Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Icog Membership FormDokument2 SeitenIcog Membership FormDrDevdatt Laxman PitaleNoch keine Bewertungen
- Natboard-Data Publicnotice Notice 202305033312Dokument7 SeitenNatboard-Data Publicnotice Notice 202305033312DrDevdatt Laxman PitaleNoch keine Bewertungen
- Chicken Pox in Pregnancy - A Challenge To The Obstetrician: Hem Kanta SarmaDokument2 SeitenChicken Pox in Pregnancy - A Challenge To The Obstetrician: Hem Kanta SarmaDrDevdatt Laxman PitaleNoch keine Bewertungen
- SAcervical CancerDokument12 SeitenSAcervical CancerDrDevdatt Laxman PitaleNoch keine Bewertungen
- Devdatt AncDokument31 SeitenDevdatt AncDrDevdatt Laxman PitaleNoch keine Bewertungen
- DR Devdatt Laxman Pitale, Consultant Obstetrician and Gynaecologist, High Risk Preganancy and ReproductiveDokument31 SeitenDR Devdatt Laxman Pitale, Consultant Obstetrician and Gynaecologist, High Risk Preganancy and ReproductiveDrDevdatt Laxman PitaleNoch keine Bewertungen
- Ectopic PregnancyDokument9 SeitenEctopic Pregnancysaleemut3Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Drug Use in Paeds and ElderlyDokument27 SeitenDrug Use in Paeds and ElderlyCuthbert Tinotenda MusarurwaNoch keine Bewertungen
- Integrative Behavioral Health Screening Tools and Resource ListDokument19 SeitenIntegrative Behavioral Health Screening Tools and Resource ListSkawnger SaluperNoch keine Bewertungen
- Larynx, Trachea, Lung and PleuraDokument60 SeitenLarynx, Trachea, Lung and PleuraKatNoch keine Bewertungen
- Preoperative Physiology, Imaging, andDokument13 SeitenPreoperative Physiology, Imaging, andSiLfia SahrinNoch keine Bewertungen
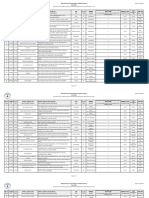
- Jadwal Preventive Maintenance Dan Kalibrasi External Peralatan Medik 2017Dokument100 SeitenJadwal Preventive Maintenance Dan Kalibrasi External Peralatan Medik 2017Ari RandaNoch keine Bewertungen
- Budson - Memory Loss, Alzheimer's Disease, and Dementia - 2 Ed - 2015Dokument283 SeitenBudson - Memory Loss, Alzheimer's Disease, and Dementia - 2 Ed - 2015Nathaly Cantor100% (3)
- Bowa Cat 10764 Electrosurgery Complete 2019 02 15 de en FR Es ItDokument208 SeitenBowa Cat 10764 Electrosurgery Complete 2019 02 15 de en FR Es Itinstrumed_globalNoch keine Bewertungen
- Rapha Exam (35 MKS)Dokument2 SeitenRapha Exam (35 MKS)TumabangNoch keine Bewertungen
- Preventing Disease Through Healthy Environments - Towards An Estimate of The Environmental Burden of DiseaseDokument105 SeitenPreventing Disease Through Healthy Environments - Towards An Estimate of The Environmental Burden of DiseaseZahara GatraNoch keine Bewertungen
- Meropenem Drug StudyDokument2 SeitenMeropenem Drug StudyKullin Rain100% (1)
- Respondent t10Dokument19 SeitenRespondent t10shreeyasingh0929Noch keine Bewertungen
- Pulmonology Techniques Breakthrough by Slidesgo 2Dokument33 SeitenPulmonology Techniques Breakthrough by Slidesgo 2BEATRIZ MACEDO VALADÃONoch keine Bewertungen
- BCBR Mcqs BookDokument211 SeitenBCBR Mcqs Bookzafrul islam100% (2)
- A Case For Psychiatric Leadership in Dispositional Capacity AssessmentDokument3 SeitenA Case For Psychiatric Leadership in Dispositional Capacity AssessmentRicardo EscNoch keine Bewertungen
- Gynecology Case HistoryDokument12 SeitenGynecology Case HistorySomNoch keine Bewertungen
- Cryptosporidiosis in ChickensDokument7 SeitenCryptosporidiosis in ChickensŠhâh NawazNoch keine Bewertungen
- TP - Getting Through Methamphetamine WithdrawalDokument2 SeitenTP - Getting Through Methamphetamine WithdrawalElizabeth GauntNoch keine Bewertungen
- NURS4060 - AshleyVigne - Assessment 4 - Attempt1Dokument7 SeitenNURS4060 - AshleyVigne - Assessment 4 - Attempt1ashleyNoch keine Bewertungen
- Q1 Las Health10 Module1 WK1 - 2Dokument10 SeitenQ1 Las Health10 Module1 WK1 - 2bonzai guillenaNoch keine Bewertungen
- Prepaid PlansDokument27 SeitenPrepaid PlansDee ReyesNoch keine Bewertungen
- WHO MDR 2020 Handbook Treatment PDFDokument88 SeitenWHO MDR 2020 Handbook Treatment PDFYuanita GunawanNoch keine Bewertungen
- Health Hazards of Chemicals Commonly Used On Military BasesDokument35 SeitenHealth Hazards of Chemicals Commonly Used On Military Basesmale nurseNoch keine Bewertungen
- Microbiology and Parasitology HandoutsDokument5 SeitenMicrobiology and Parasitology HandoutsJudy BaguiwenNoch keine Bewertungen
- Report 8b3a3101Dokument11 SeitenReport 8b3a3101Pooja AgarwalNoch keine Bewertungen
- Proximexa Suspension and Tablets GDS Version 25Dokument18 SeitenProximexa Suspension and Tablets GDS Version 25Masud l NazmulNoch keine Bewertungen
- KLSC BDU Kuwait Healthcare Report 2019 VF PDFDokument16 SeitenKLSC BDU Kuwait Healthcare Report 2019 VF PDFJim MacaoNoch keine Bewertungen
- PDEA S Register 2-14 FormDokument12 SeitenPDEA S Register 2-14 FormAngelito BALUYOT JRNoch keine Bewertungen
- NUTRILITE Apple Jujube WheatPeptide enDokument27 SeitenNUTRILITE Apple Jujube WheatPeptide enNoris Eka Raudzah IshakNoch keine Bewertungen
- MLSP111 PDF 03 - Professional Organizations PAMET PASMETH Schools of MTDokument6 SeitenMLSP111 PDF 03 - Professional Organizations PAMET PASMETH Schools of MTANGELICA ROMAWAKNoch keine Bewertungen
- Spondilitis TBDokument14 SeitenSpondilitis TBaswad 0008Noch keine Bewertungen