Das könnte Ihnen auch gefallen
- Hemophilia and Hemostasis: A Case-Based Approach to ManagementVon EverandHemophilia and Hemostasis: A Case-Based Approach to ManagementAlice D. MaNoch keine Bewertungen
- HypoparathyroidismDokument50 SeitenHypoparathyroidismspinosumNoch keine Bewertungen
- Respiratory Distress Syndrome-Hyaline Membrane DiseaseDokument4 SeitenRespiratory Distress Syndrome-Hyaline Membrane DiseaseAnapaolaNoch keine Bewertungen
- Acute Lymphocytic LeukaemiaDokument100 SeitenAcute Lymphocytic LeukaemiaHan KethyanethNoch keine Bewertungen
- Blood TransfusionDokument7 SeitenBlood TransfusionSamantha Orozco PinedaNoch keine Bewertungen
- Ijpo 5 (1) 6-11Dokument6 SeitenIjpo 5 (1) 6-11Rajesh SahuNoch keine Bewertungen
- Cancer in Children and Young People: Acute Nursing CareVon EverandCancer in Children and Young People: Acute Nursing CareNoch keine Bewertungen
- The Thalassemias: December 2014Dokument7 SeitenThe Thalassemias: December 2014Joscelind SunaryoNoch keine Bewertungen
- Sindrom NefroticDokument7 SeitenSindrom NefroticHilion FLAVIONoch keine Bewertungen
- Tirotoxicosis Mayo Clinic Proceedings. Harma2019Dokument17 SeitenTirotoxicosis Mayo Clinic Proceedings. Harma2019Salome GarciaNoch keine Bewertungen
- 2021 HiperkaliemiaDokument8 Seiten2021 HiperkaliemiaAlexis Luna BurgueñoNoch keine Bewertungen
- Hiperkalemia en ERDokument8 SeitenHiperkalemia en ERmjbb1310Noch keine Bewertungen
- Hyperkalemia Management in The Emergency Department: An Expert Panel ConsensusDokument8 SeitenHyperkalemia Management in The Emergency Department: An Expert Panel ConsensusDaniel HeSaNoch keine Bewertungen
- Veterinary Clinical Pathol - 2023 - Dohány - A Retrospective Evaluation of Phenobarbital Induced Hematologic Changes in 69Dokument6 SeitenVeterinary Clinical Pathol - 2023 - Dohány - A Retrospective Evaluation of Phenobarbital Induced Hematologic Changes in 69Lorena TomoiagăNoch keine Bewertungen
- A Retrospective Evaluation of Phenobarbital-Induced Hematologic Changes in 69 CatsDokument6 SeitenA Retrospective Evaluation of Phenobarbital-Induced Hematologic Changes in 69 CatsAkın SeverNoch keine Bewertungen
- Hemofilia Es enDokument5 SeitenHemofilia Es enChristiadi karlin12Noch keine Bewertungen
- Shunkwiler Et Al-2017-Journal of Clinical ApheresisDokument10 SeitenShunkwiler Et Al-2017-Journal of Clinical ApheresisVenkata Sreekanth SampathNoch keine Bewertungen
- Perioperative Management of Acquired Hemophilia A: A Case Report and Review of LiteratureDokument3 SeitenPerioperative Management of Acquired Hemophilia A: A Case Report and Review of LiteratureSiva SankarNoch keine Bewertungen
- Diagnosis and Management of Hyponatremia A ReviewDokument12 SeitenDiagnosis and Management of Hyponatremia A ReviewCynthia Huaman C.Noch keine Bewertungen
- Epidemiology and Complications of HypoparathyroidismDokument12 SeitenEpidemiology and Complications of HypoparathyroidismErika AvilaNoch keine Bewertungen
- Tumor MicroenvironmentVon EverandTumor MicroenvironmentDietmar W. SiemannNoch keine Bewertungen
- AssignmentDokument11 SeitenAssignmentrehamoh1997Noch keine Bewertungen
- Toxins 12 00269Dokument11 SeitenToxins 12 00269Dana DumitruNoch keine Bewertungen
- Wet Beriberi With Multiple Organ Failure Remarkably Reversed by Thiamine Administration - A Case Report and Literature ReviewDokument5 SeitenWet Beriberi With Multiple Organ Failure Remarkably Reversed by Thiamine Administration - A Case Report and Literature Reviewgwyneth.green.512Noch keine Bewertungen
- (1479683X - European Journal of Endocrinology) MANAGEMENT of ENDOCRINE DISEASE - Pathogenesis and Management of HypoglycemiaDokument11 Seiten(1479683X - European Journal of Endocrinology) MANAGEMENT of ENDOCRINE DISEASE - Pathogenesis and Management of HypoglycemiaNair Salas VelardeNoch keine Bewertungen
- Case HipotiroidDokument3 SeitenCase HipotiroidVivi DeviyanaNoch keine Bewertungen
- Jurnal 6Dokument21 SeitenJurnal 6onisNoch keine Bewertungen
- Epidemiological Profile and Treatment Pattern of Vitiligo in A Tertiary Care Teaching HospitalDokument5 SeitenEpidemiological Profile and Treatment Pattern of Vitiligo in A Tertiary Care Teaching HospitalVidini Kusuma AjiNoch keine Bewertungen
- ANGIOEDEMADokument11 SeitenANGIOEDEMAromimedNoch keine Bewertungen
- Fast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseVon EverandFast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseNoch keine Bewertungen
- Acquired Hemophilia A Presenting in An Elderly Man: Teaching Case ReportDokument2 SeitenAcquired Hemophilia A Presenting in An Elderly Man: Teaching Case ReportvishnupgiNoch keine Bewertungen
- Practical Lipid Management: Concepts and ControversiesVon EverandPractical Lipid Management: Concepts and ControversiesNoch keine Bewertungen
- Anemia in Cancer Some Pathophysiological AspectsDokument6 SeitenAnemia in Cancer Some Pathophysiological AspectsCindyGaniNoch keine Bewertungen
- HaematologyDokument260 SeitenHaematologydatitox100% (1)
- The Qualitative Estimation of BCR-ABL Transcript: An In-Lab Procedural Study on Leukemia PatientsVon EverandThe Qualitative Estimation of BCR-ABL Transcript: An In-Lab Procedural Study on Leukemia PatientsNoch keine Bewertungen
- Thyroiditis: Evaluation and TreatmentDokument9 SeitenThyroiditis: Evaluation and Treatmentรติรัตน์ หนูนุ่นNoch keine Bewertungen
- Primary HyperparathyroidismDokument50 SeitenPrimary HyperparathyroidismKate ClarksonNoch keine Bewertungen
- Sca PDFDokument58 SeitenSca PDFMUHAMMAD09Noch keine Bewertungen
- Nejmct 1007101Dokument9 SeitenNejmct 1007101Daniel LamNoch keine Bewertungen
- Casos Medicina InternaDokument219 SeitenCasos Medicina Internazara galiciaNoch keine Bewertungen
- A Study Assess The Knowledge Regarding of Hemophilia Among Female Students in Jazan UniversityDokument14 SeitenA Study Assess The Knowledge Regarding of Hemophilia Among Female Students in Jazan Universityشهد خالدNoch keine Bewertungen
- Enf de Graves NEJM 2008Dokument12 SeitenEnf de Graves NEJM 2008david santiago libreros pinedaNoch keine Bewertungen
- Blood Trasnfusions 1Dokument7 SeitenBlood Trasnfusions 1Silvia RodríguezNoch keine Bewertungen
- Marfan'sDokument39 SeitenMarfan'sRavin DebieNoch keine Bewertungen
- Lisis TumoralDokument11 SeitenLisis TumoralCsr A. Varela UlloaNoch keine Bewertungen
- Challenging Therapy in Pregnant Woman With Systemic Lupus Erythematosus (SLE) and Chronic Hepatitis BDokument3 SeitenChallenging Therapy in Pregnant Woman With Systemic Lupus Erythematosus (SLE) and Chronic Hepatitis BMiss AmyNoch keine Bewertungen
- Myelodysplastic Syndromes PDFDokument14 SeitenMyelodysplastic Syndromes PDFAdriian PortilloNoch keine Bewertungen
- Preventiondiagnosis of Hbpathies BOOKLETNEW 1Dokument82 SeitenPreventiondiagnosis of Hbpathies BOOKLETNEW 1amaya rajivNoch keine Bewertungen
- Hemophila 190121092014Dokument46 SeitenHemophila 190121092014interna MANADONoch keine Bewertungen
- Bleeding 20 ProblemDokument7 SeitenBleeding 20 ProblemDalilah DahalanNoch keine Bewertungen
- Seminar: Lionel Adès, Raphael Itzykson, Pierre FenauxDokument14 SeitenSeminar: Lionel Adès, Raphael Itzykson, Pierre FenauxAchmad Teguh Fikri PratamaNoch keine Bewertungen
- Arterial Disorders: Definition, Clinical Manifestations, Mechanisms and Therapeutic ApproachesVon EverandArterial Disorders: Definition, Clinical Manifestations, Mechanisms and Therapeutic ApproachesAdel BerbariNoch keine Bewertungen
- Haemolytic Uremic Syndrome: Diagnosis and Management (Version 1 Peer Review: 3 Approved)Dokument11 SeitenHaemolytic Uremic Syndrome: Diagnosis and Management (Version 1 Peer Review: 3 Approved)Ana-Mihaela BalanuțaNoch keine Bewertungen
- J Transci 2018 10 013Dokument7 SeitenJ Transci 2018 10 013Clara Espinosa ArnandisNoch keine Bewertungen
- Thiamine Deficiency Disease, Dysautonomia, and High Calorie MalnutritionVon EverandThiamine Deficiency Disease, Dysautonomia, and High Calorie MalnutritionBewertung: 4.5 von 5 Sternen4.5/5 (5)
- Hemorrhoids in PregnancyDokument3 SeitenHemorrhoids in PregnancySalwa Rizky SalsabillaNoch keine Bewertungen
- HematologyDokument58 SeitenHematologyAchmad DainuriNoch keine Bewertungen
- A Model for Gene Therapy: Gene Replacement in the Treatment of Sickle Cell Anemia and ThalassemiaVon EverandA Model for Gene Therapy: Gene Replacement in the Treatment of Sickle Cell Anemia and ThalassemiaNoch keine Bewertungen
- Soal Ulangan Harian Sistem Sirkulasi (Tanggapan)Dokument65 SeitenSoal Ulangan Harian Sistem Sirkulasi (Tanggapan)Dortje Pili RoboNoch keine Bewertungen
- Lecture 16 - Bleeding Tendency DiseasesDokument64 SeitenLecture 16 - Bleeding Tendency Diseasesapi-3703352100% (1)
- Pathology Outlines - Abnormal PT and PTT - CausesDokument1 SeitePathology Outlines - Abnormal PT and PTT - CausesShane AranetaNoch keine Bewertungen
- Coagulation Capillary: BloodDokument5 SeitenCoagulation Capillary: BloodSafiyanu IbrahimNoch keine Bewertungen
- Abordaje Niño Que Sangra Hematologia de OskyDokument13 SeitenAbordaje Niño Que Sangra Hematologia de OskyivanNoch keine Bewertungen
- Haemophilia AssignmentDokument2 SeitenHaemophilia AssignmentKhadija JaraNoch keine Bewertungen
- HemostasisDokument23 SeitenHemostasisSwathi BNoch keine Bewertungen
- Hemostasis Catalog Rev.14 - Eu 2017 PDFDokument56 SeitenHemostasis Catalog Rev.14 - Eu 2017 PDFIulia MariaNoch keine Bewertungen
- Blood RevisedDokument105 SeitenBlood RevisedKanelle SisayanNoch keine Bewertungen
- Heparin Resistance - Clinical Perspectives and Management StrategiesDokument7 SeitenHeparin Resistance - Clinical Perspectives and Management StrategiesRaul DoctoNoch keine Bewertungen
- Bleeding Time & Clotting Time Practical NewDokument34 SeitenBleeding Time & Clotting Time Practical NewSreedeep Teja100% (1)
- Secondary HemostasisDokument9 SeitenSecondary HemostasisMedicah Simon PeligrinoNoch keine Bewertungen
- Coadata 504+: Incl. Dual-Wavelength TechnologyDokument4 SeitenCoadata 504+: Incl. Dual-Wavelength TechnologyAgung PutraNoch keine Bewertungen
- PT, Aptt, TTDokument44 SeitenPT, Aptt, TTswaraj sharmaNoch keine Bewertungen
- BT CT PT PTTDokument31 SeitenBT CT PT PTTCristineVillablancaNoch keine Bewertungen
- Protrombin TimeDokument2 SeitenProtrombin TimeMark Norriel CajandabNoch keine Bewertungen
- 1 s2.0 S0140673603134058 MainDokument9 Seiten1 s2.0 S0140673603134058 MainΚωνσταντίνος ΤσίπηςNoch keine Bewertungen
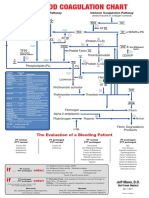
- Blood Clotting ChartDokument1 SeiteBlood Clotting ChartBianca SimionescuNoch keine Bewertungen
- Guyton Chapter 36Dokument6 SeitenGuyton Chapter 36g_komolafe100% (1)
- Lesson 8Dokument11 SeitenLesson 8Jill ArciagaNoch keine Bewertungen
- Pathophysiology of Protein S DeficiencyDokument5 SeitenPathophysiology of Protein S DeficiencyRenz Ivan FuntilonNoch keine Bewertungen
- Blood Coagulation 2011Dokument64 SeitenBlood Coagulation 2011azizNoch keine Bewertungen
- Coagulants and AnticoagulantsDokument5 SeitenCoagulants and AnticoagulantsMuhammad AsifNoch keine Bewertungen
- Jawaban DK Herwandi - Pemicu 1 - Modul Hematologi Dan Onkologi - 2018Dokument5 SeitenJawaban DK Herwandi - Pemicu 1 - Modul Hematologi Dan Onkologi - 2018HerwandiNoch keine Bewertungen
- HemophiliaDokument19 SeitenHemophiliaHatem EletrebyNoch keine Bewertungen
- Prothrombin Time (PT) PDFDokument3 SeitenProthrombin Time (PT) PDFbongbongz8646100% (2)
- Platelet Von Willebrand Factor in Hermansky-Pudlak Syndrome (American Journal of Hematology, Vol. 59, Issue 2) (1998)Dokument6 SeitenPlatelet Von Willebrand Factor in Hermansky-Pudlak Syndrome (American Journal of Hematology, Vol. 59, Issue 2) (1998)Ahmed MagzoubNoch keine Bewertungen
- HemofiliaDokument17 SeitenHemofiliareinyNoch keine Bewertungen
- Antiphospholipid Syndrome: Antiphospholipid Syndrome or Antiphospholipid Antibody Syndrome (APS orDokument6 SeitenAntiphospholipid Syndrome: Antiphospholipid Syndrome or Antiphospholipid Antibody Syndrome (APS orhikmat sheraniNoch keine Bewertungen
- Blood GroupDokument13 SeitenBlood GroupShanJishmaNoch keine Bewertungen