CatsDokument8 SeitenFormulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy Catsludiegues752Noch keine Bewertungen
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDokument5 SeitenTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752Noch keine Bewertungen
- Small Animal Abdominal Ultrasonography - The SpleenDokument9 SeitenSmall Animal Abdominal Ultrasonography - The Spleenludiegues752Noch keine Bewertungen
- Radiology Packet 4 Cardiac EnlargementDokument28 SeitenRadiology Packet 4 Cardiac Enlargementludiegues752Noch keine Bewertungen
- Radiology Packet 5 Heart FailureDokument25 SeitenRadiology Packet 5 Heart Failureludiegues752Noch keine Bewertungen
- US Artifacts - University of ChicagoDokument101 SeitenUS Artifacts - University of Chicagoludiegues752Noch keine Bewertungen
- Imaging Intestinal ObstructionDokument5 SeitenImaging Intestinal Obstructionludiegues752Noch keine Bewertungen
- Case Report: Rapport de CasDokument4 SeitenCase Report: Rapport de Casludiegues752Noch keine Bewertungen
- Radiology Packet 7 Congenital Cardiac DiseaseDokument27 SeitenRadiology Packet 7 Congenital Cardiac Diseaseludiegues752Noch keine Bewertungen
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsDokument5 Seiten(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752Noch keine Bewertungen
- The IntegumentDokument15 SeitenThe Integumentludiegues752Noch keine Bewertungen
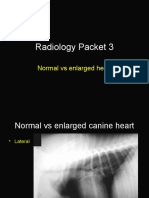
- Radiology Packet 3 Normal Vs Enlarged HeartDokument11 SeitenRadiology Packet 3 Normal Vs Enlarged Heartludiegues752Noch keine Bewertungen
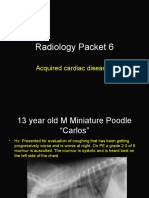
- Radiology Packet 6 Acquired Cardiac DiseasesDokument25 SeitenRadiology Packet 6 Acquired Cardiac Diseasesludiegues752Noch keine Bewertungen
- Alterations in The SkinDokument9 SeitenAlterations in The Skinludiegues752Noch keine Bewertungen
- Spleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical EhrlichiosisDokument5 SeitenSpleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical Ehrlichiosisludiegues752Noch keine Bewertungen
- Derm History FormDokument1 SeiteDerm History Formludiegues752Noch keine Bewertungen
- Nodular Fat Necrosis in The Feline and Canine AbdomenDokument5 SeitenNodular Fat Necrosis in The Feline and Canine Abdomenludiegues752Noch keine Bewertungen
- Ultrasonographic Differences Between Dogs and CatsDokument13 SeitenUltrasonographic Differences Between Dogs and Catsludiegues752Noch keine Bewertungen
- (2015) Part 1 - Basics of Ultrasound Transducers & Image FormationDokument4 Seiten(2015) Part 1 - Basics of Ultrasound Transducers & Image Formationludiegues752Noch keine Bewertungen
- Ultrasound of The Thorax (Noncardiac)Dokument13 SeitenUltrasound of The Thorax (Noncardiac)ludiegues752Noch keine Bewertungen
- (2016) Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 1Dokument7 Seiten(2016) Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 1ludiegues752100% (1)
- Daftar PustakaDokument2 SeitenDaftar PustakaAnonymous 65zjdAVNoch keine Bewertungen
- PSM Prep LadderDokument43 SeitenPSM Prep LadderMayanka SaxenaNoch keine Bewertungen
- Standard PrecautionsDokument20 SeitenStandard PrecautionspomiakhterNoch keine Bewertungen
- Lab Examination Parasitology UnibrawDokument40 SeitenLab Examination Parasitology UnibrawFaiz Fort Knox80% (5)
- Final Course RequirementDokument2 SeitenFinal Course RequirementJuliet ArdalesNoch keine Bewertungen
- Fraser Health: Health Authority Redesign AccomplishmentsDokument13 SeitenFraser Health: Health Authority Redesign AccomplishmentsStephen OlsonNoch keine Bewertungen
- Autoimmune Abnormalities of Postpartum Thyroid DiseasesDokument8 SeitenAutoimmune Abnormalities of Postpartum Thyroid DiseasesIpan MahendriyansaNoch keine Bewertungen
- Causes of Hearing LossDokument58 SeitenCauses of Hearing LossHalley MichelleNoch keine Bewertungen
- Concept Map of CKD Gastrointestinal SymptomsDokument4 SeitenConcept Map of CKD Gastrointestinal SymptomsWendy Escalante0% (1)
- Introduction To Waterborne PathogensDokument60 SeitenIntroduction To Waterborne PathogensSyed Alwi Alattas100% (1)
- PoliomyelitisDokument13 SeitenPoliomyelitiscasandra morante100% (2)
- Emerging Issues Report - Covid-19 and Social Development - FINAL - 24.9.2020 EditsDokument86 SeitenEmerging Issues Report - Covid-19 and Social Development - FINAL - 24.9.2020 EditsTanzia RahmanNoch keine Bewertungen
- Febrile SeizureDokument8 SeitenFebrile Seizureanon_944507650Noch keine Bewertungen
- Health Education Counseling Unit of Anemia in Pregnant WomenDokument6 SeitenHealth Education Counseling Unit of Anemia in Pregnant WomenNofri mansaNoch keine Bewertungen
- Clinical Tips Part - 1 PDFDokument4 SeitenClinical Tips Part - 1 PDFshclinic0% (1)
- Who Cds NTD Whopes GCDPP 2006.1 EngDokument125 SeitenWho Cds NTD Whopes GCDPP 2006.1 EngRohitNoch keine Bewertungen
- Chapter 1 Science Form 1Dokument19 SeitenChapter 1 Science Form 1Che SalNoch keine Bewertungen
- PAE044 Vulvovaginitis in Young GirlsDokument2 SeitenPAE044 Vulvovaginitis in Young GirlsFEBRYAN RAMADHANNoch keine Bewertungen
- CHN Post Test Students Copy NewDokument3 SeitenCHN Post Test Students Copy NewMeeKo Videña100% (1)
- Knowledge of Risk Factors and Preventive Practices Towards Domestic Fire Accidents Among Residents of Tanke Community in Ilorin, NigeriaDokument11 SeitenKnowledge of Risk Factors and Preventive Practices Towards Domestic Fire Accidents Among Residents of Tanke Community in Ilorin, NigeriaAnonymous izrFWiQNoch keine Bewertungen
- 2020-COR-TXT Planetary Emergency 2-0-Aug2020Dokument9 Seiten2020-COR-TXT Planetary Emergency 2-0-Aug2020Mika DeverinNoch keine Bewertungen
- Awareness of Dengue and Practice of Dengue Control Among1Dokument6 SeitenAwareness of Dengue and Practice of Dengue Control Among1rjohn 7Noch keine Bewertungen
- Dengue Annual Epidemiological Report 2018Dokument7 SeitenDengue Annual Epidemiological Report 2018b9738952Noch keine Bewertungen
- Post Parturent Haemoglobinuria.. 1112,1111,1113Dokument11 SeitenPost Parturent Haemoglobinuria.. 1112,1111,1113Na KhanNoch keine Bewertungen
- Ha CCP Document Record FormsDokument21 SeitenHa CCP Document Record FormsHotna Oktaria100% (1)
- Neonatal Sepsis Case 2Dokument81 SeitenNeonatal Sepsis Case 2Joanne Bernadette Aguilar100% (1)