Das könnte Ihnen auch gefallen
- Cardioembolic StrokeDokument3 SeitenCardioembolic StrokeJeffri Sofian LeksanaNoch keine Bewertungen
- IM - Heart Failure Part 1Dokument6 SeitenIM - Heart Failure Part 1Elisha BernabeNoch keine Bewertungen
- Essensial Hypertension Pathogenesis and PathophsiologyDokument22 SeitenEssensial Hypertension Pathogenesis and PathophsiologyAmeliana KamaludinNoch keine Bewertungen
- 2008 2 92 PDFDokument8 Seiten2008 2 92 PDFdidiNoch keine Bewertungen
- Essential Hypertension Pathogen Es Is and Path o PhysiologyDokument23 SeitenEssential Hypertension Pathogen Es Is and Path o Physiology1910149 Yemima Elshantika SyNoch keine Bewertungen
- Essential (Primary) Hypertension: Lectгurer - prof. Yu.R. KovalevDokument36 SeitenEssential (Primary) Hypertension: Lectгurer - prof. Yu.R. Kovalevalfaz lakhaniNoch keine Bewertungen
- FCA Hipertensiva Viau2015Dokument8 SeitenFCA Hipertensiva Viau2015gioandregabNoch keine Bewertungen
- Jurnal Anes 1Dokument7 SeitenJurnal Anes 1Chanvira Aria CandrayanaNoch keine Bewertungen
- Antihypertensive Drug LongDokument21 SeitenAntihypertensive Drug Longa.muhsinNoch keine Bewertungen
- Healing Hypertension: A Focus On Alternative Systems of MedicineDokument10 SeitenHealing Hypertension: A Focus On Alternative Systems of Medicinedeepa rNoch keine Bewertungen
- Hypotension: Sandeep Sharma Priyanka T. BhattacharyaDokument10 SeitenHypotension: Sandeep Sharma Priyanka T. Bhattacharyaمحمود محمدNoch keine Bewertungen
- Hipotensi PDFDokument6 SeitenHipotensi PDFimahNoch keine Bewertungen
- Drugs For Cardiovascular DiseasesDokument74 SeitenDrugs For Cardiovascular Diseasesmjd13mjd4Noch keine Bewertungen
- Pathophysiology Diagnosis and Treatment of Orthostatic Hypotension and Vasovagal Syncope1Dokument17 SeitenPathophysiology Diagnosis and Treatment of Orthostatic Hypotension and Vasovagal Syncope1Idha ANoch keine Bewertungen
- AnnCardAnaesth10119-300904 082130 PDFDokument8 SeitenAnnCardAnaesth10119-300904 082130 PDFFirah Triple'sNoch keine Bewertungen
- Mitchell 2005Dokument8 SeitenMitchell 2005DianNoch keine Bewertungen
- Articulo 1 HTADokument15 SeitenArticulo 1 HTAMateo VisbalNoch keine Bewertungen
- Pathophysiology of Congenital Heart Diseases PDFDokument8 SeitenPathophysiology of Congenital Heart Diseases PDFkishanNoch keine Bewertungen
- Pathophysiology of Congenital Heart Diseases PDFDokument8 SeitenPathophysiology of Congenital Heart Diseases PDFdramitjainNoch keine Bewertungen
- Heart FailureDokument8 SeitenHeart FailureSophia MarieNoch keine Bewertungen
- Conginital Heart DiseaseDokument19 SeitenConginital Heart DiseaseSanthosh.S.UNoch keine Bewertungen
- 3 FullDokument13 Seiten3 Fullمحمد رافد لطيفNoch keine Bewertungen
- Health Teaching PlanDokument6 SeitenHealth Teaching PlanLay YoungNoch keine Bewertungen
- Hypertension: Hypertension Is One of The Most Common Worldwide Diseases Afflicting Humans. BecauseDokument8 SeitenHypertension: Hypertension Is One of The Most Common Worldwide Diseases Afflicting Humans. BecauseKramojNoch keine Bewertungen
- Hypertension: Nursing Care PlansDokument7 SeitenHypertension: Nursing Care PlansSamah AdnanNoch keine Bewertungen
- Clinmed 21 3 E275Dokument8 SeitenClinmed 21 3 E275Carlos CoronaNoch keine Bewertungen
- Pharmacological Therapy of Portal HypertensionDokument8 SeitenPharmacological Therapy of Portal HypertensionSisiliana KristinNoch keine Bewertungen
- HipotensiDokument12 SeitenHipotensiAfdhalia Khairunnisa SyammarhanNoch keine Bewertungen
- LP HypertentionDokument16 SeitenLP HypertentionFitria NorkhalidaNoch keine Bewertungen
- HypertensionDokument15 SeitenHypertensiondeaNoch keine Bewertungen
- Hypertensive Crisis PathoDokument4 SeitenHypertensive Crisis PathoJanelle Dela CruzNoch keine Bewertungen
- Hypertension Is Not A Disease of The Left Arm: A Difficult Diagnosis of Hypertension in Takayasu's ArteritisDokument3 SeitenHypertension Is Not A Disease of The Left Arm: A Difficult Diagnosis of Hypertension in Takayasu's ArteritisvkphyNoch keine Bewertungen
- Cardiovascular DysfunctionDokument15 SeitenCardiovascular DysfunctionJhasseryne Orias SanchezNoch keine Bewertungen
- HypertensionDokument10 SeitenHypertensionagus fetal mein feraldNoch keine Bewertungen
- Hypertensiveemergencies PDFDokument7 SeitenHypertensiveemergencies PDFGede AdiNoch keine Bewertungen
- Case IchDokument4 SeitenCase IchsteffiNoch keine Bewertungen
- Tgs Bhs InggrisDokument22 SeitenTgs Bhs InggrisHarda DedaliNoch keine Bewertungen
- Calixtro, Narrative HypertensionDokument2 SeitenCalixtro, Narrative HypertensionKim SunooNoch keine Bewertungen
- In Partial Fulfillment of The Requirements in Medical Ward RotationDokument5 SeitenIn Partial Fulfillment of The Requirements in Medical Ward RotationEiz CabreraNoch keine Bewertungen
- Diff DS AH - Eh. TreatmentDokument80 SeitenDiff DS AH - Eh. TreatmentCastleKGNoch keine Bewertungen
- Hall 2013Dokument6 SeitenHall 2013Julio Orallo MartínezNoch keine Bewertungen
- Pulmonary HypertensionDokument26 SeitenPulmonary Hypertensionakoeljames8543Noch keine Bewertungen
- Heart FailureDokument13 SeitenHeart Failuremildred alidon100% (2)
- Hypertensive Heart Disease: Hypertension Curriculum ReviewDokument8 SeitenHypertensive Heart Disease: Hypertension Curriculum ReviewPricilia OliveNoch keine Bewertungen
- Pa Tho Physiology of Essential HypertensionDokument5 SeitenPa Tho Physiology of Essential HypertensionassilamorNoch keine Bewertungen
- Chapter 1Dokument12 SeitenChapter 1Niña MoradaNoch keine Bewertungen
- Orthostatic HypertensionDokument8 SeitenOrthostatic HypertensionCharalampidis KonstantinosNoch keine Bewertungen
- Posterior Reversible Encephalopathy SyndromeDokument9 SeitenPosterior Reversible Encephalopathy SyndromejuanmontoyaseNoch keine Bewertungen
- HT RenovascularDokument8 SeitenHT Renovascularsilviagonzalez9007Noch keine Bewertungen
- 01 Cir 42 2 297Dokument11 Seiten01 Cir 42 2 297Abdurrahman Arsyad As SiddiqiNoch keine Bewertungen
- Shock 2024Dokument13 SeitenShock 2024eavasiNoch keine Bewertungen
- Manejo de La Insufiencia Cardica HtaDokument10 SeitenManejo de La Insufiencia Cardica HtaNeiny FonsecaNoch keine Bewertungen
- Hypertension Pathophysiology and Treatment PDFDokument6 SeitenHypertension Pathophysiology and Treatment PDFBella TogasNoch keine Bewertungen
- Rossano2014 PDFDokument6 SeitenRossano2014 PDFAditya SanjayaNoch keine Bewertungen
- Hypertension: S F Vascular SystemDokument12 SeitenHypertension: S F Vascular SystemSNoch keine Bewertungen
- CHF and CardiomyopathiesDokument8 SeitenCHF and CardiomyopathiesDan HoNoch keine Bewertungen
- Renal Artery StenosisDokument3 SeitenRenal Artery StenosisauxtalleriocomNoch keine Bewertungen
- Portal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandPortal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Heart Failure & Cor PulmunaleDokument12 SeitenHeart Failure & Cor PulmunaleShrestha AnjivNoch keine Bewertungen
- Materi Koas GinjalDokument30 SeitenMateri Koas GinjalRichard 151289Noch keine Bewertungen
- Diuretics: Venous Vasodilators (E.g., Nitrates) IncreaseDokument4 SeitenDiuretics: Venous Vasodilators (E.g., Nitrates) IncreasedeanNoch keine Bewertungen
- Week 5 1Dokument6 SeitenWeek 5 1deanNoch keine Bewertungen
- Disease Adalah Suatu Kelainan Formasi Dari JantungDokument5 SeitenDisease Adalah Suatu Kelainan Formasi Dari JantungdeanNoch keine Bewertungen
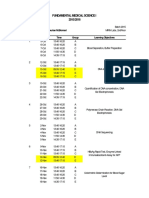
- FMS1 MRIN Lab Schedule - Revisi21sepDokument1 SeiteFMS1 MRIN Lab Schedule - Revisi21sepdeanNoch keine Bewertungen
- Endocardium. The Subendocardial TissueDokument8 SeitenEndocardium. The Subendocardial TissuedeanNoch keine Bewertungen
- FMS1 Schedule 2015 - Revisi21sepDokument3 SeitenFMS1 Schedule 2015 - Revisi21sepdeanNoch keine Bewertungen
- 2015/2016 Fundamental Medical Science I: Cytology Lab Batch 2015 Coordinator: DR Jan Tambayong FK UPH Labs, 3rd FloorDokument1 Seite2015/2016 Fundamental Medical Science I: Cytology Lab Batch 2015 Coordinator: DR Jan Tambayong FK UPH Labs, 3rd FloordeanNoch keine Bewertungen
- Jadwal CTB Revisi 10 Agustus 2015Dokument2 SeitenJadwal CTB Revisi 10 Agustus 2015deanNoch keine Bewertungen
- Impacts of Antibiotic ResistanceDokument3 SeitenImpacts of Antibiotic ResistanceSajid RahimNoch keine Bewertungen
- Cerebral Palsy in ChildrenDokument7 SeitenCerebral Palsy in ChildrenKelvin FundiNoch keine Bewertungen
- Dengue Fever (Nepal) An Emerging Public Health Problem.Dokument13 SeitenDengue Fever (Nepal) An Emerging Public Health Problem.Bzay DhitalNoch keine Bewertungen
- Microbiology Question PapersDokument100 SeitenMicrobiology Question Papersprinceej92% (13)
- TESDA COVID-19 Test (Answer Keys)Dokument12 SeitenTESDA COVID-19 Test (Answer Keys)ash mizushiNoch keine Bewertungen
- EAU 2022 - Prostate CancerDokument229 SeitenEAU 2022 - Prostate Cancerpablo penguinNoch keine Bewertungen
- Breast Abscess ManagementDokument10 SeitenBreast Abscess Managementطلال العمريNoch keine Bewertungen
- Nimhans Previous QuestionDokument51 SeitenNimhans Previous QuestionravasoNoch keine Bewertungen
- Result Analysis Date: November 22, 2017 Conclusion: V. Laboratories and Diagnostic ExamsDokument7 SeitenResult Analysis Date: November 22, 2017 Conclusion: V. Laboratories and Diagnostic ExamsEllaine Joy Mesina PadizNoch keine Bewertungen
- Rectal ProlapseDokument2 SeitenRectal ProlapseSalem ZoghbyNoch keine Bewertungen
- List of Diseases & Afflictions: Intestinal Parasites (Stalker & Interloper)Dokument2 SeitenList of Diseases & Afflictions: Intestinal Parasites (Stalker & Interloper)Alex Vikingoviejo SchmidtNoch keine Bewertungen
- I. Ecologic Model A. HypothesisDokument5 SeitenI. Ecologic Model A. HypothesisTintin LevidaNoch keine Bewertungen
- Chapter 20 Prep U.odtDokument9 SeitenChapter 20 Prep U.odtShade ElugbajuNoch keine Bewertungen
- Feline Anemia Diagnostic AlgorithmDokument1 SeiteFeline Anemia Diagnostic AlgorithmEd BlackadderNoch keine Bewertungen
- Virulence Factors of Streptococcus PyogenesDokument6 SeitenVirulence Factors of Streptococcus PyogenesAmador GielasNoch keine Bewertungen
- Hand Washing Lesson PlanDokument9 SeitenHand Washing Lesson PlanLisa GurreaNoch keine Bewertungen
- Baru Standar 7 S3ffkuh9brs1219brDokument191 SeitenBaru Standar 7 S3ffkuh9brs1219brjumrainiNoch keine Bewertungen
- PRECIO PromalabDokument6 SeitenPRECIO PromalabJenny QuingaNoch keine Bewertungen
- Connors and Other ADHD ScalesDokument3 SeitenConnors and Other ADHD ScalesPragnya NidugondaNoch keine Bewertungen
- Cancer ReportDokument9 SeitenCancer Reportcool_stud_waliNoch keine Bewertungen
- Antimalarial DrugsDokument7 SeitenAntimalarial DrugsHilmanNoch keine Bewertungen
- How To Diagnose LBP RevisiDokument65 SeitenHow To Diagnose LBP RevisiDedy SavradinataNoch keine Bewertungen
- Bpad 051822Dokument32 SeitenBpad 051822Shubhrima KhanNoch keine Bewertungen
- Pasteur Vs Bechamp - An Alternative View of Infectious DiseaseDokument3 SeitenPasteur Vs Bechamp - An Alternative View of Infectious DiseaseRadhe GovindaNoch keine Bewertungen
- Pancreatitis: Pancreatitis Is Inflammation of The Pancreas. It Occurs When Pancreatic Enzymes (Especially Trypsin)Dokument6 SeitenPancreatitis: Pancreatitis Is Inflammation of The Pancreas. It Occurs When Pancreatic Enzymes (Especially Trypsin)tianallyNoch keine Bewertungen
- Emergency Nursing IntroDokument111 SeitenEmergency Nursing IntroteuuuuNoch keine Bewertungen
- KSC WSSforKSCCQIDokument34 SeitenKSC WSSforKSCCQILệnhHồXungNoch keine Bewertungen
- The Child With Endocrine DysfunctionDokument5 SeitenThe Child With Endocrine Dysfunctionhenny1620Noch keine Bewertungen
- Dr. Mohammad Shaikhani. Sulaimani University, College of Medicine. Sulaimanya-Iraqi KurdistanDokument51 SeitenDr. Mohammad Shaikhani. Sulaimani University, College of Medicine. Sulaimanya-Iraqi KurdistanHNINNoch keine Bewertungen
- Oceanic Question Bank Year 4Dokument358 SeitenOceanic Question Bank Year 4maryNoch keine Bewertungen