Das könnte Ihnen auch gefallen
- DiscoDokument19 SeitenDiscovcuadrosvNoch keine Bewertungen
- Adaptive Behavior Profiles in Autism Spectrum Disorders: DisclosuresDokument14 SeitenAdaptive Behavior Profiles in Autism Spectrum Disorders: DisclosuresAbd El-RahmanNoch keine Bewertungen
- ASD Manual PDFDokument15 SeitenASD Manual PDFEzri Mariveles Coda Jr.100% (1)
- DSM 5 ASD ChecklistDokument2 SeitenDSM 5 ASD ChecklistPuabNoch keine Bewertungen
- AUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONDokument5 SeitenAUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONvai2Noch keine Bewertungen
- Example M3 Report 2019Dokument7 SeitenExample M3 Report 2019EverestNoch keine Bewertungen
- Vineland AutismDokument17 SeitenVineland AutismfabcardososNoch keine Bewertungen
- Asd AssessmentDokument37 SeitenAsd AssessmentAvi MagiNoch keine Bewertungen
- BBBB, Aaaa Deidentified No ASDDokument16 SeitenBBBB, Aaaa Deidentified No ASDRomina Gisell Trogo100% (1)
- Autism Spectrum DisorderDokument58 SeitenAutism Spectrum DisorderPriscilla ChumrooNoch keine Bewertungen
- ASD Assessment ConsiderationsDokument8 SeitenASD Assessment ConsiderationsAggelou Maya50% (2)
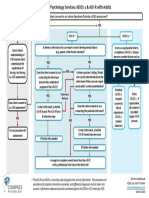
- Compass Psychology Services: ADOS-2 & ADI-R FlowchartDokument1 SeiteCompass Psychology Services: ADOS-2 & ADI-R Flowchartaspire centerNoch keine Bewertungen
- Sample Questions From Diagnostcic ToolsDokument5 SeitenSample Questions From Diagnostcic ToolstracycwNoch keine Bewertungen
- Expo 3 NEPSY II A Developmental Neuropsychological AssessmentDokument23 SeitenExpo 3 NEPSY II A Developmental Neuropsychological AssessmentHugo Cruz LlamasNoch keine Bewertungen
- F.5 Selective Mutism Powerpoint 2016Dokument32 SeitenF.5 Selective Mutism Powerpoint 2016Ptrc Lbr LpNoch keine Bewertungen
- GARS 2 - ArticleDokument20 SeitenGARS 2 - ArticleGoropadNoch keine Bewertungen
- YBOCSDokument21 SeitenYBOCSsnNoch keine Bewertungen
- Collaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeVon EverandCollaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeAlisha R. PollastriNoch keine Bewertungen
- The Effectiveness of RAADS-R As A Screening Tool FDokument6 SeitenThe Effectiveness of RAADS-R As A Screening Tool FCarola ValdésNoch keine Bewertungen
- (Adolescent Version) : Please Tick One Option Per Question OnlyDokument1 Seite(Adolescent Version) : Please Tick One Option Per Question OnlyDIMITRIOSVOLOSNoch keine Bewertungen
- Autism PDFDokument41 SeitenAutism PDFflower21Noch keine Bewertungen
- Autism ScalesDokument33 SeitenAutism Scalesapi-30946491260% (5)
- BOSA Example Clinical SummariesDokument5 SeitenBOSA Example Clinical SummariesMacarena Ignacia Argaluza Guerrero100% (3)
- ADOS ThesisDokument44 SeitenADOS Thesistelopettinilamattina0% (1)
- The Accuracy of The ADOS-2 in Identifying Autism Among Adults With Complex Psychiatric ConditionsDokument14 SeitenThe Accuracy of The ADOS-2 in Identifying Autism Among Adults With Complex Psychiatric ConditionsgatosurferNoch keine Bewertungen
- Early Expression of Autism Spectrum DisordersDokument39 SeitenEarly Expression of Autism Spectrum Disordersjyoti mahajanNoch keine Bewertungen
- Sohn Grayson Rating Scale for Asperger'sDokument4 SeitenSohn Grayson Rating Scale for Asperger'sJovanka SolmosanNoch keine Bewertungen
- Assessment and Diagnosis AutismDokument12 SeitenAssessment and Diagnosis AutismPanaviChughNoch keine Bewertungen
- CPG Management of Autism Spectrum Disorder in Children and Adolescents PDFDokument76 SeitenCPG Management of Autism Spectrum Disorder in Children and Adolescents PDFfatin zulaikha100% (1)
- 'Theory of Mind and Autism: A Review' by Simon Baron-CohenDokument35 Seiten'Theory of Mind and Autism: A Review' by Simon Baron-CohenashworthceeNoch keine Bewertungen
- ASD in DSM5 - Overview of Updates To DSM and ADOS2Dokument27 SeitenASD in DSM5 - Overview of Updates To DSM and ADOS2Erwin Syah100% (1)
- ASD Comparison Information Brief PDFDokument6 SeitenASD Comparison Information Brief PDFMaryam BehramNoch keine Bewertungen
- Emotion Perception Mediates The Predictive Relationship Between Verbal Ability and Functional Outcome in High-Functioning Adults With Autism Spectrum DisorderDokument17 SeitenEmotion Perception Mediates The Predictive Relationship Between Verbal Ability and Functional Outcome in High-Functioning Adults With Autism Spectrum DisorderThamires DiasNoch keine Bewertungen
- Autism Spectrum Disorders Diagnosis and Early IdentificationDokument17 SeitenAutism Spectrum Disorders Diagnosis and Early IdentificationTito100% (4)
- Screening Tools For AutismDokument17 SeitenScreening Tools For AutismivanakraljevicNoch keine Bewertungen
- The Investigation and Differential Diagnosis of Asperger Syndrome in AdultsDokument9 SeitenThe Investigation and Differential Diagnosis of Asperger Syndrome in AdultsamarillonoexpectaNoch keine Bewertungen
- The Camouflaging Autistic Traits Questionnaire (CDokument3 SeitenThe Camouflaging Autistic Traits Questionnaire (Clidicesilveira969Noch keine Bewertungen
- Autism AssessmentDokument37 SeitenAutism AssessmentRafael Martins94% (16)
- M Chat ScoringDokument2 SeitenM Chat ScoringAmir ShenoudaNoch keine Bewertungen
- Discrete Trial TeachingDokument2 SeitenDiscrete Trial TeachingsuisenNoch keine Bewertungen
- Pai Adolescent Sample1Dokument9 SeitenPai Adolescent Sample1diablero999Noch keine Bewertungen
- Autism Screening QuestionnaireDokument3 SeitenAutism Screening QuestionnaireMichelotto Toonomamoueinaikaneís PauloNoch keine Bewertungen
- Students' MetacognitiveDokument11 SeitenStudents' MetacognitiveMicheal LezondraNoch keine Bewertungen
- Social Skills Assessments For Children With Autism Spectrum Disorders 2165 7890.1000122Dokument9 SeitenSocial Skills Assessments For Children With Autism Spectrum Disorders 2165 7890.1000122Shinta SeptiaNoch keine Bewertungen
- Basc-2 Presentation - All SlidesDokument59 SeitenBasc-2 Presentation - All Slidesapi-290174387100% (1)
- Functional Assessment Tool For Behavior PDFDokument2 SeitenFunctional Assessment Tool For Behavior PDFads100% (1)
- Denver Developmental Screening TestDokument8 SeitenDenver Developmental Screening TestEleanor AlmendralNoch keine Bewertungen
- 1asperger Syndrome Diagnostic ScaleDokument1 Seite1asperger Syndrome Diagnostic ScaleAna Leonor BorgesNoch keine Bewertungen
- Autism 206 AymakelidesDokument44 SeitenAutism 206 AymakelidesȘtefana StefiNoch keine Bewertungen
- Autism DyslexiaDokument2 SeitenAutism DyslexiaAutismDyslexiaNoch keine Bewertungen
- Detection and Diagnosis of ASD in Females: Journal of Health Service Psychology February 2020Dokument12 SeitenDetection and Diagnosis of ASD in Females: Journal of Health Service Psychology February 2020Jennifer Soares de Souza de Freitas100% (1)
- DSM 5 Interview ASD EnglishDokument10 SeitenDSM 5 Interview ASD EnglishJacob NotHank FrancisNoch keine Bewertungen
- The Autism-Spectrum Quotient (AQ) : Evidence From Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and MathematiciansDokument13 SeitenThe Autism-Spectrum Quotient (AQ) : Evidence From Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and MathematiciansDamian Maya0% (1)
- 2 - Diagnostic Evaluation of Autism Spectrum DisordersDokument9 Seiten2 - Diagnostic Evaluation of Autism Spectrum DisordersAlice WernecNoch keine Bewertungen
- The Assessment of Executive Functioning in ChildrenDokument37 SeitenThe Assessment of Executive Functioning in ChildrenYovana Estefany Lasso Caicedo100% (1)
- Facilitating Social Inclusion of Children with AutismDokument16 SeitenFacilitating Social Inclusion of Children with AutismZAHRUDIN ZAHIRUDDIN DAUD Moe100% (1)
- A Replication of The Autism Diagnostic Observation Schedule AdosDokument10 SeitenA Replication of The Autism Diagnostic Observation Schedule AdosmayelapsNoch keine Bewertungen
- Autism Spectrum Disorder Final HandoutDokument2 SeitenAutism Spectrum Disorder Final Handoutapi-264629576Noch keine Bewertungen
- Autism Spectrum Disorders Exceptionality ReportDokument29 SeitenAutism Spectrum Disorders Exceptionality Reportapi-272317458Noch keine Bewertungen
- ABA Preference AssessmentDokument6 SeitenABA Preference AssessmentJavier GarciaNoch keine Bewertungen
- Steven Taylor - The Psychology of Pandemics - Preparing For The Next Global Outbreak of Infectious Disease-Cambridge Scholars Publishing (2019) PDFDokument179 SeitenSteven Taylor - The Psychology of Pandemics - Preparing For The Next Global Outbreak of Infectious Disease-Cambridge Scholars Publishing (2019) PDFCaroline Barroso100% (4)
- Farah M.J. Visual AgnosiaDokument207 SeitenFarah M.J. Visual AgnosiaHelen Anyfandi100% (1)
- Matrices Progresivas Escala Coloreada Manual PDFDokument27 SeitenMatrices Progresivas Escala Coloreada Manual PDFMaría LuzNoch keine Bewertungen
- Matrices Progresivas Escala Coloreada Manual PDFDokument27 SeitenMatrices Progresivas Escala Coloreada Manual PDFMaría LuzNoch keine Bewertungen
- The IFS (INECO Frontal Screening) and Level of Education - Normative DataDokument10 SeitenThe IFS (INECO Frontal Screening) and Level of Education - Normative DatavictorpsycheNoch keine Bewertungen
- ACE MahuranathDokument9 SeitenACE MahuranathStephanie Saavedra GomezNoch keine Bewertungen
- Tibon-Czopp & Weiner (2016) The Rorschach Inkblot Method ResearchDokument248 SeitenTibon-Czopp & Weiner (2016) The Rorschach Inkblot Method ResearchTito Aedo Saravia100% (1)
- Actividad Habilidades Sociales ComicsDokument1 SeiteActividad Habilidades Sociales ComicsvictorpsycheNoch keine Bewertungen
- Improving in NeuorpsychologicalDokument13 SeitenImproving in NeuorpsychologicalvictorpsycheNoch keine Bewertungen
- Meyer, Neuropsychological Factors ChildrensDokument21 SeitenMeyer, Neuropsychological Factors ChildrensvictorpsycheNoch keine Bewertungen
- (Personality & Clinical Psychology Series) Ronald J. Ganellen - Integrating The Rorschach and The MMPI-2 in Personality Assessment-Routledge (1996) PDFDokument363 Seiten(Personality & Clinical Psychology Series) Ronald J. Ganellen - Integrating The Rorschach and The MMPI-2 in Personality Assessment-Routledge (1996) PDFvictorpsycheNoch keine Bewertungen
- D KEFSStroopasPVT2018 PDFDokument14 SeitenD KEFSStroopasPVT2018 PDFvictorpsycheNoch keine Bewertungen
- Acklin 1996 Contributions of Cognitive Science To Rorschah TechniqueDokument11 SeitenAcklin 1996 Contributions of Cognitive Science To Rorschah TechniquevictorpsycheNoch keine Bewertungen
- Planilla OspepriDokument2 SeitenPlanilla OspeprivictorpsycheNoch keine Bewertungen
- Jugar para Crecer 1-20181022171937 PDFDokument9 SeitenJugar para Crecer 1-20181022171937 PDFvictorpsycheNoch keine Bewertungen
- Reid J. Meloy - The Psychopathic Mind - Origins, Dynamics, and Treatment-Jason Aronson, Inc. (1988) PDFDokument497 SeitenReid J. Meloy - The Psychopathic Mind - Origins, Dynamics, and Treatment-Jason Aronson, Inc. (1988) PDFvictorpsyche71% (7)
- D KEFSStroopasPVT2018 PDFDokument14 SeitenD KEFSStroopasPVT2018 PDFvictorpsycheNoch keine Bewertungen
- Improving in NeuorpsychologicalDokument13 SeitenImproving in NeuorpsychologicalvictorpsycheNoch keine Bewertungen
- Roebuckspencer2017 PDFDokument8 SeitenRoebuckspencer2017 PDFvictorpsycheNoch keine Bewertungen
- Addressing Bias in Cross-Cultural Neuropsychological TestingDokument36 SeitenAddressing Bias in Cross-Cultural Neuropsychological TestingvictorpsycheNoch keine Bewertungen
- Current Limitation of Tests (2019)Dokument10 SeitenCurrent Limitation of Tests (2019)victorpsycheNoch keine Bewertungen
- Clayton Et Al (2012) HB Env & Con PsyDokument873 SeitenClayton Et Al (2012) HB Env & Con PsyDayse Albuquerque100% (2)
- Roebuckspencer2017 PDFDokument8 SeitenRoebuckspencer2017 PDFvictorpsycheNoch keine Bewertungen
- Urist1982 PDFDokument6 SeitenUrist1982 PDFvictorpsycheNoch keine Bewertungen
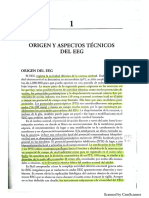
- Libro ElectroencefalografiaDokument19 SeitenLibro ElectroencefalografiavictorpsycheNoch keine Bewertungen
- Mmpi 2 Paper InvestigationDokument15 SeitenMmpi 2 Paper InvestigationvictorpsycheNoch keine Bewertungen
- Improving in NeuorpsychologicalDokument13 SeitenImproving in NeuorpsychologicalvictorpsycheNoch keine Bewertungen
- Gass, The Trail Making Test PaperDokument6 SeitenGass, The Trail Making Test PapervictorpsycheNoch keine Bewertungen
- Clayton Et Al (2012) HB Env & Con PsyDokument873 SeitenClayton Et Al (2012) HB Env & Con PsyDayse Albuquerque100% (2)
- Strategies For Power Calculations in Predictive Biomarker Studies in Survival DataDokument9 SeitenStrategies For Power Calculations in Predictive Biomarker Studies in Survival DataagusjatNoch keine Bewertungen
- ScizopheniaDokument20 SeitenScizopheniaGogea GabrielaNoch keine Bewertungen
- TJW Penile Anatomy and PhysiologyDokument9 SeitenTJW Penile Anatomy and Physiologyhamza shahNoch keine Bewertungen
- DLP in PE 10 Common InjuriesDokument6 SeitenDLP in PE 10 Common InjuriesChristopherArjayCigaral100% (2)
- Human Chromosomes PowerpointDokument16 SeitenHuman Chromosomes Powerpointmihalcea alin50% (2)
- Osteoporose: Laís Gomes - R1 CM Orientação: Dra LucianaDokument23 SeitenOsteoporose: Laís Gomes - R1 CM Orientação: Dra LucianaMichellePeresNoch keine Bewertungen
- Volume5 Number4 Article5Dokument6 SeitenVolume5 Number4 Article5Hafidzoh NajwatiNoch keine Bewertungen
- Liver DiseasesDokument59 SeitenLiver Diseasesडा. सत्यदेव त्यागी आर्यNoch keine Bewertungen
- Wilson - Medical Implications of BiofilmsDokument329 SeitenWilson - Medical Implications of Biofilmsrahuldhodapkar100% (1)
- Chemical Pathology MBCHB Student Lecture Notes 2013Dokument397 SeitenChemical Pathology MBCHB Student Lecture Notes 2013Micky Sunnyraj67% (3)
- Absorption, Distribution, Metabolism, Excretion and Mechanisms of Action of AflatoxinsDokument3 SeitenAbsorption, Distribution, Metabolism, Excretion and Mechanisms of Action of AflatoxinsMaya Innaka ArhayuNoch keine Bewertungen
- The Role of Mutations On Genes NSD1 and NFIX, in Sotos SyndromeDokument4 SeitenThe Role of Mutations On Genes NSD1 and NFIX, in Sotos SyndromeasclepiuspdfsNoch keine Bewertungen
- Problem Set #3Dokument3 SeitenProblem Set #3Riley SpielmanNoch keine Bewertungen
- Document on skin changes associated with hypothyroidismDokument3 SeitenDocument on skin changes associated with hypothyroidismKrystal VallesNoch keine Bewertungen
- Animal Tissue StructuresDokument12 SeitenAnimal Tissue StructuresPatricia GarciaNoch keine Bewertungen
- Human Respiratory System and MechanicsDokument105 SeitenHuman Respiratory System and MechanicsAbdul Qadir100% (1)
- Factors Affecting PCR Amplifications and The TroubleshootingDokument27 SeitenFactors Affecting PCR Amplifications and The TroubleshootingXavier LooNoch keine Bewertungen
- Biotechnology Study GuideDokument9 SeitenBiotechnology Study Guideapi-284282126Noch keine Bewertungen
- Gastrointestinal HormonesDokument46 SeitenGastrointestinal HormonesTaufiq Singgih BaskoroNoch keine Bewertungen
- Myco Viro Mod 5Dokument3 SeitenMyco Viro Mod 5Pauline Louise S. DURANNoch keine Bewertungen
- Ozone TherapyDokument24 SeitenOzone TherapyDadoBabylobas100% (2)
- Month 4 PDFDokument8 SeitenMonth 4 PDFCheryl YeanNoch keine Bewertungen
- Buteyko Meets DR MewDokument176 SeitenButeyko Meets DR MewAnonymous hndaj8zCA100% (1)
- CytogeneticsDokument9 SeitenCytogeneticsnaiktariq00Noch keine Bewertungen
- Patient Fact Sheet: SecukinumabDokument1 SeitePatient Fact Sheet: SecukinumabKarthik YadaNoch keine Bewertungen
- Genetic Basis For Variation I ANSWDokument10 SeitenGenetic Basis For Variation I ANSWwan yangNoch keine Bewertungen
- Papalia SummarydocxDokument38 SeitenPapalia Summarydocxec_ecNoch keine Bewertungen
- PH 303 Study GuideDokument44 SeitenPH 303 Study GuidesheilaNoch keine Bewertungen
- Science 6 1st RatingDokument85 SeitenScience 6 1st RatingMichael Joseph SantosNoch keine Bewertungen
- Create PDFDokument11 SeitenCreate PDFpuskesmas mantangNoch keine Bewertungen