Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Soal Imspq 2015Dokument9 SeitenSoal Imspq 2015AgungBudiPamungkasNoch keine Bewertungen
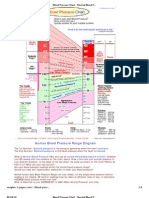
- Blood Pressure ChartDokument4 SeitenBlood Pressure ChartPixelateNoch keine Bewertungen
- Staffing ComputationsDokument24 SeitenStaffing ComputationsOliric Acnab Nabcih100% (4)
- Brmedj05524 0003Dokument1 SeiteBrmedj05524 0003AgungBudiPamungkasNoch keine Bewertungen
- The Synthesis of Kynurenic Acid in Mammals: An Updated Kynurenine Aminotransferase Structural KatalogueDokument9 SeitenThe Synthesis of Kynurenic Acid in Mammals: An Updated Kynurenine Aminotransferase Structural KatalogueAgungBudiPamungkasNoch keine Bewertungen
- The Patient With Hypertension Undergoing Surgery: ReviewDokument6 SeitenThe Patient With Hypertension Undergoing Surgery: ReviewAgungBudiPamungkasNoch keine Bewertungen
- Syinphyseotomy: DR. ON Cesarean Section. (BritishDokument3 SeitenSyinphyseotomy: DR. ON Cesarean Section. (BritishAgungBudiPamungkasNoch keine Bewertungen
- Physical Kinglake, Atkinson : PhilosophyDokument9 SeitenPhysical Kinglake, Atkinson : PhilosophyAgungBudiPamungkasNoch keine Bewertungen
- Starr, Kinglake, Month, Kinglake Practice, Practitioners,: Mr. The JournalDokument2 SeitenStarr, Kinglake, Month, Kinglake Practice, Practitioners,: Mr. The JournalAgungBudiPamungkasNoch keine Bewertungen
- Hepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyDokument17 SeitenHepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyAgungBudiPamungkasNoch keine Bewertungen
- How I Treat Anemia in Pregnancy: Iron, Cobalamin, and FolateDokument11 SeitenHow I Treat Anemia in Pregnancy: Iron, Cobalamin, and FolateAgungBudiPamungkasNoch keine Bewertungen
- International Journal of Infectious DiseasesDokument4 SeitenInternational Journal of Infectious DiseasesAgungBudiPamungkasNoch keine Bewertungen
- On June 30, 2019 Downloaded From Published Online: 1 March, 1912 - Supp InfoDokument20 SeitenOn June 30, 2019 Downloaded From Published Online: 1 March, 1912 - Supp InfoAgungBudiPamungkasNoch keine Bewertungen
- CJWCNLWKVNDokument1 SeiteCJWCNLWKVNAgungBudiPamungkasNoch keine Bewertungen
- Succinylcholine ChlorideDokument19 SeitenSuccinylcholine ChlorideAgungBudiPamungkas100% (1)
- Follow Up Bangsal Stella Gemi Annisa Agung Stella Annisa Gemi AgungDokument1 SeiteFollow Up Bangsal Stella Gemi Annisa Agung Stella Annisa Gemi AgungAgungBudiPamungkasNoch keine Bewertungen
- Tesis StuntingDokument2 SeitenTesis StuntingLentri Fitri MulyaniNoch keine Bewertungen
- Hepatitis CDokument15 SeitenHepatitis CMohamed IsmailNoch keine Bewertungen
- Pelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesDokument13 SeitenPelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesIndah MeylizaNoch keine Bewertungen
- Planned Parenthood and Students Knowledge of Contraceptive MethodsDokument10 SeitenPlanned Parenthood and Students Knowledge of Contraceptive MethodssncuNoch keine Bewertungen
- Palliative+care Toolkit SwahiliDokument110 SeitenPalliative+care Toolkit SwahiliIssa Juma K. AlmazruiNoch keine Bewertungen
- A QUASI SynopsisDokument9 SeitenA QUASI Synopsischaranjit kaurNoch keine Bewertungen
- Nova Stat Strip Glucose 261021Dokument35 SeitenNova Stat Strip Glucose 261021Herbanu Haryo PramonoNoch keine Bewertungen
- Discharge Planning PaperDokument4 SeitenDischarge Planning Paperapi-338998736Noch keine Bewertungen
- Lesson 14 - : Nutrition For Adults: The Early, Middle, and Late YearsDokument30 SeitenLesson 14 - : Nutrition For Adults: The Early, Middle, and Late YearsMelody MirandaNoch keine Bewertungen
- Stainless Steel CrownDokument63 SeitenStainless Steel CrownKaran Arora100% (1)
- Communication Interaction in ICU-Patient and Staff Experiences and Perceptions.Dokument5 SeitenCommunication Interaction in ICU-Patient and Staff Experiences and Perceptions.osondoarNoch keine Bewertungen
- Wiley Protocol Consumer Newsletter September 2009Dokument3 SeitenWiley Protocol Consumer Newsletter September 2009WileyProtocolNoch keine Bewertungen
- Application of Hot Water BagDokument9 SeitenApplication of Hot Water BagDoj Deej Mendoza GambleNoch keine Bewertungen
- Siwes Report.Dokument64 SeitenSiwes Report.Nmesoma AjokuNoch keine Bewertungen
- Chapter7 H.WDokument16 SeitenChapter7 H.WNorah AbdallahNoch keine Bewertungen
- Migraine Diaries PDFDokument4 SeitenMigraine Diaries PDFDr.Gopinath SaravananNoch keine Bewertungen
- PMID 1393911 Niacin Vs NiacinamideDokument1 SeitePMID 1393911 Niacin Vs NiacinamideInbal LandsbergNoch keine Bewertungen
- (IJIT-V7I2P6) :B.Rajalakshmi, G.Sanjana DeviDokument5 Seiten(IJIT-V7I2P6) :B.Rajalakshmi, G.Sanjana DeviIJITJournalsNoch keine Bewertungen
- EssayDokument16 SeitenEssayLorenz Sagayaga ListaNoch keine Bewertungen
- Meal Planning 1Dokument12 SeitenMeal Planning 1KHALEEL SALEHNoch keine Bewertungen
- NEWBORN CAREPLAN - VEST - FISTULA SurgicalDokument16 SeitenNEWBORN CAREPLAN - VEST - FISTULA SurgicalArchana SahuNoch keine Bewertungen
- PE Hyperventilation TopicDokument2 SeitenPE Hyperventilation TopicJimmy Jr ChapapNoch keine Bewertungen
- A Pocket Guide To Pain Management PDFDokument324 SeitenA Pocket Guide To Pain Management PDFGalina MalaiNoch keine Bewertungen
- HomeopathyResearchEvidenceBase - 10 29 15 PDFDokument138 SeitenHomeopathyResearchEvidenceBase - 10 29 15 PDFdr.mengane100% (1)
- MS GuldaneDokument22 SeitenMS GuldaneKhyy SafitryNoch keine Bewertungen
- ThesisDokument58 SeitenThesisSimran MáhátoNoch keine Bewertungen
- Catheterisation - Suprapubic Catheter ProcedureNewDokument12 SeitenCatheterisation - Suprapubic Catheter ProcedureNewAmit KapuriaNoch keine Bewertungen
- HPV Infection and MenDokument4 SeitenHPV Infection and Menmedicine2life100% (1)