Das könnte Ihnen auch gefallen
- Hematology SOPsDokument99 SeitenHematology SOPssalamon2t100% (1)
- Lab Policies Differential Counting and Morphology Lab 5074Dokument14 SeitenLab Policies Differential Counting and Morphology Lab 5074Egil SantosNoch keine Bewertungen
- Prismaflex TrainingDokument37 SeitenPrismaflex TrainingSarah Al-Qadri100% (4)
- Hematology UnitDokument8 SeitenHematology UnitMary CabalceNoch keine Bewertungen
- Blood TransfusionDokument37 SeitenBlood TransfusionSumathi Akshaya100% (1)
- Towler Transurethral14346Dokument4 SeitenTowler Transurethral14346Dian NovitasariNoch keine Bewertungen
- 1 s2.0 S0085253815349693 MainDokument5 Seiten1 s2.0 S0085253815349693 MainSotero MoralesNoch keine Bewertungen
- Peter Hudson Blood TransfusionDokument29 SeitenPeter Hudson Blood TransfusionRyan-Jay AbolenciaNoch keine Bewertungen
- PRP TechniqueDokument9 SeitenPRP Techniquerandomaeiou7273Noch keine Bewertungen
- Evaluation of The Abbott CELL-DYN 4000 HematologyDokument10 SeitenEvaluation of The Abbott CELL-DYN 4000 Hematologypasamuco473Noch keine Bewertungen
- Blood Transfusion Peter HudsonDokument21 SeitenBlood Transfusion Peter HudsonWai YanNoch keine Bewertungen
- Cases in Surgical Critical CareDokument36 SeitenCases in Surgical Critical CareHasan ShanawaniNoch keine Bewertungen
- tmp6536 TMPDokument8 Seitentmp6536 TMPFrontiersNoch keine Bewertungen
- Fat CATSTransfus Med 17Dokument9 SeitenFat CATSTransfus Med 17Jamel GrineNoch keine Bewertungen
- Ject 2004 v36 n1 Lawson p66 HCDokument4 SeitenJect 2004 v36 n1 Lawson p66 HCMuzammil AhmedNoch keine Bewertungen
- Blood Safety in Nursing CareDokument33 SeitenBlood Safety in Nursing CareVidya Jayasekaran JNoch keine Bewertungen
- 7080138A Diacap Polysulfone Prospekt e 01 09Dokument6 Seiten7080138A Diacap Polysulfone Prospekt e 01 09natasa972Noch keine Bewertungen
- The Effect of Pre-Operative Blood Withdrawal, With or Without Sequestration, On Allogeneic Blood Product RequirementsDokument9 SeitenThe Effect of Pre-Operative Blood Withdrawal, With or Without Sequestration, On Allogeneic Blood Product Requirementslekah khasanahNoch keine Bewertungen
- COMPLETE BLOOD COUNT Lecture GuideDokument9 SeitenCOMPLETE BLOOD COUNT Lecture GuideKaycee Gretz LorescaNoch keine Bewertungen
- ASTM 71830-97 - Standard Practice For Selection of Blood For in Vitro Evaluation of Blood PumpsDokument2 SeitenASTM 71830-97 - Standard Practice For Selection of Blood For in Vitro Evaluation of Blood PumpsJoãoNoch keine Bewertungen
- Blood Transfusion On Dialysis Guidelines Aug 2017 PDFDokument5 SeitenBlood Transfusion On Dialysis Guidelines Aug 2017 PDFYolanda IrawatiNoch keine Bewertungen
- Efficacy of Platelet Gel in Reconstructive Bone Surgery: M F, MD P D, MD I F, S D M D G, MD R A, MDDokument3 SeitenEfficacy of Platelet Gel in Reconstructive Bone Surgery: M F, MD P D, MD I F, S D M D G, MD R A, MDAnsh Veer ChouhanNoch keine Bewertungen
- HaematologyDokument11 SeitenHaematologyIkram AzmanNoch keine Bewertungen
- Massive Haemorrhage: P Donnelly B FergusonDokument18 SeitenMassive Haemorrhage: P Donnelly B FergusonRizqiNoch keine Bewertungen
- Ct7 Fluid, Electrolyte ImbalanceDokument9 SeitenCt7 Fluid, Electrolyte ImbalanceAlondra VelascoNoch keine Bewertungen
- 0049 3848 (80) 90005 5Dokument9 Seiten0049 3848 (80) 90005 5Dian NovitasariNoch keine Bewertungen
- CVVHDokument4 SeitenCVVHSyarif UddinNoch keine Bewertungen
- PG Lab 2 VenipunctureDokument26 SeitenPG Lab 2 VenipunctureFlordabee Mercurio PaniaguaNoch keine Bewertungen
- Original Article: Rapamycin Combined with α-Cyanoacrylate Contributes to Inhibiting Intimal Hyperplasia in Rat ModelsDokument8 SeitenOriginal Article: Rapamycin Combined with α-Cyanoacrylate Contributes to Inhibiting Intimal Hyperplasia in Rat ModelsMariantFomperosaNoch keine Bewertungen
- Evaluation and Performance Characteristics of The Q Hemostasis Analyzer, An Automated Coagulation AnalyzerDokument9 SeitenEvaluation and Performance Characteristics of The Q Hemostasis Analyzer, An Automated Coagulation AnalyzerEsther Jara GarcíaNoch keine Bewertungen
- Cerebrospinal Fluid Penetration of AmikacinDokument3 SeitenCerebrospinal Fluid Penetration of AmikacinDanny JacobusNoch keine Bewertungen
- High-Throughput Characterization of Indices of Clinical Chemistry and HematologyDokument22 SeitenHigh-Throughput Characterization of Indices of Clinical Chemistry and HematologyCheng Ho OcNoch keine Bewertungen
- Evaluation of The Automated Coagulation Analyzer SYSMEX CA 6000Dokument7 SeitenEvaluation of The Automated Coagulation Analyzer SYSMEX CA 6000Esther Jara GarcíaNoch keine Bewertungen
- Karski1999 Article EtiologyOfPreoperativeAnemiaInDokument4 SeitenKarski1999 Article EtiologyOfPreoperativeAnemiaInAleksandar VilaNoch keine Bewertungen
- Gi Bleeding CaseDokument28 SeitenGi Bleeding CaseP BNoch keine Bewertungen
- OriginalDokument6 SeitenOriginalSynder Castellanos del AguilaNoch keine Bewertungen
- BlacT Package InsertDokument2 SeitenBlacT Package InsertaliborabasNoch keine Bewertungen
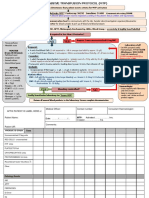
- PBM Module1 MTP Template 0Dokument2 SeitenPBM Module1 MTP Template 0Daniela Marie RonquilloNoch keine Bewertungen
- Civd - AjcpDokument11 SeitenCivd - AjcpHenrique MachadoNoch keine Bewertungen
- AUMENTAR MAP 65-85 No Mejorar Urina y LactatoDokument4 SeitenAUMENTAR MAP 65-85 No Mejorar Urina y LactatoCurro InglesNoch keine Bewertungen
- Hiroshi Kondo JPN Whole Blood for Hematology QC MaretialDokument33 SeitenHiroshi Kondo JPN Whole Blood for Hematology QC MaretialAnonymous EbAN1jmNoch keine Bewertungen
- 104063870902100512Dokument5 Seiten104063870902100512Toafan MegaNoch keine Bewertungen
- Evaluation of The Automated Coagulation Analyzer Sysmex CA-7000 2005Dokument9 SeitenEvaluation of The Automated Coagulation Analyzer Sysmex CA-7000 2005Esther Jara GarcíaNoch keine Bewertungen
- 2.8 Investigation of Transfusion ReactionDokument8 Seiten2.8 Investigation of Transfusion ReactionBALAJINoch keine Bewertungen
- Ferritin - SOPDokument6 SeitenFerritin - SOPNoor AshrafNoch keine Bewertungen
- Sismex ManualDokument11 SeitenSismex ManualDigo SomengNoch keine Bewertungen
- Baseline:: Notify Transfusion Laboratory To: Activate MTP'. Footscray: 56292 Sunshine: 51480 Allocate Team RolesDokument2 SeitenBaseline:: Notify Transfusion Laboratory To: Activate MTP'. Footscray: 56292 Sunshine: 51480 Allocate Team RolesDumindu PereraNoch keine Bewertungen
- 039.14 Management of Clotted Access Extra Corporeal Circuit.Dokument9 Seiten039.14 Management of Clotted Access Extra Corporeal Circuit.Khoi RNNoch keine Bewertungen
- Biolabo PTDokument2 SeitenBiolabo PTSendy Fadilla OktoraNoch keine Bewertungen
- The Open Anesthesia JournalDokument11 SeitenThe Open Anesthesia JournalmikoNoch keine Bewertungen
- Feline Blood Film 230902 043358Dokument13 SeitenFeline Blood Film 230902 04335897namithaNoch keine Bewertungen
- The Preservation of Whole Blood: Max M. Strumia,, Miss Margaret Dolan, Miss Louise ColwellDokument6 SeitenThe Preservation of Whole Blood: Max M. Strumia,, Miss Margaret Dolan, Miss Louise ColwellRevi NisaNoch keine Bewertungen
- PGDT Protocol Summary ReferenceDokument32 SeitenPGDT Protocol Summary Referenceghg sddNoch keine Bewertungen
- Control of Bleeding in Severely Uremic Patients Undergoing Oral SurgeryDokument4 SeitenControl of Bleeding in Severely Uremic Patients Undergoing Oral SurgeryAnonymous GyqTkXMwMNoch keine Bewertungen
- 02.99.055 (PDF Library)Dokument3 Seiten02.99.055 (PDF Library)Muthu KumarNoch keine Bewertungen
- Clinical Outcomes For Maintenance Hemodialysis Patients Using A High Flux FX60 DialyzerDokument7 SeitenClinical Outcomes For Maintenance Hemodialysis Patients Using A High Flux FX60 DialyzerOsama El NegmNoch keine Bewertungen
- PIIS0085253815601144Dokument5 SeitenPIIS0085253815601144Владимир Ильич ЛенинNoch keine Bewertungen
- Case Presentation: Dr. Anjali Pandey DNB ResidentDokument35 SeitenCase Presentation: Dr. Anjali Pandey DNB Residentanjali pandeyNoch keine Bewertungen
- Cardiac Magnetic Resonance Atlas: 101 Clinical CasesVon EverandCardiac Magnetic Resonance Atlas: 101 Clinical CasesNoch keine Bewertungen
- Thrombosis and Bleeding Disorders: Theory and MethodsVon EverandThrombosis and Bleeding Disorders: Theory and MethodsNils U. BangBewertung: 2 von 5 Sternen2/5 (1)
- Career Guide / Interviewing / Career Guide / InterviewingDokument4 SeitenCareer Guide / Interviewing / Career Guide / InterviewingshihabNoch keine Bewertungen
- Biomed Technician: The JobDokument6 SeitenBiomed Technician: The JobshihabNoch keine Bewertungen
- Medical and Instrumentation Engineers - YemenHR - HTMLDokument4 SeitenMedical and Instrumentation Engineers - YemenHR - HTMLshihabNoch keine Bewertungen
- Off Grid System Design SheetDokument6 SeitenOff Grid System Design SheetshihabNoch keine Bewertungen
- Psychiatric Hostel Design GuidelinesDokument104 SeitenPsychiatric Hostel Design GuidelinesshihabNoch keine Bewertungen
- Teoria y Practica de La Purificacion Del H2O - Tomo 2Dokument32 SeitenTeoria y Practica de La Purificacion Del H2O - Tomo 2Dextre Pajuelo CristoferNoch keine Bewertungen
- HTM 02 01 Part ADokument201 SeitenHTM 02 01 Part Aobligatoriu100% (2)
- Soft Series Bed Head Unit Brochure - v1-1Dokument8 SeitenSoft Series Bed Head Unit Brochure - v1-1shihabNoch keine Bewertungen
- Surgical ToolsDokument11 SeitenSurgical ToolsshihabNoch keine Bewertungen
- Specifications For Medical Equipment OPDokument66 SeitenSpecifications For Medical Equipment OPshihabNoch keine Bewertungen
- Hemodialysis Machines Testing Your UnderstandingDokument30 SeitenHemodialysis Machines Testing Your UnderstandingstarykNoch keine Bewertungen
- 70c777d2 7c41 4387 BCFC 4019efb31fe238 Dialysis MachineDokument3 Seiten70c777d2 7c41 4387 BCFC 4019efb31fe238 Dialysis MachineshihabNoch keine Bewertungen
- Circuit Diagram: Emulators For 80C51Dokument1 SeiteCircuit Diagram: Emulators For 80C51shihabNoch keine Bewertungen
- Dialysis MachineDokument1 SeiteDialysis MachineshihabNoch keine Bewertungen
- Technical Specifications For Dialysis MachineDokument2 SeitenTechnical Specifications For Dialysis MachineJohn Son G100% (1)
- 67 PDFDokument7 Seiten67 PDFshihabNoch keine Bewertungen
- Group MediclaimDokument21 SeitenGroup MediclaimAishwarya Deepak ChintalapatiNoch keine Bewertungen
- Alliancehpsr KenyaabridgedprimasysDokument12 SeitenAlliancehpsr Kenyaabridgedprimasysdisposable101Noch keine Bewertungen
- 03 Medical Records DeptDokument3 Seiten03 Medical Records Deptproghekm0% (1)
- ADR News Dec2008 Vol10 No3Dokument8 SeitenADR News Dec2008 Vol10 No3William ChandraNoch keine Bewertungen
- Insomnia: Management of Underlying ProblemsDokument6 SeitenInsomnia: Management of Underlying Problems7OrangesNoch keine Bewertungen
- Changes in Brain Function (Quantitative EEG Cordance) During Placebo Lead-In and Treatment Outcomes in Clinical Trials For Major DepressionDokument7 SeitenChanges in Brain Function (Quantitative EEG Cordance) During Placebo Lead-In and Treatment Outcomes in Clinical Trials For Major DepressiondebdotnetNoch keine Bewertungen
- Pathophysiology and Natural History of Atrial Septal DefectDokument10 SeitenPathophysiology and Natural History of Atrial Septal DefectrosaNoch keine Bewertungen
- The Basal Ganglia and Movement Disorders 2015 RevisedDokument19 SeitenThe Basal Ganglia and Movement Disorders 2015 RevisedJoan ChoiNoch keine Bewertungen
- Air PolishingDokument9 SeitenAir PolishingGonçalo Cunha-CoutinhoNoch keine Bewertungen
- 666 CDR - Scale PDFDokument10 Seiten666 CDR - Scale PDFIkanpaus Di BlogspotNoch keine Bewertungen
- Cariogram E BookDokument90 SeitenCariogram E BookAlifianNoch keine Bewertungen
- 2 CP Bekam Angin Tahap 3Dokument8 Seiten2 CP Bekam Angin Tahap 3Norhissam MustafaNoch keine Bewertungen
- Clinical Study: Development of Dengue Infection Severity ScoreDokument6 SeitenClinical Study: Development of Dengue Infection Severity ScoreValencius SunandarNoch keine Bewertungen
- Case Analysis SchizoDokument4 SeitenCase Analysis SchizoiamELHIZANoch keine Bewertungen
- MCQ 2019 Part 1 UseDokument94 SeitenMCQ 2019 Part 1 UseWanny WattakavanichNoch keine Bewertungen
- Comat NotesDokument33 SeitenComat NotesVee Mend100% (1)
- HCA/HealthONE's North Suburban Medical Center Achieves Healthgrades 2020 Patient Safety Excellence Award (TM)Dokument3 SeitenHCA/HealthONE's North Suburban Medical Center Achieves Healthgrades 2020 Patient Safety Excellence Award (TM)PR.comNoch keine Bewertungen
- Application of The Bethesda Classification For Thyroid FNABDokument12 SeitenApplication of The Bethesda Classification For Thyroid FNABJudrelle Krizia MarianoNoch keine Bewertungen
- Clinical Study of Postpartum Eclampsia: Dr. S. K. Rath, Dr. Swati AgrawalDokument3 SeitenClinical Study of Postpartum Eclampsia: Dr. S. K. Rath, Dr. Swati AgrawalSulabh ShresthaNoch keine Bewertungen
- Kuliah 8. Anestesi - Syok Dan Tata LaksananyaDokument63 SeitenKuliah 8. Anestesi - Syok Dan Tata LaksananyaDesi Suryani DewiNoch keine Bewertungen
- Alzehimer GuiaDokument9 SeitenAlzehimer GuiaAlejandro PiscitelliNoch keine Bewertungen
- Drug Overdose: Dr. Diah Ari Safitri, SPPDDokument9 SeitenDrug Overdose: Dr. Diah Ari Safitri, SPPDmkafabillahNoch keine Bewertungen
- Policies and Procedures Manual 2017-2018Dokument43 SeitenPolicies and Procedures Manual 2017-2018gus_lionsNoch keine Bewertungen
- Intertrigo Facts: Obesity ItchingDokument3 SeitenIntertrigo Facts: Obesity Itchingyyfan98Noch keine Bewertungen
- Richard Belli WorkshopDokument62 SeitenRichard Belli WorkshopalicefreespiritNoch keine Bewertungen
- '05 Sullivan A.Dokument48 Seiten'05 Sullivan A.Geo NavarroNoch keine Bewertungen
- 11 Common Symptoms of CandidaDokument12 Seiten11 Common Symptoms of Candidasantana2013Noch keine Bewertungen
- Needle CutterDokument6 SeitenNeedle CutterPaul Anthony Centeno PimentelNoch keine Bewertungen
- NEURO2 1.02C Hemorrhagic Stroke - Dr. HiyadanDokument2 SeitenNEURO2 1.02C Hemorrhagic Stroke - Dr. HiyadanAra Diocos100% (1)
- ParacetamolDokument24 SeitenParacetamolFriné MirandaNoch keine Bewertungen