Das könnte Ihnen auch gefallen
- LDTDokument6 SeitenLDTRaian SuyuNoch keine Bewertungen
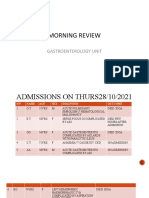
- MR GastroDokument31 SeitenMR GastroAdefuye AbiolaNoch keine Bewertungen
- LAPKAS-Elsa Nur Rahma Diahnissa-2016730030-1Dokument34 SeitenLAPKAS-Elsa Nur Rahma Diahnissa-2016730030-1Raka WibisonoNoch keine Bewertungen
- POMR PakDhe R26HCU - NHL+Septic Condition+Febril Neutropenia+Hematoscezia - CINV+Anemi+Trombocytopenia+HypoalbuminDokument42 SeitenPOMR PakDhe R26HCU - NHL+Septic Condition+Febril Neutropenia+Hematoscezia - CINV+Anemi+Trombocytopenia+HypoalbuminPramudia DeniNoch keine Bewertungen
- Clinical Portfolio Name: Armeen Amin ENROLLMENT NO. 4-4/2019/001 BSCN Year Ii Group A Faculty Name: Ms. Roma JosephDokument15 SeitenClinical Portfolio Name: Armeen Amin ENROLLMENT NO. 4-4/2019/001 BSCN Year Ii Group A Faculty Name: Ms. Roma JosephArmeen AminNoch keine Bewertungen
- Hashimotos ThyroiditisDokument9 SeitenHashimotos ThyroiditisKristiannlae DanoNoch keine Bewertungen
- Acute Pancreatitis Case PresDokument29 SeitenAcute Pancreatitis Case Preskristine keen buanNoch keine Bewertungen
- Delayed Emergence in Post Anesthesia Care Unit (Pacu) : Achmed RizalDokument15 SeitenDelayed Emergence in Post Anesthesia Care Unit (Pacu) : Achmed RizalAdikurniawanNoch keine Bewertungen
- MR Neng Meta ParuDokument15 SeitenMR Neng Meta Paruazraeni_629166196Noch keine Bewertungen
- Jaga Tengah - MedCon - 010321 - CAMDokument22 SeitenJaga Tengah - MedCon - 010321 - CAMAdinda DianNoch keine Bewertungen
- Stroke by K. NusrithaDokument13 SeitenStroke by K. NusrithaSai SharathNoch keine Bewertungen
- Case Conference Saturday Morning Shift, MAY 18, 2019Dokument39 SeitenCase Conference Saturday Morning Shift, MAY 18, 2019Aisya FikritamaNoch keine Bewertungen
- CC 18 Mei 19 HidrocephalusDokument50 SeitenCC 18 Mei 19 HidrocephalusAisya FikritamaNoch keine Bewertungen
- MR Konsul Sangkala PPOKDokument14 SeitenMR Konsul Sangkala PPOKazraeni_629166196Noch keine Bewertungen
- REV POMR KIPI SatyaDokument20 SeitenREV POMR KIPI SatyaDoctoRides 46Noch keine Bewertungen
- The PatientDokument9 SeitenThe PatientJan Crizza Dale R. FrancoNoch keine Bewertungen
- Morning: Friday, 6 March 2020Dokument17 SeitenMorning: Friday, 6 March 2020Herka PutraNoch keine Bewertungen
- Clinical Confrence: Neurology Division (New Case)Dokument20 SeitenClinical Confrence: Neurology Division (New Case)Sukma SusantiNoch keine Bewertungen
- POMR FAH BAshori CMLDokument22 SeitenPOMR FAH BAshori CMLIka AyuNoch keine Bewertungen
- Intraoperatively Inadequate BlockMORBIDITY ProtocolDokument9 SeitenIntraoperatively Inadequate BlockMORBIDITY Protocoldocv526Noch keine Bewertungen
- MR Muh. Arafah TB (Autosaved)Dokument14 SeitenMR Muh. Arafah TB (Autosaved)tiarapolarisiriuzNoch keine Bewertungen
- Case Study 1Dokument3 SeitenCase Study 1Ayman NabilNoch keine Bewertungen
- PCC CaseDokument9 SeitenPCC CaseKaila AbeledaNoch keine Bewertungen
- Morning Report: Monday, 8 May 2017Dokument25 SeitenMorning Report: Monday, 8 May 2017HarisNoch keine Bewertungen
- Clinical Abstract (2nd Sem 1st Rotation)Dokument3 SeitenClinical Abstract (2nd Sem 1st Rotation)Michael Gino SarenasNoch keine Bewertungen
- Brain AbscessDokument45 SeitenBrain AbscessAnanda AsmaraNoch keine Bewertungen
- Ahmad Basori VidiDokument30 SeitenAhmad Basori VidiIka AyuNoch keine Bewertungen
- Pharmacotherapeutics - I: Case Study On Anterior Wall Myocardial InfarctionDokument20 SeitenPharmacotherapeutics - I: Case Study On Anterior Wall Myocardial InfarctionDr. Suba Senthil0% (1)
- 14 MR Er Krs RDG ZakDokument15 Seiten14 MR Er Krs RDG Zaktriska antonyNoch keine Bewertungen
- DepartmentDokument7 SeitenDepartmentmubarek abdurohemanNoch keine Bewertungen
- Febrile SeizureDokument14 SeitenFebrile Seizuredk.clinicalresearchNoch keine Bewertungen
- Flail Chest MP Shah - CcuDokument29 SeitenFlail Chest MP Shah - CcuMARTINNoch keine Bewertungen
- Shock SepticDokument35 SeitenShock SepticAkbar SyarialNoch keine Bewertungen
- Grand Rounds: Roxanne Jeen L. Fornolles, M.DDokument61 SeitenGrand Rounds: Roxanne Jeen L. Fornolles, M.DRj FornollesNoch keine Bewertungen
- 6.19.07 Nephrology Board Review ShahDokument57 Seiten6.19.07 Nephrology Board Review Shahactidwell0% (1)
- Grand Round Case Presentation: by DR Sanjay Khare MD MedicineDokument19 SeitenGrand Round Case Presentation: by DR Sanjay Khare MD MedicineHrishikeshNoch keine Bewertungen
- Mortality by YvonneDokument25 SeitenMortality by YvonneYvonne SiiloNoch keine Bewertungen
- Morning Report: Physician in ChargeDokument29 SeitenMorning Report: Physician in ChargeWilujeng AnggrainiNoch keine Bewertungen
- Vincent Brody Care PlanDokument10 SeitenVincent Brody Care PlanKarina Rodriguez50% (2)
- Pedia Census ArrythmiaDokument48 SeitenPedia Census ArrythmiaBhi-An BatobalonosNoch keine Bewertungen
- History Taking General DataDokument5 SeitenHistory Taking General DatapjulyeNoch keine Bewertungen
- Lapsus Cardio v3Dokument31 SeitenLapsus Cardio v3Nurfitrianti ArfahNoch keine Bewertungen
- Ob Case 3 ChartDokument6 SeitenOb Case 3 ChartSteffiNoch keine Bewertungen
- Ca - CacaoDokument2 SeitenCa - CacaoISRAEL JULIANO SALGADONoch keine Bewertungen
- Laporan Jaga 11 Sep (English) KoreksiDokument30 SeitenLaporan Jaga 11 Sep (English) KoreksiArick Frendi AndriyanNoch keine Bewertungen
- Karapitiya OSCE 2017 With AnswersDokument34 SeitenKarapitiya OSCE 2017 With Answersweerawarna fernandoNoch keine Bewertungen
- Case No 37Dokument5 SeitenCase No 37Aila GoliasNoch keine Bewertungen
- Foreign BobyDokument29 SeitenForeign BobyAbhilasha Singh PanwarNoch keine Bewertungen
- Remon CovidDokument13 SeitenRemon CovidJuli2022 Semnol-SemsaNoch keine Bewertungen
- Sample Case ScenarioDokument8 SeitenSample Case ScenarioJan Crizza Dale R. FrancoNoch keine Bewertungen
- MR Kasa Hydropneumothorax EditedDokument17 SeitenMR Kasa Hydropneumothorax Editedazraeni_629166196Noch keine Bewertungen
- Wa0024Dokument25 SeitenWa0024sujarot dwiNoch keine Bewertungen
- CMC Cns Infection 2023Dokument5 SeitenCMC Cns Infection 2023Juan RecyNoch keine Bewertungen
- NC Rara HemaDokument18 SeitenNC Rara HemaDodi DiNoch keine Bewertungen
- ACUTE AND CHRONIC PANCREATITIS-undoneDokument6 SeitenACUTE AND CHRONIC PANCREATITIS-undonecory kurdapyaNoch keine Bewertungen
- Nursing Process 3Dokument10 SeitenNursing Process 3Shubhra Sheoran100% (1)
- CPC Protocol 2022Dokument4 SeitenCPC Protocol 2022Brian AtencionNoch keine Bewertungen
- A 12 Years Old 6 Months Girl With Eritema Ec Drug Eruption, All HR Pro Chemotherapy Week 9, Obs Fever Day 4, Oral MucositisDokument10 SeitenA 12 Years Old 6 Months Girl With Eritema Ec Drug Eruption, All HR Pro Chemotherapy Week 9, Obs Fever Day 4, Oral MucositisramotNoch keine Bewertungen
- Case Report Case ReportDokument18 SeitenCase Report Case ReportMelly MirandaNoch keine Bewertungen
- Choanal AtresiaDokument8 SeitenChoanal AtresiaDantowaluyo NewNoch keine Bewertungen
- Oral Surgery Benign Cysts P.2Dokument33 SeitenOral Surgery Benign Cysts P.2abbasmazaal1234Noch keine Bewertungen
- List of - EctomiesDokument4 SeitenList of - EctomiesASIF AL MAHMOODNoch keine Bewertungen
- Patient Safety 2020 PDFDokument1 SeitePatient Safety 2020 PDFxxdissuNoch keine Bewertungen
- Simple Technique For Lip and Nasolabial Fold Anesthesia For Injectable FillersDokument3 SeitenSimple Technique For Lip and Nasolabial Fold Anesthesia For Injectable FillersGina CastilloNoch keine Bewertungen
- Plastic Surgery Benefits and DisadvantagesDokument2 SeitenPlastic Surgery Benefits and DisadvantagesDana HamdaniNoch keine Bewertungen
- Wall ChartDokument2 SeitenWall ChartAhmed Fittoh Mosallam0% (1)
- Clinical Practice Guidelines For The Management of Cataract Among AdultsDokument16 SeitenClinical Practice Guidelines For The Management of Cataract Among AdultstvmedicineNoch keine Bewertungen
- Cardiac Arrest After Cardiac Surgery: An Evidence-Based Resuscitation ProtocolDokument12 SeitenCardiac Arrest After Cardiac Surgery: An Evidence-Based Resuscitation ProtocoljoseNoch keine Bewertungen
- Ico Oscar SicsDokument5 SeitenIco Oscar Sicsbrahmani pitanatriNoch keine Bewertungen
- LML 6002 Task 2Dokument9 SeitenLML 6002 Task 2hind.ausNoch keine Bewertungen
- History of SurgeryDokument22 SeitenHistory of SurgeryPrachi KharatmalNoch keine Bewertungen
- Nanorobots in Cancer TreatmentDokument4 SeitenNanorobots in Cancer TreatmentEditor IJTSRDNoch keine Bewertungen
- Recent Final Frca Vascular Anaesthesia QuestionsDokument4 SeitenRecent Final Frca Vascular Anaesthesia Questionslim sjNoch keine Bewertungen
- Star Health and Allied Insurance Company Limited IRDA Regn - No.129Dokument12 SeitenStar Health and Allied Insurance Company Limited IRDA Regn - No.129ng28Noch keine Bewertungen
- Operasi MetodeDokument4 SeitenOperasi MetodeImam S BluesNoch keine Bewertungen
- 2016 - Optimal Perioperative Management of The Geriatric PatientDokument18 Seiten2016 - Optimal Perioperative Management of The Geriatric PatientruthchristinawibowoNoch keine Bewertungen
- MixDokument1.789 SeitenMixIrvan VeryadiNoch keine Bewertungen
- Surgical Approaches To The Facial Skeleton 3rd Edition Ebook PDFDokument47 SeitenSurgical Approaches To The Facial Skeleton 3rd Edition Ebook PDFmary.burklow183100% (38)
- Up CHC 2016Dokument12 SeitenUp CHC 2016tajesh rajNoch keine Bewertungen
- Hysterectomy: EditorsDokument1.595 SeitenHysterectomy: EditorsHạnh Lê Hoàng Mỹ100% (1)
- Ozone IIMKozhikode Shashank SainiDokument11 SeitenOzone IIMKozhikode Shashank Sainishashank sainiNoch keine Bewertungen
- Basic Perioperative Nursing Skills Check ListDokument37 SeitenBasic Perioperative Nursing Skills Check Listradisid100% (2)
- DFGHDokument6 SeitenDFGHManuelEduardoSanchezSotoNoch keine Bewertungen
- 4 Amputation Nursing Care Plans - Nurseslabs-1 PDFDokument12 Seiten4 Amputation Nursing Care Plans - Nurseslabs-1 PDFsaidi MwanamongaNoch keine Bewertungen
- Siopel 4 Protocol 1Dokument156 SeitenSiopel 4 Protocol 1Caballero X CaballeroNoch keine Bewertungen
- Handbook On Field Veterinary Surgery (VetBooks - Ir) PDFDokument141 SeitenHandbook On Field Veterinary Surgery (VetBooks - Ir) PDFguadasampaioNoch keine Bewertungen
- Unit - 1. Overview of BiomaterialsDokument33 SeitenUnit - 1. Overview of Biomaterialsronaldo magarNoch keine Bewertungen
- DR Abdul Kalam - President of India Speech at Medical ConferenceDokument7 SeitenDR Abdul Kalam - President of India Speech at Medical ConferenceSibia SukhbindarNoch keine Bewertungen
- Surgery Case Presentation: Surgical Correction of Teat Fistula in GoatDokument15 SeitenSurgery Case Presentation: Surgical Correction of Teat Fistula in GoatSanjay KumarNoch keine Bewertungen