Das könnte Ihnen auch gefallen
- Pre-Employment ChecklistDokument1 SeitePre-Employment ChecklistBrielleNoch keine Bewertungen
- Pre-Employment ChecklistDokument1 SeitePre-Employment ChecklistBrielleNoch keine Bewertungen
- 7 Gastroenteritis Nursing Care Plans - NurseslabsDokument8 Seiten7 Gastroenteritis Nursing Care Plans - NurseslabsHikaru Takishima91% (23)
- Applied Protozoology and Parasitology Key ConceptsDokument60 SeitenApplied Protozoology and Parasitology Key ConceptsIL Mago50% (2)
- Roundworms: Characteristics, Types & DiseasesDokument257 SeitenRoundworms: Characteristics, Types & Diseasessummer dj100% (1)
- Introduction to Helminthology: Understanding Intestinal ParasitesDokument44 SeitenIntroduction to Helminthology: Understanding Intestinal Parasitespurnama bakti0% (1)
- Poultry diseases: Causes, symptoms and treatment, with notes on post-mortem examinationsVon EverandPoultry diseases: Causes, symptoms and treatment, with notes on post-mortem examinationsNoch keine Bewertungen
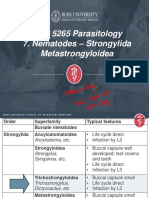
- VMP 5265 Parasitology 6. Nematodes - Strongylida ResistanceDokument54 SeitenVMP 5265 Parasitology 6. Nematodes - Strongylida ResistanceJessica KadykNoch keine Bewertungen
- ParasitologyDokument390 SeitenParasitologyVench DemicaisNoch keine Bewertungen
- Virus Family Envelope Stuff To Know Treatment/ VaccineDokument10 SeitenVirus Family Envelope Stuff To Know Treatment/ Vaccinebtoy1Noch keine Bewertungen
- 1.intro of EpidemiologyDokument30 Seiten1.intro of EpidemiologyMuhammad AsifNoch keine Bewertungen
- 5) +nematodes Fall2020 PDFDokument118 Seiten5) +nematodes Fall2020 PDFJessica KadykNoch keine Bewertungen
- 7) +nematodes Fall20 PDFDokument61 Seiten7) +nematodes Fall20 PDFJessica KadykNoch keine Bewertungen
- Cestodes of Wild Birds PDFDokument5 SeitenCestodes of Wild Birds PDFSunil100% (1)
- Nematode Infections 2019 Student PDFDokument272 SeitenNematode Infections 2019 Student PDFCharlene SuliganNoch keine Bewertungen
- Cephalosporin and Carbapenem GenerationsDokument19 SeitenCephalosporin and Carbapenem GenerationsStarlet Rhonadez Bito-onon OrielNoch keine Bewertungen
- Entamoeba histolytica (True PathogenDokument112 SeitenEntamoeba histolytica (True PathogenMiaQuiambaoNoch keine Bewertungen
- Babesia FinalDokument104 SeitenBabesia FinalSameerPeerNoch keine Bewertungen
- Trematodes of Wild BirdsDokument5 SeitenTrematodes of Wild BirdsSunilNoch keine Bewertungen
- Malarial ParasitesDokument27 SeitenMalarial ParasitesHANNAH SHALOM FERNANDEZNoch keine Bewertungen
- Standardised Nomenclature of Animal Parasitic Diseases (Snopad)Dokument67 SeitenStandardised Nomenclature of Animal Parasitic Diseases (Snopad)Pwaveno BamaiyiNoch keine Bewertungen
- Phylum NematodaDokument14 SeitenPhylum NematodaEloisa LopezNoch keine Bewertungen
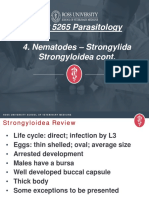
- VMP 5265 Parasitology 4. Nematodes - Strongylida Strongyloidea ContDokument40 SeitenVMP 5265 Parasitology 4. Nematodes - Strongylida Strongyloidea ContJessica KadykNoch keine Bewertungen
- Unit-I. Epidemiology IntroductionDokument60 SeitenUnit-I. Epidemiology IntroductionAny OneNoch keine Bewertungen
- Prac PracDokument16 SeitenPrac PracIdkNoch keine Bewertungen
- 3) +nematodes Su20 PDFDokument67 Seiten3) +nematodes Su20 PDFJessica KadykNoch keine Bewertungen
- Introduction To ParasitologyDokument79 SeitenIntroduction To ParasitologyLeeShauran100% (7)
- Quinolones, Folic Acid Antagonist and Urinary Tract Antitb and LeprosyDokument124 SeitenQuinolones, Folic Acid Antagonist and Urinary Tract Antitb and LeprosyrenNoch keine Bewertungen
- NemaoDokument94 SeitenNemaoRoxenette Gil Bernales PangilinanNoch keine Bewertungen
- Phylum Platyhelminthes (Flatworms) : Important InformationDokument26 SeitenPhylum Platyhelminthes (Flatworms) : Important InformationYoussef EmadNoch keine Bewertungen
- Bacteria PDFDokument13 SeitenBacteria PDFJohn Christopher LucesNoch keine Bewertungen
- Emetics and Antiemetics 2012 PDFDokument36 SeitenEmetics and Antiemetics 2012 PDFJamaluddin Ahmad A.M100% (2)
- Introduction To MycologyDokument66 SeitenIntroduction To MycologyHerlinaNababanNoch keine Bewertungen
- ANTIMICROBIAL ResistanceDokument4 SeitenANTIMICROBIAL ResistancePuspa Das100% (1)
- Medical Parasitology - FullDokument30 SeitenMedical Parasitology - FullJesse Osborn100% (2)
- MycologyDokument9 SeitenMycologyibti100% (1)
- Levanthan Short Ans KeyDokument42 SeitenLevanthan Short Ans Keyxyab.varga.swuNoch keine Bewertungen
- Chapter 13 PharmacologyDokument35 SeitenChapter 13 PharmacologyEdelrose LapitanNoch keine Bewertungen
- Trematodes LECDokument2 SeitenTrematodes LECAki SuzumeNoch keine Bewertungen
- CephalosporinsDokument21 SeitenCephalosporinsMoha Bin Ladiif75% (4)
- Leishmania NewDokument27 SeitenLeishmania NewAnnu RajeshNoch keine Bewertungen
- Pregnancy Pathology: Causes and Types of AbortionDokument73 SeitenPregnancy Pathology: Causes and Types of AbortionRafiq Samto100% (1)
- Blood Tissue and FlagellatesDokument15 SeitenBlood Tissue and FlagellatesHughNoch keine Bewertungen
- Microbiology textbook and reference guide comparisonDokument2 SeitenMicrobiology textbook and reference guide comparisonIbrahimFikryNoch keine Bewertungen
- Postpartum Uterine Infection in CattleDokument26 SeitenPostpartum Uterine Infection in CattleDilip GuptaNoch keine Bewertungen
- Innate ImmunityDokument9 SeitenInnate Immunitynascha dumpNoch keine Bewertungen
- Veterinary Clinical Pathology Clerkship ProgramDokument46 SeitenVeterinary Clinical Pathology Clerkship ProgramDrVijayata ChoudharyNoch keine Bewertungen
- Actinomycosis: Mohanad N. Saleh 6 Year Meical Student Supervisor: Dr. Anas MuhannaDokument19 SeitenActinomycosis: Mohanad N. Saleh 6 Year Meical Student Supervisor: Dr. Anas MuhannaMohanad SalehNoch keine Bewertungen
- M T Ch16 Innate Immunity SDokument30 SeitenM T Ch16 Innate Immunity SAnonymous STRYVGKNoch keine Bewertungen
- pm2 TREMATODESDokument39 Seitenpm2 TREMATODESshastaNoch keine Bewertungen
- Maraviroc: A New Approach Against The HumanDokument4 SeitenMaraviroc: A New Approach Against The HumanAimhigh_PPMNoch keine Bewertungen
- Communicable Disease of The Gastro Intestinal TractDokument40 SeitenCommunicable Disease of The Gastro Intestinal Tractɹǝʍdןnos100% (2)
- Cytologic Patterns - Eclinpath PDFDokument5 SeitenCytologic Patterns - Eclinpath PDFJD46Noch keine Bewertungen
- Parasites of PoultryDokument8 SeitenParasites of PoultrylisaNoch keine Bewertungen
- Pharmacology Module PDFDokument23 SeitenPharmacology Module PDFmirza_baig_46100% (1)
- Trypanosoma: Sri SundariDokument37 SeitenTrypanosoma: Sri SundariVaniaNoch keine Bewertungen
- Common Poultry DiseasesDokument15 SeitenCommon Poultry DiseasesMamas IpunkNoch keine Bewertungen
- Microbiology Slides MediaDokument34 SeitenMicrobiology Slides MediaTarek ElnagdyNoch keine Bewertungen
- Pathogenesis, Treatment and Prevention of LeishmaniasisVon EverandPathogenesis, Treatment and Prevention of LeishmaniasisMukesh SamantNoch keine Bewertungen
- Pathology, Vector Studies, and CultureVon EverandPathology, Vector Studies, and CultureJulius P. KreierBewertung: 5 von 5 Sternen5/5 (1)
- Malaria: Immunology and ImmunizationVon EverandMalaria: Immunology and ImmunizationJulius P. KreierNoch keine Bewertungen
- Ra 5527Dokument10 SeitenRa 5527wendeliciousNoch keine Bewertungen
- Document 1Dokument1 SeiteDocument 1BrielleNoch keine Bewertungen
- BimbDokument2 SeitenBimbCattrainuhNoch keine Bewertungen
- BB RiveraDokument3 SeitenBB RiveraBrielleNoch keine Bewertungen
- Research questions on blood typing procedures and hemolytic disease of the newborn (HDNDokument3 SeitenResearch questions on blood typing procedures and hemolytic disease of the newborn (HDNBrielleNoch keine Bewertungen
- Chapt Er9:BloodvesselsDokument20 SeitenChapt Er9:BloodvesselsBrielleNoch keine Bewertungen
- Addisons Disease and HypercorticolismDokument2 SeitenAddisons Disease and HypercorticolismBrielleNoch keine Bewertungen
- 1 SheyDokument1 Seite1 SheyBrielleNoch keine Bewertungen
- Hematology CourseDokument89 SeitenHematology CourseSuzie Q BeatrixNoch keine Bewertungen
- Blood Bank Equipment FunctionsDokument14 SeitenBlood Bank Equipment FunctionsBrielleNoch keine Bewertungen
- Cal A ChuchiDokument1 SeiteCal A ChuchiBrielleNoch keine Bewertungen
- LeprosyDokument11 SeitenLeprosyBrielleNoch keine Bewertungen
- Epidemiology of Toxic and Infectious Risk Related To Shellfish ConsumptionDokument1 SeiteEpidemiology of Toxic and Infectious Risk Related To Shellfish ConsumptionBrielleNoch keine Bewertungen
- Epidemiology of Toxic and Infectious Risk Related To Shellfish ConsumptionDokument1 SeiteEpidemiology of Toxic and Infectious Risk Related To Shellfish ConsumptionBrielleNoch keine Bewertungen
- 3021 Reflective JournalDokument5 Seiten3021 Reflective Journalapi-660581645Noch keine Bewertungen
- Diabetes Ada 2020 PDFDokument10 SeitenDiabetes Ada 2020 PDFOrlando CuellarNoch keine Bewertungen
- Fat Embolism Syndrome: DescriptionDokument4 SeitenFat Embolism Syndrome: DescriptionDayuKurnia DewantiNoch keine Bewertungen
- Preeclampsia SFlt-1-PlGF Ratio - Pocket CardDokument2 SeitenPreeclampsia SFlt-1-PlGF Ratio - Pocket CardRajeev PareekNoch keine Bewertungen
- Substance Abuse & PregnancyDokument2 SeitenSubstance Abuse & PregnancyChelcee MagsinoNoch keine Bewertungen
- Multi Lab Id ReportDokument12 SeitenMulti Lab Id ReportMayuresh NaikNoch keine Bewertungen
- 21841Dokument397 Seiten21841Sudheer JayaramNoch keine Bewertungen
- Chapter 2 Respiratory AssessmentDokument9 SeitenChapter 2 Respiratory AssessmentKathleen Dela CruzNoch keine Bewertungen
- SKIN, HAIR, and NAILSDokument17 SeitenSKIN, HAIR, and NAILSkhalidNoch keine Bewertungen
- Patient-Nurse DialogueDokument3 SeitenPatient-Nurse Dialogueristy dian puspitaNoch keine Bewertungen
- Peach and Green Organic Shapes Meditation Workshop Webinar Keynote PresentationDokument7 SeitenPeach and Green Organic Shapes Meditation Workshop Webinar Keynote PresentationNicole Ivy GorimoNoch keine Bewertungen
- RupatadineDokument1 SeiteRupatadinePiscean YangNoch keine Bewertungen
- Transfusion - March April 1966 - Allen - Choice of Blood For Exchange TransfusionDokument3 SeitenTransfusion - March April 1966 - Allen - Choice of Blood For Exchange TransfusionDR. KHANNoch keine Bewertungen
- Dr. Tyna MooreDokument91 SeitenDr. Tyna MooreCaroline AloulNoch keine Bewertungen
- COPD AE (Book) (20210118) (林冠霖)Dokument15 SeitenCOPD AE (Book) (20210118) (林冠霖)林冠霖Noch keine Bewertungen
- Evo ProductDokument58 SeitenEvo ProductMohammadfaroq HasanNoch keine Bewertungen
- Torticolis OdtDokument25 SeitenTorticolis OdtAndreea CimpoiNoch keine Bewertungen
- American J Hematol - 2022 - Ansell - Hodgkin Lymphoma 2023 Update On Diagnosis Risk Stratification and ManagementDokument12 SeitenAmerican J Hematol - 2022 - Ansell - Hodgkin Lymphoma 2023 Update On Diagnosis Risk Stratification and ManagementRaul Matute MartinNoch keine Bewertungen
- Coronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdDokument99 SeitenCoronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdMwanja MosesNoch keine Bewertungen
- Comprehensive Geriatric AssessmentDokument75 SeitenComprehensive Geriatric AssessmentBodat BodatsNoch keine Bewertungen
- Tog 12091Dokument4 SeitenTog 12091princessmeleana6499Noch keine Bewertungen
- Case Study-Infant With Fluid Imbalance08-10-KEYDokument3 SeitenCase Study-Infant With Fluid Imbalance08-10-KEYreecoleNoch keine Bewertungen
- Questions After Dr. Hamoud FileDokument9 SeitenQuestions After Dr. Hamoud File181120183Noch keine Bewertungen
- FM Shelf Exam ReviewDokument5 SeitenFM Shelf Exam ReviewMohammad Katato100% (1)
- Tatalaksana Stroke VertebrobasilarDokument20 SeitenTatalaksana Stroke VertebrobasilarMarest AskynaNoch keine Bewertungen
- Guillain-Barré SyndromeDokument60 SeitenGuillain-Barré SyndromekharaNoch keine Bewertungen
- Is Chronic Constipation A Sign of A Larger Health Issue - Dr. Samrat JankarDokument2 SeitenIs Chronic Constipation A Sign of A Larger Health Issue - Dr. Samrat JankarDr. Samrat JankarNoch keine Bewertungen
- Disorders of Lashes: Trichiasis, Metaplastic Lashes, DistichiasisDokument8 SeitenDisorders of Lashes: Trichiasis, Metaplastic Lashes, DistichiasisAhmed YounisNoch keine Bewertungen
- Acute CholecystitisDokument28 SeitenAcute CholecystitisWilfredo Mata JrNoch keine Bewertungen