Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Far Eastern University - Nicanor Reyes Medical FoundationDokument2 SeitenFar Eastern University - Nicanor Reyes Medical FoundationMikee MeladNoch keine Bewertungen
- 2.1musculoskeletal Radiology I IIDokument8 Seiten2.1musculoskeletal Radiology I IIMikee MeladNoch keine Bewertungen
- CD RADIO Upper and Lower ExtDokument12 SeitenCD RADIO Upper and Lower Extisprikitik3Noch keine Bewertungen
- 3.2cerebrovascular Disease 2018Dokument7 Seiten3.2cerebrovascular Disease 2018Mikee MeladNoch keine Bewertungen
- 3.1intro To Neuro Imaging 2018Dokument10 Seiten3.1intro To Neuro Imaging 2018Mikee MeladNoch keine Bewertungen
- CD RADIO Upper and Lower ExtDokument12 SeitenCD RADIO Upper and Lower Extisprikitik3Noch keine Bewertungen
- 2.2CD RADIO Upper and Lower ExtDokument15 Seiten2.2CD RADIO Upper and Lower ExtMikee MeladNoch keine Bewertungen
- Far Eastern University - Nicanor Reyes Medical FoundationDokument4 SeitenFar Eastern University - Nicanor Reyes Medical FoundationMikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.02.01 - Case - Kimberly Bergalis (Pat G)Dokument3 Seiten(Bioethics 2) 2.02.01 - Case - Kimberly Bergalis (Pat G)Asylum AllegoryNoch keine Bewertungen
- (CD B - Clin Path) Renal Function Tests - DR - AtibagosDokument3 Seiten(CD B - Clin Path) Renal Function Tests - DR - AtibagosMikee MeladNoch keine Bewertungen
- 1.1radio AbdomenDokument19 Seiten1.1radio AbdomenMikee MeladNoch keine Bewertungen
- 1 2CDLECAbdomenAusVISIONDokument3 Seiten1 2CDLECAbdomenAusVISIONMikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.02.02 - Case - Gaetan Dugas (Pat G) PDFDokument1 Seite(Bioethics 2) 2.02.02 - Case - Gaetan Dugas (Pat G) PDFMikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.02.02 - Case - Gaetan Dugas (Pat G) PDFDokument1 Seite(Bioethics 2) 2.02.02 - Case - Gaetan Dugas (Pat G) PDFMikee MeladNoch keine Bewertungen
- (Bioethics 2) 3.02 - Neri's Ethical Issues in Surgery (Pat G)Dokument1 Seite(Bioethics 2) 3.02 - Neri's Ethical Issues in Surgery (Pat G)Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.02 - Chua-Chan - S AIDS - Health Care (Pat G)Dokument7 Seiten(Bioethics 2) 2.02 - Chua-Chan - S AIDS - Health Care (Pat G)Asylum AllegoryNoch keine Bewertungen
- (Bioethics 2) 2.05.01GregoryNovakDokument2 Seiten(Bioethics 2) 2.05.01GregoryNovakMikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.03 - Chua-Chan's Ethical Issues in Pediatrics (Pat G)Dokument4 Seiten(Bioethics 2) 2.03 - Chua-Chan's Ethical Issues in Pediatrics (Pat G)Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.03 - Chua-Chan's Ethical Issues in Pediatrics (Pat G)Dokument4 Seiten(Bioethics 2) 2.03 - Chua-Chan's Ethical Issues in Pediatrics (Pat G)Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.02 - Chua-Chan - S AIDS - Health Care (Pat G)Dokument13 Seiten(Bioethics 2) 2.02 - Chua-Chan - S AIDS - Health Care (Pat G)Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.01.01 - Case - Karen Quinlan (Pat G)Dokument1 Seite(Bioethics 2) 2.01.01 - Case - Karen Quinlan (Pat G)Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.01.01 - Case - Karen Quinlan (Pat G)Dokument3 Seiten(Bioethics 2) 2.01.01 - Case - Karen Quinlan (Pat G)Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.01.01 - Case - Karen Quinlan (Pat G)Dokument1 Seite(Bioethics 2) 2.01.01 - Case - Karen Quinlan (Pat G)Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 1.4bcase of Louie BrownDokument2 Seiten(Bioethics 2) 1.4bcase of Louie BrownMikee MeladNoch keine Bewertungen
- Mediastinum 1234Dokument57 SeitenMediastinum 1234Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 2.01 - Manalo's Ethical Decision-Making in End-Of-Life Care (Pat G)Dokument3 Seiten(Bioethics 2) 2.01 - Manalo's Ethical Decision-Making in End-Of-Life Care (Pat G)Mikee MeladNoch keine Bewertungen
- (Bioethics 2) 1.04.02 - Case - Baby M (Pat G)Dokument3 Seiten(Bioethics 2) 1.04.02 - Case - Baby M (Pat G)Mikee MeladNoch keine Bewertungen
- Gastrointestinal Tract Physiology Part 2 - Dr. VilaDokument5 SeitenGastrointestinal Tract Physiology Part 2 - Dr. VilaMikee MeladNoch keine Bewertungen
- 1-4 Assessing Specs - APIDokument34 Seiten1-4 Assessing Specs - APIMikee MeladNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Lesson Tasks: Lesson Plan: Addition and Subtraction To 20Dokument2 SeitenLesson Tasks: Lesson Plan: Addition and Subtraction To 20Марина СтанојевићNoch keine Bewertungen
- Substitution Reactions - PMDokument64 SeitenSubstitution Reactions - PMprasoon jhaNoch keine Bewertungen
- An Enhanced RFID-Based Authentication Protocol Using PUF For Vehicular Cloud ComputingDokument18 SeitenAn Enhanced RFID-Based Authentication Protocol Using PUF For Vehicular Cloud Computing0dayNoch keine Bewertungen
- Functions of The Gastrointestinal Organs: Muhammad ImranDokument21 SeitenFunctions of The Gastrointestinal Organs: Muhammad ImranSalman KhanNoch keine Bewertungen
- 3.1.1 - Nirmaan Annual Report 2018 19Dokument66 Seiten3.1.1 - Nirmaan Annual Report 2018 19Nikhil GampaNoch keine Bewertungen
- The Hot Aishwarya Rai Wedding and Her Life.20130105.040216Dokument2 SeitenThe Hot Aishwarya Rai Wedding and Her Life.20130105.040216anon_501746111100% (1)
- New Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)Dokument42 SeitenNew Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)stan.isgod99Noch keine Bewertungen
- The Two Diode Bipolar Junction Transistor ModelDokument3 SeitenThe Two Diode Bipolar Junction Transistor ModelAlbertoNoch keine Bewertungen
- Quiz EditedDokument6 SeitenQuiz EditedAbigail LeronNoch keine Bewertungen
- Emulsion LectureDokument30 SeitenEmulsion LectureRay YangNoch keine Bewertungen
- P4 Science Topical Questions Term 1Dokument36 SeitenP4 Science Topical Questions Term 1Sean Liam0% (1)
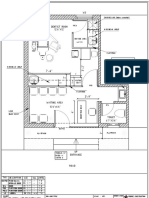
- Dental Clinic - Floor Plan R3-2Dokument1 SeiteDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- DGKCC Internship ReportDokument17 SeitenDGKCC Internship ReportMuhammad AtharNoch keine Bewertungen
- Datasheet Brahma (2023)Dokument8 SeitenDatasheet Brahma (2023)Edi ForexNoch keine Bewertungen
- Hydrotest Test FormatDokument27 SeitenHydrotest Test FormatRähûl Prätäp SïnghNoch keine Bewertungen
- Mat101 w12 Hw6 SolutionsDokument8 SeitenMat101 w12 Hw6 SolutionsKonark PatelNoch keine Bewertungen
- MVC Training Course Prerequisite: WWW - Focustech.InDokument2 SeitenMVC Training Course Prerequisite: WWW - Focustech.InLakshman Samanth ReddyNoch keine Bewertungen
- GMDSSDokument1 SeiteGMDSSRahul rajeshNoch keine Bewertungen
- E WiLES 2021 - BroucherDokument1 SeiteE WiLES 2021 - BroucherAshish HingnekarNoch keine Bewertungen
- Workshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Dokument33 SeitenWorkshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Ilie Viorel75% (4)
- Training Structure - Thinkific Plus TemplateDokument7 SeitenTraining Structure - Thinkific Plus TemplateQIONG WUNoch keine Bewertungen
- Case StarbucksDokument3 SeitenCase StarbucksAbilu Bin AkbarNoch keine Bewertungen
- JSSC JDLCCE 2021 (Civil Engineering) Official Pape 230615 233342Dokument39 SeitenJSSC JDLCCE 2021 (Civil Engineering) Official Pape 230615 233342Bhuban KumbhakarNoch keine Bewertungen
- Psyche Finals: Trans 2: Psychotic Disorder: SchizophreniaDokument4 SeitenPsyche Finals: Trans 2: Psychotic Disorder: SchizophreniajisooNoch keine Bewertungen
- Nursing Care Plan For AIDS HIVDokument3 SeitenNursing Care Plan For AIDS HIVFARAH MAE MEDINA100% (2)
- Btech CertificatesDokument6 SeitenBtech CertificatesSuresh VadlamudiNoch keine Bewertungen
- ZEROPAY WhitepaperDokument15 SeitenZEROPAY WhitepaperIlham NurrohimNoch keine Bewertungen
- The Origin, Nature, and Challenges of Area Studies in The United StatesDokument22 SeitenThe Origin, Nature, and Challenges of Area Studies in The United StatesannsaralondeNoch keine Bewertungen
- Preparation, Characterization, and Evaluation of Some Ashless Detergent-Dispersant Additives For Lubricating Engine OilDokument10 SeitenPreparation, Characterization, and Evaluation of Some Ashless Detergent-Dispersant Additives For Lubricating Engine OilNelson Enrique Bessone MadridNoch keine Bewertungen
- Speaking Quý 1 2024Dokument43 SeitenSpeaking Quý 1 2024Khang HoàngNoch keine Bewertungen