Das könnte Ihnen auch gefallen
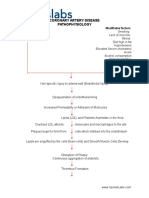
- Coronary Artery Disease PathophysiologyDokument3 SeitenCoronary Artery Disease Pathophysiologynursing concept maps50% (4)
- Coronary Artery Disease Pathophysiology PDFDokument3 SeitenCoronary Artery Disease Pathophysiology PDFMohd Amir Bin Bashir0% (1)
- PathophysiologyDokument34 SeitenPathophysiologyeunams_1195% (20)
- Congestive Heart Failure Pathophysiology Schematic DiagramDokument3 SeitenCongestive Heart Failure Pathophysiology Schematic DiagramJasleen KaurNoch keine Bewertungen
- Pathophysiology of Congestive Heart FailureDokument2 SeitenPathophysiology of Congestive Heart FailurePerry Oliver AlvarezNoch keine Bewertungen
- ShockDokument16 SeitenShockBK WorldNoch keine Bewertungen
- Pathophysiolgoy Coronary Artery DiseaseDokument3 SeitenPathophysiolgoy Coronary Artery DiseaseNursesLabs.comNoch keine Bewertungen
- Congestive Heart Failure Secondary To Coronary Artery Disease PathophysiologyDokument5 SeitenCongestive Heart Failure Secondary To Coronary Artery Disease PathophysiologyJanica MarinasNoch keine Bewertungen
- Congestive Heart Failure PDFDokument11 SeitenCongestive Heart Failure PDFpriyanka bhavsarNoch keine Bewertungen
- SHOCK - HandoutsDokument6 SeitenSHOCK - HandoutsKim GonzalesNoch keine Bewertungen
- Systematic Inflammatory Response SyndromeDokument6 SeitenSystematic Inflammatory Response Syndromenerlyn silaoNoch keine Bewertungen
- Shock and Multi OrganDokument90 SeitenShock and Multi OrganElishaNoch keine Bewertungen
- LT ShockDokument26 SeitenLT ShockLong LieNoch keine Bewertungen
- Cercarial DermatitisDokument18 SeitenCercarial DermatitisEfraimNoch keine Bewertungen
- Acute Coronary Syndrome PathophysiologyDokument3 SeitenAcute Coronary Syndrome PathophysiologyJocelle Joy OrellanedaNoch keine Bewertungen
- Fluid and ElectrolytesDokument105 SeitenFluid and ElectrolytesCarl Elexer Cuyugan Ano100% (3)
- Nursing Diagnosis Nursing Intervention Rationale: Prioritized Nursing Problem For Congestive Heart FailureDokument2 SeitenNursing Diagnosis Nursing Intervention Rationale: Prioritized Nursing Problem For Congestive Heart FailureMyrshaida IbrahimNoch keine Bewertungen
- Pathophysiology of Hypertension: RAAS Activation and Organ DamageDokument2 SeitenPathophysiology of Hypertension: RAAS Activation and Organ DamageAlvin RamirezNoch keine Bewertungen
- 3 Heart FailureDokument8 Seiten3 Heart FailureAudrey Ann AcobNoch keine Bewertungen
- Feedback Mechanisms Stimulus Receptor Control Center Effector ResponseDokument1 SeiteFeedback Mechanisms Stimulus Receptor Control Center Effector ResponsekimNoch keine Bewertungen
- Shock 2019 - SmallDokument89 SeitenShock 2019 - SmallKristian Dwi CahyaNoch keine Bewertungen
- Pathophysiology of Congestive Heart Failure: Predisposing Factors Precipitating/Aggravating FactorsDokument1 SeitePathophysiology of Congestive Heart Failure: Predisposing Factors Precipitating/Aggravating Factorsguillermojerry100% (2)
- Pathophysiology and Nursing Care Plan for Cor PulmonaleDokument6 SeitenPathophysiology and Nursing Care Plan for Cor PulmonaleMonette Abalos MendovaNoch keine Bewertungen
- Menigitis & EncephalitisDokument38 SeitenMenigitis & EncephalitisKim GonzalesNoch keine Bewertungen
- Fluids and Electrolytes ReviewerDokument4 SeitenFluids and Electrolytes ReviewerdverraNoch keine Bewertungen
- Cikini Pengelolaan Nyeri FinalDokument85 SeitenCikini Pengelolaan Nyeri FinalisabellaruthhhNoch keine Bewertungen
- Pathophysiology of HCVD DM2 CVD Left Basal GangliaDokument1 SeitePathophysiology of HCVD DM2 CVD Left Basal GangliaJake Caballo100% (1)
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Dokument3 SeitenDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNoch keine Bewertungen
- RegulationDokument6 SeitenRegulationraacchhaaeelNoch keine Bewertungen
- Congestive Heart FailureDokument10 SeitenCongestive Heart FailurekarenbelnasNoch keine Bewertungen
- Pathophysiology of HCVD, DM2, CVD (Left Basal Ganglia)Dokument1 SeitePathophysiology of HCVD, DM2, CVD (Left Basal Ganglia)rexale ria100% (1)
- Angina Risk Factors & SymptomsDokument2 SeitenAngina Risk Factors & Symptomsjoyrena ochondraNoch keine Bewertungen
- Short and Long Term Regulation and Determinants of BPDokument90 SeitenShort and Long Term Regulation and Determinants of BPDan Tristam MicabaloNoch keine Bewertungen
- NCM 112 Cellular Aberrations: Fluid Volume ExcessDokument3 SeitenNCM 112 Cellular Aberrations: Fluid Volume ExcessAngeline NavarroNoch keine Bewertungen
- SHOCKDokument1 SeiteSHOCKJessa Mae Alforque AsentistaNoch keine Bewertungen
- Pathophysiology of Congestive Heart FailureDokument2 SeitenPathophysiology of Congestive Heart FailureTrixia Almendral100% (2)
- Compensatory Mechanism of Circulatory ShockDokument29 SeitenCompensatory Mechanism of Circulatory ShockWan Razin Wan Hassan100% (1)
- Tetralogy of Fallot Pathophysiology & Risk FactorsDokument1 SeiteTetralogy of Fallot Pathophysiology & Risk FactorsEiztirfNoch keine Bewertungen
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Dokument6 SeitenPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNoch keine Bewertungen
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Dokument6 SeitenPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNoch keine Bewertungen
- Inp PathoDokument1 SeiteInp PathoNoveeNoch keine Bewertungen
- Transient Ischemic Attack Precipitating Factors Predisposing FactorsDokument6 SeitenTransient Ischemic Attack Precipitating Factors Predisposing FactorsYosef OxinioNoch keine Bewertungen
- Pre Gestational 1Dokument12 SeitenPre Gestational 1Fatima TañedoNoch keine Bewertungen
- PATHOPHYDokument3 SeitenPATHOPHYArlly Faena AbadNoch keine Bewertungen
- Acid-Base Imbalances: Types, Causes, Symptoms & TreatmentsDokument4 SeitenAcid-Base Imbalances: Types, Causes, Symptoms & TreatmentsHenric CasimiroNoch keine Bewertungen
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDokument92 SeitenHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoNoch keine Bewertungen
- Congestive Heart Failure PathophysiologyDokument7 SeitenCongestive Heart Failure PathophysiologyAileen Grace RodrigoNoch keine Bewertungen
- Pathophysiology of Congestive Heart FailureDokument3 SeitenPathophysiology of Congestive Heart FailureMel Izhra N. MargateNoch keine Bewertungen
- O High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleDokument4 SeitenO High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleJoherNoch keine Bewertungen
- Bio Project Chapter 13Dokument28 SeitenBio Project Chapter 13FionNoch keine Bewertungen
- Risk Factors and Causes of HypertensionDokument8 SeitenRisk Factors and Causes of HypertensionannisaNoch keine Bewertungen
- Pathophysio - Stemi - FinalDokument4 SeitenPathophysio - Stemi - FinalPrincessDianneNoch keine Bewertungen
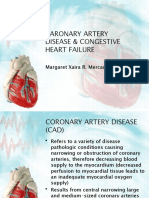
- Caronary Artery Disease & Congestive Heart Failure: Margaret Xaira R. Mercado RNDokument32 SeitenCaronary Artery Disease & Congestive Heart Failure: Margaret Xaira R. Mercado RNMargaret Xaira Rubio MercadoNoch keine Bewertungen
- Hypoxia Ischemic Encephalopathy and Congenital AnomaliesDokument36 SeitenHypoxia Ischemic Encephalopathy and Congenital AnomaliesVarna MohanNoch keine Bewertungen
- Pathophysiology Non-Modifiable Factors Modifiable FactorsDokument3 SeitenPathophysiology Non-Modifiable Factors Modifiable FactorsErrol B. TiozonNoch keine Bewertungen
- Diagnosis&Manajemen ShockDokument8 SeitenDiagnosis&Manajemen ShockHJKIMNoch keine Bewertungen
- Fluid and Electrolytes for Nursing StudentsVon EverandFluid and Electrolytes for Nursing StudentsBewertung: 5 von 5 Sternen5/5 (12)
- Adrenal Fatigue: Understanding the Symptoms: How Malfunctioning Adrenal Glands Negatively Affect the BodyVon EverandAdrenal Fatigue: Understanding the Symptoms: How Malfunctioning Adrenal Glands Negatively Affect the BodyNoch keine Bewertungen
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtVon EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtBewertung: 5 von 5 Sternen5/5 (1)
- DOH Approved Medicinal PlantsDokument2 SeitenDOH Approved Medicinal PlantsAikoP.NarcisoNoch keine Bewertungen
- Physical Pharmacy Post-Lab Discussion For Preliminary PeriodDokument18 SeitenPhysical Pharmacy Post-Lab Discussion For Preliminary PeriodKatryn Punsalang100% (2)
- RicinDokument2 SeitenRicinAikoP.NarcisoNoch keine Bewertungen
- Importance of Physical Pharmacy for Pharmaceutical SciencesDokument3 SeitenImportance of Physical Pharmacy for Pharmaceutical SciencesAikoP.NarcisoNoch keine Bewertungen
- Heart Failure GuideDokument8 SeitenHeart Failure GuideAikoP.NarcisoNoch keine Bewertungen
- ASCE's Roadmap to Sustainable InfrastructureDokument5 SeitenASCE's Roadmap to Sustainable InfrastructureRodolfo De La GarzaNoch keine Bewertungen
- Case Study of Bronchial Asthma in Acute ExacerbationDokument16 SeitenCase Study of Bronchial Asthma in Acute Exacerbationdextroid1290% (29)
- Coulter Slidemaking - Service ManualDokument443 SeitenCoulter Slidemaking - Service ManualIoana BeteaNoch keine Bewertungen
- 6.11 Bullying ReadyDokument41 Seiten6.11 Bullying ReadyAstraX EducationNoch keine Bewertungen
- 1393un 2023-03Dokument94 Seiten1393un 2023-03Marcela Martínez100% (1)
- Nosotros NoDokument2 SeitenNosotros NoAlcindorLeadonNoch keine Bewertungen
- 12 SM 2017 Biology EngDokument206 Seiten12 SM 2017 Biology EngJaiminGajjar100% (1)
- Freud and The Greeks PDFDokument19 SeitenFreud and The Greeks PDFJulio GarciaNoch keine Bewertungen
- Roth - From Free WombDokument19 SeitenRoth - From Free WombNubss SSNoch keine Bewertungen
- Hts Policy PhilippinesDokument15 SeitenHts Policy PhilippinesBrunxAlabastro100% (1)
- A Six Step Approach To Writing A Formal SummaryDokument5 SeitenA Six Step Approach To Writing A Formal SummaryБезымянный КактусNoch keine Bewertungen
- C.Systematic ReviewDokument12 SeitenC.Systematic ReviewIta ApriliyaniNoch keine Bewertungen
- Conceptual Understanding of OptimismDokument8 SeitenConceptual Understanding of OptimismUDITA PARIKHNoch keine Bewertungen
- Using The Vineland 3 On Q Global Pearsonclinical Com AuDokument16 SeitenUsing The Vineland 3 On Q Global Pearsonclinical Com AuAndreia SilvaNoch keine Bewertungen
- Susarla 2020Dokument7 SeitenSusarla 2020lauNoch keine Bewertungen
- CBSE Class 6 Science Components of Food MCQs Set A, Multiple Choice Questions For ScienceDokument4 SeitenCBSE Class 6 Science Components of Food MCQs Set A, Multiple Choice Questions For ScienceNinaNoch keine Bewertungen
- Uber CEO EmailDokument5 SeitenUber CEO EmailKhristopher J. BrooksNoch keine Bewertungen
- Graded RecitationDokument22 SeitenGraded RecitationClara MaeNoch keine Bewertungen
- Veterinarians 03-2023Dokument13 SeitenVeterinarians 03-2023PRC BaguioNoch keine Bewertungen
- Helene Deutsch, A Psychoanalysts Life (Lacanempdf)Dokument400 SeitenHelene Deutsch, A Psychoanalysts Life (Lacanempdf)Carlos AugustoNoch keine Bewertungen
- Clinical Psychopharmacology Principles and Practice by S Nassir CompressedDokument600 SeitenClinical Psychopharmacology Principles and Practice by S Nassir CompressedCátia Ramos100% (1)
- RFP 23-031 Electronic & Physical Site SecurityDokument31 SeitenRFP 23-031 Electronic & Physical Site SecurityElle PolonNoch keine Bewertungen
- WHMIS-HHPS ReviewDokument12 SeitenWHMIS-HHPS Review9RO ClanNoch keine Bewertungen
- TVEC Guide to Sri Lanka's Vocational Education SystemDokument31 SeitenTVEC Guide to Sri Lanka's Vocational Education Systemshishir_cNoch keine Bewertungen
- ML SyllDokument2 SeitenML Syllmurlak37Noch keine Bewertungen
- Gac 311 NotesDokument26 SeitenGac 311 NotesZAINABU OLANDONoch keine Bewertungen
- Business VmvogDokument3 SeitenBusiness VmvogAmadea SutandiNoch keine Bewertungen
- The Kübler-Ross Change Curve: Emotional Response To ChangeDokument9 SeitenThe Kübler-Ross Change Curve: Emotional Response To ChangeChanel PostelNoch keine Bewertungen
- Quality Control Procedure For HVDokument9 SeitenQuality Control Procedure For HVVIKRAM DESAINoch keine Bewertungen
- Academic Compare and Contrast Essay TopicsDokument53 SeitenAcademic Compare and Contrast Essay Topicszzcpllaeg100% (3)