Das könnte Ihnen auch gefallen
- ArticuloDokument5 SeitenArticuloJuliana Nathaly SanabriaNoch keine Bewertungen
- Revised AugustDokument20 SeitenRevised AugustOsman AitaNoch keine Bewertungen
- Audit Procedures For Vessels: August 2017Dokument22 SeitenAudit Procedures For Vessels: August 2017bridelNoch keine Bewertungen
- South Africa’s Renewable Energy IPP Procurement ProgramVon EverandSouth Africa’s Renewable Energy IPP Procurement ProgramNoch keine Bewertungen
- Privman Gorshkov ReviewDokument13 SeitenPrivman Gorshkov ReviewГорослав КоманчоNoch keine Bewertungen
- Pollution Prevention: Methodology, Technologies and PracticesVon EverandPollution Prevention: Methodology, Technologies and PracticesNoch keine Bewertungen
- CDC 21304 DS1sDokument37 SeitenCDC 21304 DS1sDecendio Rosa Trindade WarilaNoch keine Bewertungen
- Odontologia Woelfel Anatomia Dental 2018Dokument504 SeitenOdontologia Woelfel Anatomia Dental 2018Herry Portocarrero Castillo85% (34)
- CS 468 Revision 1 Assessment of Freyssinet Concrete Hinges in Highway Structures-WebDokument29 SeitenCS 468 Revision 1 Assessment of Freyssinet Concrete Hinges in Highway Structures-WebThong NguyenNoch keine Bewertungen
- Sb477bennettlaw Patternspdfpdf PDF FreeDokument62 SeitenSb477bennettlaw Patternspdfpdf PDF FreeGolden Path ExponentialNoch keine Bewertungen
- Must Read For Surgery Clerkship Procedure ManualDokument33 SeitenMust Read For Surgery Clerkship Procedure ManualTrisNoch keine Bewertungen
- Macroura) Harvest And: Mourning Dove (Zenaida Population Parameters Derived From A National Banding StudyDokument57 SeitenMacroura) Harvest And: Mourning Dove (Zenaida Population Parameters Derived From A National Banding Studyapi-252580560Noch keine Bewertungen
- Handbook For Cell Culture Basics (Gibco)Dokument62 SeitenHandbook For Cell Culture Basics (Gibco)Cesar PuentesNoch keine Bewertungen
- Well Testing SLBDokument25 SeitenWell Testing SLBfergot2010Noch keine Bewertungen
- WP Creating Maintaining Soc PDFDokument16 SeitenWP Creating Maintaining Soc PDFgeo36Noch keine Bewertungen
- PDF Filter Separator Vessel Manual DLDokument40 SeitenPDF Filter Separator Vessel Manual DLRosa SparksNoch keine Bewertungen
- Process Simulation Model For A Staged, Fluidized-Bed Oil-Shale Retort With Lift-Pipe CombustorDokument31 SeitenProcess Simulation Model For A Staged, Fluidized-Bed Oil-Shale Retort With Lift-Pipe CombustorAljay Neeson ImperialNoch keine Bewertungen
- Diclofenac For Acute Pain in Children (Review) - Cochrane 2009Dokument63 SeitenDiclofenac For Acute Pain in Children (Review) - Cochrane 2009Carlos CuetoNoch keine Bewertungen
- Standards For Improving Quality of Maternaland Newborn Care in Health FacilitiesDokument84 SeitenStandards For Improving Quality of Maternaland Newborn Care in Health FacilitiesBettyUgazNoch keine Bewertungen
- ManualDokument62 SeitenManualMelissa CastañedaNoch keine Bewertungen
- Cell Culture BasicsDokument61 SeitenCell Culture BasicsLidia EscutiaNoch keine Bewertungen
- Ultrasound Versus Liver Function Tests For Diagnosis of Common Bile Duct Stones (Review)Dokument57 SeitenUltrasound Versus Liver Function Tests For Diagnosis of Common Bile Duct Stones (Review)FlipNoch keine Bewertungen
- CBMT HandbookDokument25 SeitenCBMT Handbookhousi73Noch keine Bewertungen
- MD Codes BookletDokument50 SeitenMD Codes Bookletoliver rdz100% (29)
- Recordall® Turbo Series Meters: User ManualDokument16 SeitenRecordall® Turbo Series Meters: User Manualخوسيه لويس فرنانديزNoch keine Bewertungen
- Natural Experiments GuidanceDokument29 SeitenNatural Experiments GuidancelordNoch keine Bewertungen
- Sae Uscar45 - 2018Dokument22 SeitenSae Uscar45 - 2018Salafi Mhmd100% (1)
- CD 362 Enclosure of Bridges-WebDokument27 SeitenCD 362 Enclosure of Bridges-Webyanxi liuNoch keine Bewertungen
- Gibco Cell Culture Basics Handbook Global PDFDokument120 SeitenGibco Cell Culture Basics Handbook Global PDFKARINA ALEXANDRA PARRA HARONoch keine Bewertungen
- CD 362 Revision 1 Enclosure of Bridges-WebDokument27 SeitenCD 362 Revision 1 Enclosure of Bridges-WebAbinashNoch keine Bewertungen
- Lateral Static LoadDokument87 SeitenLateral Static LoadMuhammad Nur AkromuzzamanNoch keine Bewertungen
- Tuberculosis Infection: Gamma Interferon Release Assays For Detection of MycobacteriumDokument18 SeitenTuberculosis Infection: Gamma Interferon Release Assays For Detection of MycobacteriumLinda MaylianaNoch keine Bewertungen
- Nclex-Rn Test Plan: Effective April 2023Dokument59 SeitenNclex-Rn Test Plan: Effective April 2023GjbNoch keine Bewertungen
- Ameloblastoma A RetDokument6 SeitenAmeloblastoma A RetFranco FrancoNoch keine Bewertungen
- Din 5480Dokument27 SeitenDin 5480MiguelNoch keine Bewertungen
- Rizzieri 2016Dokument13 SeitenRizzieri 2016alinamatei1000000Noch keine Bewertungen
- 2023 - PN - Test Plan - FINALDokument56 Seiten2023 - PN - Test Plan - FINALMuhammad Tahir SaleemNoch keine Bewertungen
- Jet Aerator InstallationDokument12 SeitenJet Aerator InstallationAmin SmileyNoch keine Bewertungen
- "BEST": Biochemical Engineering Simulation Technology: NRE /MPDokument23 Seiten"BEST": Biochemical Engineering Simulation Technology: NRE /MPSachini SarthchandraNoch keine Bewertungen
- Atresia Elsefier Overview 2014Dokument4 SeitenAtresia Elsefier Overview 2014Abigail Wahyu ArdiyantiNoch keine Bewertungen
- Project Report PDFDokument50 SeitenProject Report PDFvinoth devaNoch keine Bewertungen
- Science Olympics BookletDokument87 SeitenScience Olympics BookletShaun WildeNoch keine Bewertungen
- Geophysical Methods To Detect Stress in Underground Mines: Report of Investigations/2004Dokument23 SeitenGeophysical Methods To Detect Stress in Underground Mines: Report of Investigations/2004wypoNoch keine Bewertungen
- Sense 2nd Gen User Guide Win PDFDokument17 SeitenSense 2nd Gen User Guide Win PDFcclaureNoch keine Bewertungen
- Operative Versus Non-Operative Treatment For Thoracolumbar Burst Fractures Without Neurological Deficit (Review)Dokument18 SeitenOperative Versus Non-Operative Treatment For Thoracolumbar Burst Fractures Without Neurological Deficit (Review)Tarib TrifaNoch keine Bewertungen
- Glosar European de Restaurare IcoanaDokument450 SeitenGlosar European de Restaurare IcoanaVioleta ScarlatNoch keine Bewertungen
- CD 523 Determination of Pipe Roughness and Assessment of Sediment Deposition To Aid Pipeline Design Version 1.1.0Dokument54 SeitenCD 523 Determination of Pipe Roughness and Assessment of Sediment Deposition To Aid Pipeline Design Version 1.1.0Pranav KumarNoch keine Bewertungen
- CD 358 Waterproofing and Surfacing of Concrete Bridge Decks-WebDokument63 SeitenCD 358 Waterproofing and Surfacing of Concrete Bridge Decks-WebJorge Baños LloredoNoch keine Bewertungen
- OCT and GlaucomaDokument276 SeitenOCT and GlaucomaMarta G. HadidNoch keine Bewertungen
- Sharif 2015Dokument15 SeitenSharif 2015shehla khanNoch keine Bewertungen
- Marine-Shuttle-Tanker-Advisory 2020Dokument49 SeitenMarine-Shuttle-Tanker-Advisory 2020KosNoch keine Bewertungen
- Ger 3954c Generator in Situ InspectionsDokument16 SeitenGer 3954c Generator in Situ InspectionsMisdehRasmanNoch keine Bewertungen
- BulkLite Product Manual WsDokument30 SeitenBulkLite Product Manual WsHafez AymanNoch keine Bewertungen
- CPHQ Examination Hand BookDokument26 SeitenCPHQ Examination Hand BookRichu Pali100% (1)
- CPHQ Cert HandbookDokument26 SeitenCPHQ Cert HandbookRichu PaliNoch keine Bewertungen
- Ger 3954c Generator in Situ InspectionsDokument16 SeitenGer 3954c Generator in Situ InspectionsAnonymous veyW4YWjkNoch keine Bewertungen
- Jordan 1Dokument5 SeitenJordan 1thiên lữNoch keine Bewertungen
- A Controversy With Respect To Occlusion: Japanese Dental Science ReviewDokument5 SeitenA Controversy With Respect To Occlusion: Japanese Dental Science Reviewthiên lữNoch keine Bewertungen
- MCQ - Three Questions Vs Four QuestionsDokument4 SeitenMCQ - Three Questions Vs Four Questionsthiên lữNoch keine Bewertungen
- Clinical Issues in Occlusion - Part I: ReviewDokument8 SeitenClinical Issues in Occlusion - Part I: Reviewthiên lữNoch keine Bewertungen
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDokument35 SeitenWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientiststhiên lữNoch keine Bewertungen
- Tongue Function Is Important For Masticatory Performance in The Healthy Elderly: A Cross-Sectional Survey of Community-Dwelling ElderlyDokument4 SeitenTongue Function Is Important For Masticatory Performance in The Healthy Elderly: A Cross-Sectional Survey of Community-Dwelling Elderlythiên lữNoch keine Bewertungen
- 1.the Influence of Occlusion On Jaw and Neck Muscle Activity - A Surface EMG Study in Healthy Young AdultsDokument8 Seiten1.the Influence of Occlusion On Jaw and Neck Muscle Activity - A Surface EMG Study in Healthy Young Adultsthiên lữNoch keine Bewertungen
- Obtaining Measurable Bilateral Simultaneous Occlusal Contacts With Computer-Analyzed and Guided Occlusal AdjustmentsDokument12 SeitenObtaining Measurable Bilateral Simultaneous Occlusal Contacts With Computer-Analyzed and Guided Occlusal Adjustmentsthiên lữNoch keine Bewertungen
- 5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal OcclusionsDokument7 Seiten5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal Occlusionsthiên lữNoch keine Bewertungen
- 5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal OcclusionsDokument5 Seiten5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal Occlusionsthiên lữNoch keine Bewertungen
- Predictable Prosthetic Space Maintenance During Staged Complete-Mouth RehabilitationDokument6 SeitenPredictable Prosthetic Space Maintenance During Staged Complete-Mouth Rehabilitationthiên lữNoch keine Bewertungen
- Systematic Assessment of The Various ControversiesDokument7 SeitenSystematic Assessment of The Various Controversiesthiên lữNoch keine Bewertungen
- 5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal OcclusionsDokument5 Seiten5.occlusal Risk Factors Associated With Temporomandibular Disorders in Young Adults With Normal Occlusionsthiên lữNoch keine Bewertungen
- 6.neuromuscular Function in Healthy OcclusionDokument7 Seiten6.neuromuscular Function in Healthy Occlusionthiên lữNoch keine Bewertungen
- 12.relative Contributions of Occlusion, Maximum Bite Force, and Chewing Cycle Kinematics To Masticatory PerformanceDokument8 Seiten12.relative Contributions of Occlusion, Maximum Bite Force, and Chewing Cycle Kinematics To Masticatory Performancethiên lữNoch keine Bewertungen
- 7.occlusal Measurement Method Can Affect SEMG Activity During OcclusionDokument6 Seiten7.occlusal Measurement Method Can Affect SEMG Activity During Occlusionthiên lữNoch keine Bewertungen
- 8.occlusal Force Distribution On The Dental Arch During Various Levels of ClenchingDokument4 Seiten8.occlusal Force Distribution On The Dental Arch During Various Levels of Clenchingthiên lữNoch keine Bewertungen
- Disclusion Time Measurement Studies A Comparison oDokument10 SeitenDisclusion Time Measurement Studies A Comparison othiên lữNoch keine Bewertungen
- How To Write MCQ QuestionsDokument5 SeitenHow To Write MCQ Questionsthiên lữNoch keine Bewertungen
- Journal of Electromyography and Kinesiology: Bao-Yong Li, Li-Juan Zhou, Shao-Xiong Guo, Yuan Zhang, Lei Lu, Mei-Qing WangDokument9 SeitenJournal of Electromyography and Kinesiology: Bao-Yong Li, Li-Juan Zhou, Shao-Xiong Guo, Yuan Zhang, Lei Lu, Mei-Qing Wangthiên lữNoch keine Bewertungen
- 11.a Possible Biomechanical Role of Occlusal Cusp-Fossa Contact RelationshipsDokument11 Seiten11.a Possible Biomechanical Role of Occlusal Cusp-Fossa Contact Relationshipsthiên lữNoch keine Bewertungen
- A Device For Occlusal Plane DeterminationDokument4 SeitenA Device For Occlusal Plane Determinationthiên lữNoch keine Bewertungen
- SAT Practice Test 10 - College BoardDokument34 SeitenSAT Practice Test 10 - College BoardAdissaya BEAM S.Noch keine Bewertungen
- Exercise On Word Formation 2 (Unit 2 - Advanced) : Tran Dai Nghia High School For The GiftedDokument3 SeitenExercise On Word Formation 2 (Unit 2 - Advanced) : Tran Dai Nghia High School For The GiftedEveryonehateshiuzo 2.0Noch keine Bewertungen
- Adaptive Reuse Architecture Documentation and Analysis 2168 9717 1000172Dokument9 SeitenAdaptive Reuse Architecture Documentation and Analysis 2168 9717 1000172Komal HundiaNoch keine Bewertungen
- Comparative Study On Serial and Parallel Manipulators - ReviewDokument23 SeitenComparative Study On Serial and Parallel Manipulators - ReviewShaik Himam SahebNoch keine Bewertungen
- Theoretical CyclesDokument49 SeitenTheoretical CyclesMariaEzzaSyUyNoch keine Bewertungen
- Bravo MRI II Operation ManualDokument45 SeitenBravo MRI II Operation ManualLuis100% (1)
- Maintenance Páginas-509-580Dokument72 SeitenMaintenance Páginas-509-580Alexandra Gabriela Pacheco PrietoNoch keine Bewertungen
- Ict 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Dokument14 SeitenIct 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Chiropractic Marketing NowNoch keine Bewertungen
- Badminton ReviewerDokument10 SeitenBadminton ReviewerHailsey WinterNoch keine Bewertungen
- Crma Unit 1 Crma RolesDokument34 SeitenCrma Unit 1 Crma Rolesumop3plsdn0% (1)
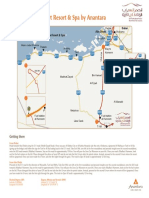
- Qasr Al Sarab Desert Resort Location Map June2012Dokument1 SeiteQasr Al Sarab Desert Resort Location Map June2012Anant GârgNoch keine Bewertungen
- Pusheen With Donut: Light Grey, Dark Grey, Brown, RoséDokument13 SeitenPusheen With Donut: Light Grey, Dark Grey, Brown, RosémafaldasNoch keine Bewertungen
- Valdez, Shenny RoseDokument3 SeitenValdez, Shenny Roseyeng botzNoch keine Bewertungen
- Basics of Population EducationDokument4 SeitenBasics of Population EducationLAILANIE DELA PENANoch keine Bewertungen
- Clinical Biomechanics: Leigh W. Marshall, Stuart M. McgillDokument4 SeitenClinical Biomechanics: Leigh W. Marshall, Stuart M. McgillMichael JunNoch keine Bewertungen
- ff2023 Web 0 0Dokument2 Seitenff2023 Web 0 0khaing khantNoch keine Bewertungen
- FBC MNCS Service-, Error-, Infocodes ENDokument23 SeitenFBC MNCS Service-, Error-, Infocodes ENDragos Stoian100% (1)
- TM 10-3930-669-34 Forklift Truck 6K Drexel MDL R60SL-DC Part 1Dokument294 SeitenTM 10-3930-669-34 Forklift Truck 6K Drexel MDL R60SL-DC Part 1AdvocateNoch keine Bewertungen
- Islam and Civilization (Analysis Study On The History of Civilization in Islam) Muhammad Hifdil IslamDokument18 SeitenIslam and Civilization (Analysis Study On The History of Civilization in Islam) Muhammad Hifdil IslamLoveth KonniaNoch keine Bewertungen
- 3 Curvilinear MotionDokument50 Seiten3 Curvilinear Motiongarhgelh100% (1)
- 988611457NK448908 Vehicle Scan ReportDokument5 Seiten988611457NK448908 Vehicle Scan ReportVictor Daniel Piñeros ZubietaNoch keine Bewertungen
- Daftar PustakaDokument3 SeitenDaftar PustakaMel DaNoch keine Bewertungen
- Raneem AlbazazDokument33 SeitenRaneem AlbazazGordana PuzovicNoch keine Bewertungen
- EDS-A-0101: Automotive Restricted Hazardous Substances For PartsDokument14 SeitenEDS-A-0101: Automotive Restricted Hazardous Substances For PartsMuthu GaneshNoch keine Bewertungen
- Chapter 7 Dopant Diffusion - IDokument32 SeitenChapter 7 Dopant Diffusion - I강준호Noch keine Bewertungen
- Indoor Air Quality Standard Procedures - 2014 RevDokument12 SeitenIndoor Air Quality Standard Procedures - 2014 RevFioriAmeliaHathawayNoch keine Bewertungen
- Free Electron TheoryDokument8 SeitenFree Electron TheoryNeelam KapoorNoch keine Bewertungen
- 9A02502 Transmission of Electric PowerDokument6 Seiten9A02502 Transmission of Electric PowersivabharathamurthyNoch keine Bewertungen
- Orbitol Motor TMTHWDokument20 SeitenOrbitol Motor TMTHWRodolfo ErenoNoch keine Bewertungen
- Reynold A. Nicholson - The Mystics of IslamDokument65 SeitenReynold A. Nicholson - The Mystics of IslamLuminon SamanNoch keine Bewertungen
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissVon EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissBewertung: 4.5 von 5 Sternen4.5/5 (81)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningVon EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningBewertung: 4 von 5 Sternen4/5 (3)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipVon EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipBewertung: 4.5 von 5 Sternen4.5/5 (1135)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerVon EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerBewertung: 4.5 von 5 Sternen4.5/5 (58)
- Breaking the Habit of Being YourselfVon EverandBreaking the Habit of Being YourselfBewertung: 4.5 von 5 Sternen4.5/5 (1458)
- Forever Strong: A New, Science-Based Strategy for Aging WellVon EverandForever Strong: A New, Science-Based Strategy for Aging WellNoch keine Bewertungen
- Really Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityVon EverandReally Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityBewertung: 5 von 5 Sternen5/5 (28)
- Peaceful Sleep Hypnosis: Meditate & RelaxVon EverandPeaceful Sleep Hypnosis: Meditate & RelaxBewertung: 4.5 von 5 Sternen4.5/5 (142)
- Love Yourself, Heal Your Life Workbook (Insight Guide)Von EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Bewertung: 5 von 5 Sternen5/5 (40)
- Gut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Von EverandGut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Bewertung: 4.5 von 5 Sternen4.5/5 (20)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayVon EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNoch keine Bewertungen
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Deep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Von EverandDeep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Bewertung: 4.5 von 5 Sternen4.5/5 (10)
- Deep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellVon EverandDeep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellBewertung: 5 von 5 Sternen5/5 (8)
- Heal: Discover Your Unlimited Potential and Awaken the Powerful Healer WithinVon EverandHeal: Discover Your Unlimited Potential and Awaken the Powerful Healer WithinBewertung: 5 von 5 Sternen5/5 (38)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingVon EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingBewertung: 4.5 von 5 Sternen4.5/5 (103)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouVon EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouBewertung: 3.5 von 5 Sternen3.5/5 (5)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookVon EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonVon EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonBewertung: 3.5 von 5 Sternen3.5/5 (33)
- Fast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperVon EverandFast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperBewertung: 4.5 von 5 Sternen4.5/5 (15)
- 369: Manifesting Through 369 and the Law of Attraction - METHODS, TECHNIQUES AND EXERCISESVon Everand369: Manifesting Through 369 and the Law of Attraction - METHODS, TECHNIQUES AND EXERCISESBewertung: 5 von 5 Sternen5/5 (50)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeVon EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeBewertung: 3.5 von 5 Sternen3.5/5 (13)
- Summary of You Can Heal Your Life by Louise HayVon EverandSummary of You Can Heal Your Life by Louise HayBewertung: 4.5 von 5 Sternen4.5/5 (69)