Das könnte Ihnen auch gefallen
- Use of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaDokument10 SeitenUse of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaLingga AniNoch keine Bewertungen
- Bag-Mask Ventilation During Tracheal Intubation of Critically Ill AdultsDokument11 SeitenBag-Mask Ventilation During Tracheal Intubation of Critically Ill AdultsRitmaNoch keine Bewertungen
- Smith 2001Dokument19 SeitenSmith 2001PaulHerreraNoch keine Bewertungen
- Care of Newborn On Respiratory SupportDokument40 SeitenCare of Newborn On Respiratory SupportsyedNoch keine Bewertungen
- Invasive and Noninvasive Pediatric Mechanical Ventilation: Ira M Cheifetz MD FAARCDokument17 SeitenInvasive and Noninvasive Pediatric Mechanical Ventilation: Ira M Cheifetz MD FAARCAhmed Rizk AhmedNoch keine Bewertungen
- Complicaciones en El PreterminoDokument4 SeitenComplicaciones en El PreterminonadisjaviNoch keine Bewertungen
- How To Improve Intubation in The Intensive Care Unit. Update On Knowledge and DevicesDokument12 SeitenHow To Improve Intubation in The Intensive Care Unit. Update On Knowledge and DevicesMatheus HilárioNoch keine Bewertungen
- Hfo 3Dokument8 SeitenHfo 3markus_danusantosoNoch keine Bewertungen
- 07a2 PDFDokument6 Seiten07a2 PDFDiana Milena Poveda AriasNoch keine Bewertungen
- Jurnal RespirasiDokument12 SeitenJurnal RespirasiwilmaNoch keine Bewertungen
- Semler Et Al 2016Dokument8 SeitenSemler Et Al 2016Neneng VitriyahNoch keine Bewertungen
- BMV Critically IllDokument11 SeitenBMV Critically IllCLARINTA BELVA SABINANoch keine Bewertungen
- Evid TT 2200305Dokument4 SeitenEvid TT 2200305Muthia Farah AshmaNoch keine Bewertungen
- Anaesthesia - 2016 - Song - Effects of An Alveolar Recruitment Manoeuvre Guided by Lung Ultrasound On Anaesthesia InducedDokument10 SeitenAnaesthesia - 2016 - Song - Effects of An Alveolar Recruitment Manoeuvre Guided by Lung Ultrasound On Anaesthesia InducedAlexandra NemesNoch keine Bewertungen
- Anesthetic Implications of Zenker's Diverticulum: Somasundaram Thiagarajah, Erwin Lear, and Margaret KehDokument3 SeitenAnesthetic Implications of Zenker's Diverticulum: Somasundaram Thiagarajah, Erwin Lear, and Margaret KehMatthew JohnsonNoch keine Bewertungen
- Edwardus T. Adar 1308012050: Consultant Dr. Stef D. Soka, SP.BDokument21 SeitenEdwardus T. Adar 1308012050: Consultant Dr. Stef D. Soka, SP.BAlbert RanggaNoch keine Bewertungen
- PIIS1744165X23000677Dokument10 SeitenPIIS1744165X23000677crislatorreferNoch keine Bewertungen
- Role of PhysiotherapyDokument23 SeitenRole of PhysiotherapyVikas ChaitanyaNoch keine Bewertungen
- Bilat Ten Pneumo Improv 0214 p20 24Dokument5 SeitenBilat Ten Pneumo Improv 0214 p20 24juliusNoch keine Bewertungen
- Original Research Paper AnaesthesiologyDokument3 SeitenOriginal Research Paper AnaesthesiologySA SHNoch keine Bewertungen
- 693 FullDokument12 Seiten693 FullGilmer alvarez floresNoch keine Bewertungen
- A Radiological Perspective of Assessing Neonatal Respiratory Distress SyndromeDokument6 SeitenA Radiological Perspective of Assessing Neonatal Respiratory Distress Syndromeyoga zunandy pratamaNoch keine Bewertungen
- Falla VentilatoriaaaaaaaaDokument6 SeitenFalla VentilatoriaaaaaaaaDIANA CAROLINA OTALORA ALVAREZNoch keine Bewertungen
- Preoxygenation For Tracheal Intubation in Critically Ill Patients: One Technique Does Not Fit AllDokument5 SeitenPreoxygenation For Tracheal Intubation in Critically Ill Patients: One Technique Does Not Fit AllMarcela ParraNoch keine Bewertungen
- C 8 F 0 CF 2 F 9 C 13052842 DDokument11 SeitenC 8 F 0 CF 2 F 9 C 13052842 DDewi Ji YongNoch keine Bewertungen
- 22Dokument5 Seiten22Thasya RenaNoch keine Bewertungen
- ResuscitationDokument8 SeitenResuscitation85tq5nhsqbNoch keine Bewertungen
- RCT of Aprv Vs LPV in Ards PtsDokument11 SeitenRCT of Aprv Vs LPV in Ards PtsOldriana Prawiro HapsariNoch keine Bewertungen
- Articulo Tesis 9Dokument8 SeitenArticulo Tesis 9Lourdes MarcosNoch keine Bewertungen
- Review: Bronchoscopy During Noninvasive Ventilation: Indications and TechniqueDokument6 SeitenReview: Bronchoscopy During Noninvasive Ventilation: Indications and TechniqueJosé Luis Gutiérrez DomingoNoch keine Bewertungen
- Case Write Up Paeds FinalDokument3 SeitenCase Write Up Paeds Finaldonut258Noch keine Bewertungen
- Neonatal Tracheostomy - JonathanWalsh 2018Dokument12 SeitenNeonatal Tracheostomy - JonathanWalsh 2018Ismael Erazo AstudilloNoch keine Bewertungen
- Case Report - Spontaneous PneumomediastinumDokument6 SeitenCase Report - Spontaneous PneumomediastinumGhita ShupiyesaNoch keine Bewertungen
- E868 FullDokument10 SeitenE868 FullCalvin AffendyNoch keine Bewertungen
- Ventilation During Lung Resection and Critical Care ComparativeDokument11 SeitenVentilation During Lung Resection and Critical Care Comparativeema moralesNoch keine Bewertungen
- VM PediatrikDokument13 SeitenVM PediatrikWayan SupiartaNoch keine Bewertungen
- 2022-10# (PEERJ) RR in ECMODokument17 Seiten2022-10# (PEERJ) RR in ECMOjycntuNoch keine Bewertungen
- Lampiran Jurnal 1 PDFDokument7 SeitenLampiran Jurnal 1 PDFCyon Siiee D'javuNoch keine Bewertungen
- Anesthetic Management of Thoracoscopic Resection of Lung Lesions in Small ChildrenDokument8 SeitenAnesthetic Management of Thoracoscopic Resection of Lung Lesions in Small ChildrenburhanNoch keine Bewertungen
- Como Optimizar La EntubaciónDokument4 SeitenComo Optimizar La EntubaciónKaren Aline Gómez CruzNoch keine Bewertungen
- Wormald2009kandidat 2Dokument4 SeitenWormald2009kandidat 2adeNoch keine Bewertungen
- Chest Physiotherapy in Children With Acute Bacterial PneumoniaDokument10 SeitenChest Physiotherapy in Children With Acute Bacterial PneumoniaEka BagaskaraNoch keine Bewertungen
- 1 s2.0 S0733862722000384 MainDokument13 Seiten1 s2.0 S0733862722000384 Maincoca12451Noch keine Bewertungen
- Clinical Risk Factors Associated With Extubation Failure in Ventilated NeonatesDokument4 SeitenClinical Risk Factors Associated With Extubation Failure in Ventilated NeonatesMALIK MANASRAHNoch keine Bewertungen
- Secuencia de Intubación RápidaDokument16 SeitenSecuencia de Intubación Rápidaalis_maNoch keine Bewertungen
- Acute Laryngitis in ChildhoodDokument6 SeitenAcute Laryngitis in ChildhoodpinanoeNoch keine Bewertungen
- A Prospective, Randomized Study of Ventilator-Associated Pneumonia in Patients Using A Closed vs. Open Suction SystemDokument6 SeitenA Prospective, Randomized Study of Ventilator-Associated Pneumonia in Patients Using A Closed vs. Open Suction SystemYur Yenova ChavezNoch keine Bewertungen
- The Physiologically Difficult Airway: Eview RticleDokument9 SeitenThe Physiologically Difficult Airway: Eview RticleEdson Llerena SalvoNoch keine Bewertungen
- Journal English Hcu AnggrekDokument6 SeitenJournal English Hcu AnggrekUmbu Njebi KarambuNoch keine Bewertungen
- Wa0042.Dokument4 SeitenWa0042.ENFERMERIA EMERGENCIANoch keine Bewertungen
- Japplphysiol 00119 2021Dokument12 SeitenJapplphysiol 00119 2021Fernando Dinamarca SotoNoch keine Bewertungen
- WID MeaslesDokument30 SeitenWID MeaslesArvind KanagaratnamNoch keine Bewertungen
- Jama Thille 2019Dokument11 SeitenJama Thille 2019Fermin LombardiaNoch keine Bewertungen
- Difficult Airway Management in The Intensive Care UnitDokument10 SeitenDifficult Airway Management in The Intensive Care UnitcedivadeniaNoch keine Bewertungen
- Symposium Papers: Emergency Airway ManagementDokument10 SeitenSymposium Papers: Emergency Airway Managementdewin21Noch keine Bewertungen
- Pneumothorax Classification and Etiology: Clinics in Chest Medicine November 2021Dokument18 SeitenPneumothorax Classification and Etiology: Clinics in Chest Medicine November 2021DesyaNoch keine Bewertungen
- Anesthesia in Prehospital Emergencies and in The Emergency DepartmentDokument7 SeitenAnesthesia in Prehospital Emergencies and in The Emergency DepartmentIvan TapiaNoch keine Bewertungen
- Freid 2005Dokument14 SeitenFreid 2005PaulHerreraNoch keine Bewertungen
- EXPRESS Trial 2008Dokument10 SeitenEXPRESS Trial 2008Dr. Sergio Oscar AlunniNoch keine Bewertungen
- Review Article: Prevention of Dementia: Focus On LifestyleDokument9 SeitenReview Article: Prevention of Dementia: Focus On LifestyleRitmaNoch keine Bewertungen
- Strategies For Dementia Prevention: Latest Evidence and ImplicationsDokument16 SeitenStrategies For Dementia Prevention: Latest Evidence and ImplicationsRitmaNoch keine Bewertungen
- Completed Audit Cycle To Explore The Use of The STOPP/START Toolkit To Optimise Medication in Psychiatric In-Patients With DementiaDokument5 SeitenCompleted Audit Cycle To Explore The Use of The STOPP/START Toolkit To Optimise Medication in Psychiatric In-Patients With DementiaRitmaNoch keine Bewertungen
- Effects of Physical Activity During Pregnancy On Neonatal Birth WeightDokument8 SeitenEffects of Physical Activity During Pregnancy On Neonatal Birth WeightRitmaNoch keine Bewertungen
- Nlex 1Dokument4 SeitenNlex 1Aileen AlphaNoch keine Bewertungen
- A Concise Guide To Endodontic Procedures (9783662437292)Dokument198 SeitenA Concise Guide To Endodontic Procedures (9783662437292)ava parham100% (2)
- Nurs FPX 4020 Assessment 3 Improvement Plan in Service PresentationDokument6 SeitenNurs FPX 4020 Assessment 3 Improvement Plan in Service Presentationzadem5266Noch keine Bewertungen
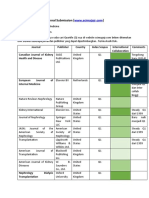
- Journal SubmissionDokument3 SeitenJournal SubmissionMaruhum Bonar MarbunNoch keine Bewertungen
- Overview of Ebola VirusDokument30 SeitenOverview of Ebola VirusJean Paolo RodriguezNoch keine Bewertungen
- Surgical Periodontal TherapyDokument11 SeitenSurgical Periodontal TherapyGonzalo Becerra LeonartNoch keine Bewertungen
- Case Studies in Nursing FundamentalsDokument393 SeitenCase Studies in Nursing FundamentalsBeverly Lavilla100% (1)
- Rielle Bioethics AssDokument7 SeitenRielle Bioethics Assdrae syNoch keine Bewertungen
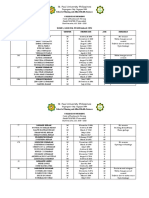
- St. Paul University Philippines: School of Nursing and Allied Health SciencesDokument12 SeitenSt. Paul University Philippines: School of Nursing and Allied Health SciencesKarina MadriagaNoch keine Bewertungen
- Ho, Jessica Y. 2013 "Mortality Under Age 50 Accounts For Much of The Fact That US Life Expectancy Lags That of Other High-Income Countries PDFDokument10 SeitenHo, Jessica Y. 2013 "Mortality Under Age 50 Accounts For Much of The Fact That US Life Expectancy Lags That of Other High-Income Countries PDFTengiz VerulavaNoch keine Bewertungen
- Eatern Equatoria State PresentationDokument24 SeitenEatern Equatoria State PresentationMayom MabuongNoch keine Bewertungen
- Approaches To Diagnosis Celiac DiseaseDokument16 SeitenApproaches To Diagnosis Celiac DiseaseJunior GrobeNoch keine Bewertungen
- Tooth Enamel DefectsDokument2 SeitenTooth Enamel DefectschamposNoch keine Bewertungen
- Minute AprilDokument3 SeitenMinute Aprilmzahir95Noch keine Bewertungen
- Common Non-Communicable DiseasesDokument28 SeitenCommon Non-Communicable DiseasesDanica AdamosNoch keine Bewertungen
- Guadiana & Okashima, 2020)Dokument3 SeitenGuadiana & Okashima, 2020)Jenina Marinelle AndresNoch keine Bewertungen
- Indian JOurnal of PediatricsDokument8 SeitenIndian JOurnal of Pediatricsliska ramdanawatiNoch keine Bewertungen
- Pay As Little As: Savings ProgramDokument1 SeitePay As Little As: Savings ProgramelasticemperorNoch keine Bewertungen
- Moawya Abu-Rashed: ObjectiveDokument3 SeitenMoawya Abu-Rashed: ObjectiveMoawya H. Abu RashedNoch keine Bewertungen
- System Generated MerDokument2 SeitenSystem Generated MerSyan ApuyanNoch keine Bewertungen
- Bulletproof Cannabis PrescribingDokument30 SeitenBulletproof Cannabis PrescribingstonerhinoNoch keine Bewertungen
- Week 8 HI-2 Intensive Care UnitDokument82 SeitenWeek 8 HI-2 Intensive Care UnitPaul Shan GoNoch keine Bewertungen
- Old New Herbal RemediesDokument76 SeitenOld New Herbal RemediesBrijesh Verma50% (2)
- Icao Health-Related DocumentsDokument30 SeitenIcao Health-Related DocumentsVitor Hugo FreitasNoch keine Bewertungen
- The Quality Improvement Customers Didn'T Want: Presented byDokument16 SeitenThe Quality Improvement Customers Didn'T Want: Presented bybbejasmine9541Noch keine Bewertungen
- Clinical Research AssociateDokument3 SeitenClinical Research Associateapi-77229440Noch keine Bewertungen
- Disease Outbreak InvestigationDokument4 SeitenDisease Outbreak Investigationkoass100% (1)
- Meningitis - 2018Dokument55 SeitenMeningitis - 2018Abraham Anaely100% (1)
- Airway 19 9 11Dokument49 SeitenAirway 19 9 11SiddharthNoch keine Bewertungen
- JCSO 2021 ReviewDokument67 SeitenJCSO 2021 ReviewENoch keine Bewertungen
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainVon EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainBewertung: 4 von 5 Sternen4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedBewertung: 4 von 5 Sternen4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (60)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (45)