Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Online Web Chat Application DocumentDokument8 SeitenOnline Web Chat Application DocumentENGINEER HERENoch keine Bewertungen
- Group 1 Nondigital Instructional MaterialsDokument22 SeitenGroup 1 Nondigital Instructional MaterialsJhon Paul Esplanada Soriano100% (1)
- Digital Citizenship E-Portfolio AssignmentDokument4 SeitenDigital Citizenship E-Portfolio AssignmentJordanne ChristieNoch keine Bewertungen
- Loads Dead Loads Imposed Loads Floor Roof Determining Load Per M and m2 WindDokument58 SeitenLoads Dead Loads Imposed Loads Floor Roof Determining Load Per M and m2 Windwaheedopple3998Noch keine Bewertungen
- Learning Centered AssDokument4 SeitenLearning Centered AssNica Rowena Bacani CajimatNoch keine Bewertungen
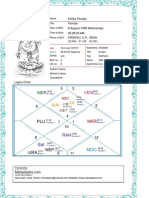
- Kritika Pandey (Kaushambi)Dokument15 SeitenKritika Pandey (Kaushambi)nishink9Noch keine Bewertungen
- Understanding Work Conditioning and Work Hardening Programs For A Successful RTW 3 13 2014 NovaCare PDFDokument37 SeitenUnderstanding Work Conditioning and Work Hardening Programs For A Successful RTW 3 13 2014 NovaCare PDFSitiSarah0% (1)
- Belajar Bahasa Spanyol PDFDokument5 SeitenBelajar Bahasa Spanyol PDFHimawan PrasojoNoch keine Bewertungen
- Breaking Into The Movies: Public Pedagogy and The Politics of FilmDokument10 SeitenBreaking Into The Movies: Public Pedagogy and The Politics of FilmDouglasNoch keine Bewertungen
- Cover Page and CertificateDokument34 SeitenCover Page and CertificateSello HlabeliNoch keine Bewertungen
- Tech Bull 3 - Free Fall of ConcreteDokument4 SeitenTech Bull 3 - Free Fall of ConcreteJoel TorcuatorNoch keine Bewertungen
- Assessment #1 StatisticsDokument4 SeitenAssessment #1 StatisticsjemimaNoch keine Bewertungen
- Types of Machine DrawingDokument19 SeitenTypes of Machine DrawingAmexTesfayeKora100% (5)
- EC9560 Data Mining: Lab 02: Classification and Prediction Using WEKADokument5 SeitenEC9560 Data Mining: Lab 02: Classification and Prediction Using WEKAkeethanNoch keine Bewertungen
- NRB Bank ReportDokument49 SeitenNRB Bank ReportTanvirBariNoch keine Bewertungen
- Mil STD 1316e Fuze DesignDokument25 SeitenMil STD 1316e Fuze Designscorpion_l_81Noch keine Bewertungen
- 9348 26140 1 PBDokument8 Seiten9348 26140 1 PBALIS TEBALNoch keine Bewertungen
- Autodesk Navisworks 2012 - Guia Do UsuárioDokument820 SeitenAutodesk Navisworks 2012 - Guia Do UsuárioericfgNoch keine Bewertungen
- The Ethics of Consumer Protection & Marketing: Ecture YnopsisDokument6 SeitenThe Ethics of Consumer Protection & Marketing: Ecture Ynopsiskuashask2Noch keine Bewertungen
- BehaviourDokument16 SeitenBehaviourIshita JainNoch keine Bewertungen
- INGOLD, Tim. Perceiving The EnviromentDokument15 SeitenINGOLD, Tim. Perceiving The EnviromentCassiana Oliveira da SilvaNoch keine Bewertungen
- Local Level Financial Systems: A Study On Three Union at Sylhet Sadar Upazilla in BangladeshDokument10 SeitenLocal Level Financial Systems: A Study On Three Union at Sylhet Sadar Upazilla in BangladeshTriple A Research Journal of Social Science and HumanityNoch keine Bewertungen
- Chebyshevs Inequality - ProblemspdfDokument6 SeitenChebyshevs Inequality - ProblemspdfamreenNoch keine Bewertungen
- Shortcut To English CollocationDokument240 SeitenShortcut To English Collocationtiago90% (10)
- C Test Questions and Answers PDFDokument15 SeitenC Test Questions and Answers PDFVikas Bakoliya100% (1)
- Starbucks and Free TradeDokument9 SeitenStarbucks and Free TradeSandraPauwelsNoch keine Bewertungen
- Fallacy - Philosophy Grade 11Dokument17 SeitenFallacy - Philosophy Grade 11leila vesagasNoch keine Bewertungen
- Curriculam Vite: ObjectiveDokument3 SeitenCurriculam Vite: ObjectiveSonyNoch keine Bewertungen
- TABLE: Concrete Column Summary - IS 456-2000 Story Label Unique Name Design Section Station Design/Check Status PMM RatioDokument3 SeitenTABLE: Concrete Column Summary - IS 456-2000 Story Label Unique Name Design Section Station Design/Check Status PMM Rationaveenpnaidu1Noch keine Bewertungen
- BSBINews 78Dokument96 SeitenBSBINews 78Anonymous dEztzVueNoch keine Bewertungen