Das könnte Ihnen auch gefallen
- Cwu 1 OrthoDokument14 SeitenCwu 1 OrthoHakimah K. Suhaimi100% (1)
- Total Abdominal Hysterectomy Case ReportDokument23 SeitenTotal Abdominal Hysterectomy Case ReportSarwhin Sugumaran100% (2)
- O&g Case Write UpDokument17 SeitenO&g Case Write Upmohd faizhakimNoch keine Bewertungen
- Paeds Case Write Up 1Dokument29 SeitenPaeds Case Write Up 1Charlotte Ee33% (3)
- Case Write Up SurgeryDokument13 SeitenCase Write Up SurgerySharvin100% (3)
- Case Presentation - EndometriosisDokument47 SeitenCase Presentation - EndometriosisPai PAi67% (9)
- CASE WRITE UP 1: PAEDIATRIC POSTING - MeningitisDokument11 SeitenCASE WRITE UP 1: PAEDIATRIC POSTING - MeningitisAmbhi GanaNoch keine Bewertungen
- Obstetrics and Gynaecology Write Up 3Dokument10 SeitenObstetrics and Gynaecology Write Up 3Luqman HarunNoch keine Bewertungen
- Case Report Example - GynaecologyDokument14 SeitenCase Report Example - GynaecologyDr Onn Azli PuadeNoch keine Bewertungen
- Left Breast SwellingDokument10 SeitenLeft Breast SwellingfarahmazlanNoch keine Bewertungen
- Case Write Up MedicineDokument16 SeitenCase Write Up MedicineSana Anam JahanNoch keine Bewertungen
- Case Write Up Acute PancreatitisDokument25 SeitenCase Write Up Acute PancreatitislunaNoch keine Bewertungen
- Case Write Up-DengueDokument16 SeitenCase Write Up-DengueSyafi'ie Syukri100% (1)
- Case Write Up - Harmeet - Multinodular GoitreDokument29 SeitenCase Write Up - Harmeet - Multinodular GoitreShalini Soorya71% (7)
- Anaest CWU OTDokument15 SeitenAnaest CWU OTHana Fauzi100% (1)
- Erpoc CmeDokument20 SeitenErpoc CmeSharon J StephenNoch keine Bewertungen
- Appendicitis Case Write UpDokument5 SeitenAppendicitis Case Write UpKaarthigan Ramaiah100% (1)
- CWU Gynae Missed MiscarriageDokument8 SeitenCWU Gynae Missed MiscarriageFaris Mohd NasirNoch keine Bewertungen
- Year 5 Obs CWUDokument12 SeitenYear 5 Obs CWUEidi IdhamNoch keine Bewertungen
- Managing Severe Dizziness in Pregnant WomanDokument19 SeitenManaging Severe Dizziness in Pregnant WomanfarahNoch keine Bewertungen
- Farah Cwu Gynae EditDokument16 SeitenFarah Cwu Gynae EditfarahNoch keine Bewertungen
- Tasha's Gynae Case WriteDokument6 SeitenTasha's Gynae Case WriteMelissa Aina Mohd YusofNoch keine Bewertungen
- Placenta Previa Case Write UpDokument24 SeitenPlacenta Previa Case Write Upsaifulhusni100% (2)
- Ong Case Sheet Sem7Dokument13 SeitenOng Case Sheet Sem7Uchiha AnzarNoch keine Bewertungen
- Case Write Up Obstetrics Gestational Diabetes MellitusDokument13 SeitenCase Write Up Obstetrics Gestational Diabetes MellitusRoshandiep GillNoch keine Bewertungen
- Managing Hypertension in PregnancyDokument18 SeitenManaging Hypertension in PregnancyAiman ArifinNoch keine Bewertungen
- Everything You Need to Know About Anemia in PregnancyDokument9 SeitenEverything You Need to Know About Anemia in PregnancyAiman ArifinNoch keine Bewertungen
- Case Write-Up - Obstetrics - Gestational Diabetes MellitusDokument17 SeitenCase Write-Up - Obstetrics - Gestational Diabetes MellitusHakimah K. Suhaimi89% (38)
- Gynaecology Threatened Miscarriage Case WriteupDokument10 SeitenGynaecology Threatened Miscarriage Case WriteupGayathrie Mahalingam100% (1)
- Gynaecology Cwu 1Dokument9 SeitenGynaecology Cwu 1Anonymous fOlJUDDNoch keine Bewertungen
- Case Write UpDokument5 SeitenCase Write UpAisyah Hamdan100% (1)
- Cwu Ong Year 5Dokument23 SeitenCwu Ong Year 5Nurulasyikin MAANoch keine Bewertungen
- Case Write Up 1 ANCDokument5 SeitenCase Write Up 1 ANCfafa dejanNoch keine Bewertungen
- Case Write UpDokument9 SeitenCase Write UpAbdulaziz Al-eisa33% (3)
- WH Case Write Up OBSDokument5 SeitenWH Case Write Up OBSJiaYee GoNoch keine Bewertungen
- Bronchial Asthma Case Write UpDokument5 SeitenBronchial Asthma Case Write UpEry FarishNoch keine Bewertungen
- Case Write Up FibroidDokument17 SeitenCase Write Up FibroidNadsri AmirNoch keine Bewertungen
- Case Write Up 2Dokument16 SeitenCase Write Up 2Shidev100% (1)
- Obstetrics Case of HIV Positive WomanDokument7 SeitenObstetrics Case of HIV Positive WomanAmbhi GanaNoch keine Bewertungen
- Write Up Surgery 1 TambahDokument22 SeitenWrite Up Surgery 1 Tambahazizi abd rahmanNoch keine Bewertungen
- Breast CarcinomaDokument13 SeitenBreast Carcinomamegat120288100% (1)
- Pediatric Case Write-UpDokument10 SeitenPediatric Case Write-UpZul Hisyam Fikri100% (1)
- Internal Medicine Case Write Up 1Dokument16 SeitenInternal Medicine Case Write Up 1Shafiah Aqilah Mohd Jamal67% (3)
- Clerking An o & G CaseDokument57 SeitenClerking An o & G CaseAlan Na100% (2)
- Surgery Case Write Up UGIHDokument37 SeitenSurgery Case Write Up UGIHRahul Audenesen33% (3)
- Case Write UpDokument8 SeitenCase Write Upaladawi930100% (1)
- Chest Pain Sudden OnsetDokument37 SeitenChest Pain Sudden OnsetAzizi Abd RahmanNoch keine Bewertungen
- Acute Appendicitis Case StudyDokument16 SeitenAcute Appendicitis Case StudyAslah NabilahNoch keine Bewertungen
- Gynaecology Case 2Dokument6 SeitenGynaecology Case 2Francesca AkanjiNoch keine Bewertungen
- PPIs Improve ENT Symptoms in GERD PatientsDokument5 SeitenPPIs Improve ENT Symptoms in GERD PatientsHadia YaqubNoch keine Bewertungen
- Internal Medicine Case Write Up 1Dokument14 SeitenInternal Medicine Case Write Up 1Roshandiep GillNoch keine Bewertungen
- Case Presentation Endometriosis 1Dokument15 SeitenCase Presentation Endometriosis 1Muhammad Ahmad Syammakh0% (1)
- Case Summary Ovarian CystDokument4 SeitenCase Summary Ovarian CystFrancesca AkanjiNoch keine Bewertungen
- Case Write-Up 2 - Suba Ramasamy (SB323827)Dokument29 SeitenCase Write-Up 2 - Suba Ramasamy (SB323827)Bavithiran KaruppiahNoch keine Bewertungen
- CWU 2 - Complicated PneumoniaDokument44 SeitenCWU 2 - Complicated PneumoniaJared Khoo Er Hau100% (1)
- ABNORMAL UTERINE BLEEDING EVALUATIONDokument41 SeitenABNORMAL UTERINE BLEEDING EVALUATIONShriyansh Chahar0% (1)
- Cerebral Palsy CaseDokument13 SeitenCerebral Palsy CaseAnusree AnusreervNoch keine Bewertungen
- EM Case Write UpDokument11 SeitenEM Case Write UpRaihana Rafi100% (2)
- Post DatismDokument10 SeitenPost DatismAiman ArifinNoch keine Bewertungen
- Preterm Contraction History ReviewDokument19 SeitenPreterm Contraction History ReviewAiman ArifinNoch keine Bewertungen
- Seminar HandDokument58 SeitenSeminar HandFaris Mohd NasirNoch keine Bewertungen
- Musculotendinous system of the hand and its blood supplyDokument41 SeitenMusculotendinous system of the hand and its blood supplyFaris Mohd NasirNoch keine Bewertungen
- Cwu Surgery 2 Breast CaDokument7 SeitenCwu Surgery 2 Breast CaFaris Mohd NasirNoch keine Bewertungen
- Psychiatric EmergenciesDokument18 SeitenPsychiatric EmergenciesFaris Mohd NasirNoch keine Bewertungen
- Psoriasis Vulgaris KoriDokument19 SeitenPsoriasis Vulgaris KoriFaris Mohd NasirNoch keine Bewertungen
- Child With Rashes: Faris Mohd Nasir 1314597Dokument34 SeitenChild With Rashes: Faris Mohd Nasir 1314597Faris Mohd NasirNoch keine Bewertungen
- Formula For Starting InsulinDokument3 SeitenFormula For Starting InsulinFaris Mohd NasirNoch keine Bewertungen
- Case Presentation BipolarDokument10 SeitenCase Presentation BipolarFaris Mohd NasirNoch keine Bewertungen
- MedSS General Election 2017/2018 Voter TurnoutDokument27 SeitenMedSS General Election 2017/2018 Voter TurnoutFaris Mohd NasirNoch keine Bewertungen
- Understanding Delirium: Causes, Symptoms and TreatmentDokument14 SeitenUnderstanding Delirium: Causes, Symptoms and TreatmentFaris Mohd NasirNoch keine Bewertungen
- Listeriosis - O&G SeminarDokument11 SeitenListeriosis - O&G SeminarFaris Mohd NasirNoch keine Bewertungen
- Listeriosis - O&G SeminarDokument17 SeitenListeriosis - O&G SeminarFaris Mohd NasirNoch keine Bewertungen
- Seminar PAEDS RashesDokument26 SeitenSeminar PAEDS RashesFaris Mohd NasirNoch keine Bewertungen
- Vocabulary Practice 8A - Sofía Sendín PDFDokument1 SeiteVocabulary Practice 8A - Sofía Sendín PDFSofia SendinNoch keine Bewertungen
- Animal Word Search Puzzle Sample3Dokument2 SeitenAnimal Word Search Puzzle Sample3tebugreenNoch keine Bewertungen
- WALT Use Language Features AnswersDokument5 SeitenWALT Use Language Features Answersroom2stjamesNoch keine Bewertungen
- 2013 Skin and Wound Infections - StudentDokument35 Seiten2013 Skin and Wound Infections - Studentmicroperadeniya0% (1)
- LearnEnglish ProfessionalsPodcasts Biotechnology 0Dokument3 SeitenLearnEnglish ProfessionalsPodcasts Biotechnology 0dinaria_ruNoch keine Bewertungen
- Life Sciences P2 Nov 2010 EngDokument14 SeitenLife Sciences P2 Nov 2010 Engbellydanceafrica9540Noch keine Bewertungen
- Urgent Care Grants - RedRoverDokument5 SeitenUrgent Care Grants - RedRovergabyNoch keine Bewertungen
- Cousins Cum 4 1Dokument15 SeitenCousins Cum 4 1ty.mcgillNoch keine Bewertungen
- R-Controlled VowelsDokument10 SeitenR-Controlled VowelsShelby BruzzeseNoch keine Bewertungen
- Ben Ming Nian (Chinese Zodiac Animal Year of Birth)Dokument2 SeitenBen Ming Nian (Chinese Zodiac Animal Year of Birth)SALIMNoch keine Bewertungen
- Noun Practice PagesDokument6 SeitenNoun Practice PagesMaggie Plby100% (1)
- Demidov - A Shooting Trip To Kamchatka 1904Dokument360 SeitenDemidov - A Shooting Trip To Kamchatka 1904Tibor Bánfalvi100% (1)
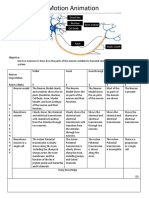
- Neurons Stop Motion AnimationDokument2 SeitenNeurons Stop Motion Animationapi-495006167Noch keine Bewertungen
- A Kingdom of Blood and Betrayal - Holly ReneeDokument250 SeitenA Kingdom of Blood and Betrayal - Holly ReneeViolet MirzaNoch keine Bewertungen
- Balinese Cat Breed Profile: Characteristics, Care, Health and MoreDokument23 SeitenBalinese Cat Breed Profile: Characteristics, Care, Health and MoreprosvetiteljNoch keine Bewertungen
- Efa 2009 UploadDokument87 SeitenEfa 2009 Uploadrobjones21Noch keine Bewertungen
- Cat Breeds & Types GuideDokument13 SeitenCat Breeds & Types Guideprabhakar_n1Noch keine Bewertungen
- Kiara Maestre 2020 05 12 1420 PDFDokument2 SeitenKiara Maestre 2020 05 12 1420 PDFmarionochesNoch keine Bewertungen
- 5090 s14 QP 11 PDFDokument16 Seiten5090 s14 QP 11 PDFruesNoch keine Bewertungen
- Story-Telling Competition Title: The Milkmaid and Her PailDokument6 SeitenStory-Telling Competition Title: The Milkmaid and Her PailCoffee&LoveNoch keine Bewertungen
- ProverbDokument38 SeitenProverbAnkita GoelNoch keine Bewertungen
- Advances in Understanding The Urine-Concentrating MechanismDokument26 SeitenAdvances in Understanding The Urine-Concentrating MechanismKiara Lopez RelaizaNoch keine Bewertungen
- 114 Dog Breeds Ranked by Temperament PDFDokument1 Seite114 Dog Breeds Ranked by Temperament PDFRamona DonisaNoch keine Bewertungen
- Book - Feed Me BillyDokument10 SeitenBook - Feed Me BillyАсель РымхановаNoch keine Bewertungen
- Bali Cattle Breeding SchemeDokument2 SeitenBali Cattle Breeding Schemesyaiful48100% (1)
- Antiremed Kelas 08 Bahasa Inggris: Chapter 4 - Latihan SoalDokument3 SeitenAntiremed Kelas 08 Bahasa Inggris: Chapter 4 - Latihan SoalNonna ShellyNoch keine Bewertungen
- Passion and Deceit Part VI PDFDokument20 SeitenPassion and Deceit Part VI PDFno2meNoch keine Bewertungen
- Issue 235 Organic Consumers AssociationDokument1 SeiteIssue 235 Organic Consumers AssociationFriends of Organic Consumers AssociationNoch keine Bewertungen
- Encoded Designs - Hobbs & Friends of The OSR Bonus Issue 1Dokument20 SeitenEncoded Designs - Hobbs & Friends of The OSR Bonus Issue 1Lionel FagoneNoch keine Bewertungen
- EN Tinycorn and Friends PDF Ebook by AhookADokument39 SeitenEN Tinycorn and Friends PDF Ebook by AhookAPato camaradas100% (1)