Beruflich Dokumente
Kultur Dokumente
Cva Other Diseases
Hochgeladen von
sheila roma sibugCopyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Cva Other Diseases
Hochgeladen von
sheila roma sibugCopyright:
Verfügbare Formate
lOMoARcPSD|3537447
CVA & Other diseases
Physical therapy (Our Lady of Fatima University)
StuDocu is not sponsored or endorsed by any college or university
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
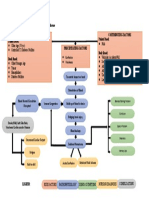
CVA
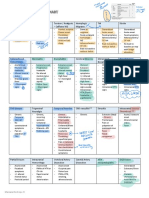
Differentials: Disconnection syndromes
Epidemiology Split brain
Old > young, M > F, black > white, asian > US Disconnection apraxia/(L) side apraxia
Alexia w/o agraphia/Pure word blindness
Pathophysiology Pure word deafness
Focal infarction and ischemic penumbra Conduction aphasia
Cerebral edema → ↑ ICP → herniation
S/Sx: ↓ level of consciousness, widened pulse pressure, ↑ HR, PCA
Cheyne-Stokes respiration, vomiting, unreacting pupils, Behavioral disorders
papilloedema Akinetic mutism
Abulia
Risk Factors Pseudobulbar affect/emotional dysregulation syndrome
Modifiable (L) (R)
Hypertension cautious impulsive
DM Visual impairment
Heart disease Visual agnosia
Cigarette smoking Pure word blindness
Hypercholesterolemia Anton – denial of blindness
Obesity (L) (R)
TIA simultagnosia depth & distance
Asymptomatic carotid bruit color agnosia
↑ hematocrit/serum fibrinogen prosopagnosia
Non-modifiable Memory deficit
Race Hemisensory deficit
Age *Thalamic pain/Dejerine-Roussy syndrome
Sex
Previous stroke Lacunar
Pure motor
Classification: Temporal Pure sensory
TIA Dysarthria with facial weakness
Reversible ischemic neurologic deficit Dysarthria with clumsy hand
Stroke in evolution Ataxic hemiparesis
Completed stroke
Brainstem
Classification: Pathophysiological
Ischemic Syndrome Area Ipsi Contra
- Thrombotic(40%) Weber medial CN III hemiplegia
- Embolic (20%) basal
- Lacunar(20%) midbrain
- Other (5%) Benedikt tegmetum CN III pain & T°,
Hemorrhagic of midbrain ataxia
- Intracerebral (10%) proprioception,
- Subarachnoid (5%) tremor, chorea,
Locked-In bilateral (+) upward
Classification: Neuroanatomical basal pons gaze only
ICA Millard- lateral pons CN VI, VII hemiplegia
Gubler
MCA Wallenberg lateral CN X & V, pain pain & T°
Contralateral hemiplegia (PICA/Latera medulla & T° (face), (body)
Contralateral hemianesthesia l Medullary ataxia,
Frontal gaze palsy Syndrome) Horner’s
Aphasias nystagmus
(L) (R) AICA cerebellum, CN V, VI, VII, pain & T°
44 Broca Aprosodia brainstem pain & T° (body)
Amelodosia (face), ataxia,
22 Wernicke Affective agnosia Horner’s
Amusia SCA cerebellum, ataxia, pain & T°
Apraxia brainstem Horner’s (body & face)
(L) (R)
39 Gerstmann Examination
40 Ideomotor Anosognosia, Neglect Test & measures – Urinalysis, blood analysis, FBS, thyroid
P Autopagnosia
function test, full cardiac eval, lumbar puncture
Somatoagnosia Figure-ground
Imaging – CT scan, MRI, PET, Doppler, Cerebral angiopgraphy
Ideational Form
Spatial relations Medical Mx
Position in space
Meds: thrombolytics, anticoagulants, antiplatelet,
Topographic
antihypertensive
Vertical Surgery:
Constructional apraxia Endarectomy
Dressing apraxia Aneurysm repair/resection – operative (clipping, trapping,
Contralateral hemianopsia
proximal occlusion), endovascular (coil embolisation, balloon
Dysphagia
remodeling, balloon occlusion, stents)
Evacuation of hematoma
ACA
Contralateral hemiplegia
Others
Contralateral hemianesthesia
Disability Scale – Fugl Meyer, STREAM
Uninhibited neurogenic bladder Greatest recovery – 3-6 months
Primitive reflexes
Palmomental
Predictors
Pout
1 month recovery → 6 month recovery
Grasp/Groping Grip strength at 24 hrs → arm recovery in 3 months
*Gegenhalten/Paratonia Poor Predictors
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
coma at onset persistent incontinence • Contralateral hemisensory loss involving mainly the UE
poor cognitive function severe hemiplegia and face (LE is more spared)
prior stroke visual-spatial perceptual deficit • Motor speech impairment: Broca’s or nonfluent aphasia
unilateral hemineglect significant cardiovascular disease with limited vocabulary and slow, hesitant speech
large cerebral lesion multiple neurologic deficits • Receptive speech impairment: Wernicke’s or fluent
lack of return of motor function after 1 month aphasia with impaired auditory comprehension and
fluent speech with normal rate and melody
STROKE • Global aphasia: nonfluent speech with poor
• Stroke is the sudden occurrence of permanent damage to comprehension
an area of the brain caused by a blocked blood vessel • Perceptual deficits: unilateral neglect, depth perception,
or bleeding within the brain. spatial relations, agnosia
• TWO MAJOR CATEGORIES: • Limb-kinetic apraxia
➢ Ischemic Note:
➢ Hemorrhagic PERCEPTUAL – UN – failure to respond to people or objects
Note: presented to the side opposite a brain lesion.
Strokes can be divided into two major categories: Ischemic – Depth perception- ability to determine distances between objects
most common type of stroke and see the world in three dimensions
- affects about 80% of individuals with stroke Apraxia- difficulty in motor planning
- happens when a clot blocks or impairs blood flow, depriving Difficulty making precise movements with
the brain of essential
oxygen and nutrients. • Contralateral homonymous hemianopsia
• etiology • Loss of conjugate gaze to the opposite side
• Atherosclerosis • Ataxia of contralateral limb(s) (sensory ataxia)
• Ischemic Strokes • Pure motor hemiplegia (lacunar stroke)
➢ Cerebral Thrombosis Note:
➢ Cerebral embolus (CE) Strokelike symptoms Other causes of focal brain damage, such
• Hemorrhagic Strokes as traumatic injury to the brain, demyelinating lesions (attacks the
➢ Cerebral Hemorrhage myelin sheath or the cells that produce and maintain it)
➢ Lacunar Stroke Brain tumors AB(N) Cells, brain abscesses (Inflammation and
➢ Subarachnoid Hemorrhage collection of infected material)
➢ epidemiology Homonymous hemianopsia - A homonymous hemianopia is the
• In the Philippines.. loss of part of the field of view on the same side, in both eyes.
Stroke has a prevalence of 0-9% - easily become lost, feel disoriented and unable to navigate
➢ Ischemic stroke 70% safely through the crowd
➢ Hemorrhagic stroke 30% Conjugate - ability to move both eyes in the same direction
• In the US…
➢ 795,000 individuals each year
➢ 610,000 are first attacks Medical treatment
➢ 185,000 are recurrent strokes of stroke
Note: By: Erica D. Cabusas
Women have a lower age-adjusted stroke incidence than men. ❑ Merci Retriever System
However, this is reversed in older ages; women over 85 years of ❑ Penumbra System
age have an elevated risk compared to men. Medical intervention
• Brief background thrombolytics
Modifiable Risk Factors Alteplase (tPA)
❑ Hypertension ❖
0.9 mg/kg (max 90 mg)
❑ Heart disease ❖
to be used <3 hrs. of onset
Ischemic/hypertensive symptoms for maximum
Valvular efficacy
Arrhythmias ❖ converts plasminogen to
❑ Smoking plasmin, degrades fibrin
❑ Diabetes mellitus present in clots, dissolves
❑ Elevated fibrinogen clots and reestablishes blood
❑ Erythrocytosis flow.
❑ Hyperlipidemia Possible adverse effects: The most common complication is
• Types of Strokes bleeding and brain hemorrhage.
1. Transient Ischemic Attacks
• Transient ischemic attacks (TIAs) have historically been anticoagulants
defined as a strokelike event that completely resolves Warfarin (Coumadin), Heparin
within 24 hours. The symptoms of a TIA begin -Used to reduce the risk of blood clots and prevent existing clots
abruptly and may persist for only a few seconds or from getting bigger by thinning the blood.
minutes, followed by apparent full resolution. TIAs
are not trivial events and require a thorough Possible adverse effects: Increased risk of bleeding and
investigation. Those TIAs associated with MRI evidence hemorrhage, hematomas.
of tissue damage carry a particularly high risk of further Antiplatelet therapy
vascular events. Acetylsalicylic acid (Aspirin), Clopidogrel bisulfate (Plavix),
• Signs and symptoms Dabigatran etexilate (Pradaxa), ticlopidine hydrochloride
• Aphasia (Ticlid)
• Ataxia -act by inhibiting platelet aggregation and adhesion.
• Apraxia -Prevent platelets (blood cells) from sticking together; long-term,
• Agnosia low-dose is used to decrease the risk of thrombosis and recurrent
• Anopsia stroke; higher doses may be used in place of anticoagulants
Note: Possible adverse effects: Increased risk of gastric ulcers and
Aphasia, an inability to produce and/or comprehend language bleeding.
ATAXIA the loss of coordination of muscles
Agnosia is the loss of the ability to recognize objects, faces, Antihypertensive agents
voices, or places ACE inhibitors, Alpha-blockers (Minipress), beta-blockers,
Anopsia - defect in the visual field calcium channel blockers, direct vasodilators, diuretics,
postganglionic neuron inhibitors
• Contralateral hemiparesis involving mainly the UE and -Used to control hypertension.
face (LE is more spared) Possible adverse effects: Dizziness, hypotension, among other
symptoms.
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
❑ Architectural modifications, assistive devices or orthotics
Angiotensin ii receptor antagonists should be ready before discharge
Telmisartan (Micardis), Losartan Potassium (Cozaar)
-A chemical that triggers muscle contraction around blood
vessels, narrowing them; enlarges blood vessels and reduces
blood pressure.
Possible adverse effects: Dizziness, hypotension, among other • MEDICAL DIAGNOSIS
symptoms. • ECHOCARDIOGRAM
• Uses soundwaves to produce images of the heart
Anticholesterol agents • Commonly used to allow the doctor to see if the heart is
Atorvastatin calcium or Lipitor, rosuvastatin calcium or normally beating and pumping blood
Crestor, Zocor, Mevacor, Lescol • non-invasive
-Lower cholesterol by inhibiting the enzyme in the blood that note:
produces cholesterol in the liver; for management of Use in stroke: can help determine if there is a blood clot na
hypercholesterolemia and mixed dyslipidemias. pwedeng magtravel and magcause ng stroke
Possible adverse effects: Dizziness, headache, insomnia,
weakness. • Computed Tomography (CT)
• Show areas of abnormalities in the brain, and can help to
Antispasmodic/spasmolytics determine if these areas have insufficient blood flow,
Carisoprodol (soma), chlorzoaxazone (Parafon Forte), hemorrhage, or other problems.
Cyclobenzaprine (Flexeril), Diazepam (Valiu), • Less costly than MRI
Methocarbamol (Robaxin), Orphenadrine (Norflex) Note:
-Used to relax skeletal muscle and decrease muscle spasm. A type of x-ray that uses a computer to make cross-sectional
Possible adverse effects: drowsiness, dizziness, dry mouth, images of your body
among other symptoms. Can be sagittal, coronal, etc
antispastics • a. Computed Tomography Angiogram (CTA)
Baclofen (Lioresal), Dantrolene Sodium (Dantrium), • CT scan with an involvement of a contrast media to
Diazepam (Valium), Tizanidine ( Zanaflex) produce pictures of blood vessels and tissues in a part
-Used to relax skeletal muscle and decrease muscle spasm. of your body
Possible adverse effects: May cause drowsiness, dizziness, • The media contrast is injected through an intravenous (IV)
confusion, weakness line started in your arm or hand
Note:
anticonvulsants The media is called a contrast because it “lights up: blood
Carbamazepine (Tegretol), Clonazepam (Klonopin), vessels and tissues that are being tested
Diazepam (Valium), Phenobarbital (Luminal), Phenytoin Gadolinium yung iniinject
(Dilantin) Some patients are allergic to gadolinium
-Used to control seizures; act as a generalized CNS depressant.
Possible adverse effects: May cause drowsiness, ataxia, • b. CT Perfusion of the Head
sedation, among other symptoms. • Uses special x-ray equipment to show which areas of the
Antidepressants brain are adequately supplied with blood
*used to control depression • Provides detailed information about blood flow to the brain
Fluoxetine (Prozac), Monoamine Oxidase Inhibitors, • Cranial Magnetic Resonance Imaging
Sertraline (Zoloft), Tricyclics Amitriptyline • This type of testing is useful to determine the extent of
❖ Possible adverse effects: May cause anxiety, tremor, brain injury and identify potential structural abnormalities
insomnia, nausea. • More effective and sensitive than Computed Tomography
(CT)
Pt intervention Note:
Acute stage The media is called a contrast because it “lights up: blood
❑ Positioning strategies vessels and tissues that are being tested
❑ Improve respiratory and circulatory function Gadolinium yung iniinject
❑ Prevent pressure sores Some patients are allergic to gadolinium
❑ Prevent form deconditioning
POSt acute stage • Magnetic Resonance Angiography (MRA)
❑ 5 days a week for minimum of 3 hours of active • Type of MRI that looks specifically at the body’s blood
rehabilitation per day vessels
❑ Intensive rehabilitation if vitals are stable • Used to evaluate blood vessels and help identify
✓ Improve sensory function abnormalities or identify plaque formation
✓ Flexibility and joint integrity • Non-invasive
✓ Improve strength • Helpful in examining extracranial & intracranial cerebral
✓ Manage spasticity vessels
✓ Improve movement control
✓ Postural control and functional mobility
✓ Improve upper extremity function
✓ Managing shoulder pain
✓ Improve lower limb function
✓ Improve balance
✓ Improve locomotion
✓ Improve aerobic function
✓ Improve feeding and swallowing
✓ Improve motor learning
Patient and family education
❑ Give factual information, counsel family members about
the patients capabilities and limitations
❑ Provide open discussion and communication
❑ Be supportive, sensitive and maintain a positive
supporting nature
❑ Give psychological support
❑ Refer to help groups
Discharge planning
❑ Family member should participate daily in the therapy
session and learn exercises
❑ Home visits should be made prior to discharge
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
arthritis (particularly rheumatoid arthritis); and poor nutrition
(including malnutrition due to eating disorders).
• Osteogenesis imperfecta
-Osteogenesis imperfecta is a rare form of osteoporosis that is
present at birth. Osteogenesis imperfecta causes bones to
break for no apparent reason.
OSTEOPOROSIS • Idiopathic juvenile osteoporosis
• INTRODUCTION: -Idiopathic juvenile osteoporosis is rare. It occurs in children
Etiology between the ages of 8 and 14 or during times of rapid
• Results from insufficient bone formation growth. There is no known cause for this type of osteoporosis,
• Excessive bone resorption in which there is too little bone formation or excessive
• Combination of both bone loss. This condition increases the risk of fractures.
• • Bone fractures:
• 15% Postmenopausal Caucasian women (US) • Bruising
• 35%- women older than 65 years • Swelling
• 50%-women older than 50 years have Osteopenia of the • Deformity
femoral neck • Pain
• Risk factors: • Loss of function (compound fx)
• Genetics • Tenderness
• Female gender • Sometimes bone protrusion
• Positive family history • - Pt. may sometimes feel dizziness
• Racial characteristics associate with Caucasian, Asian or • Sick, faint resulting from shock
Hispanic background • Upon injury, a snapping or grinding noise is present
• Low body weight • OSTEOMALACIA
• -Modified Risk Factors: • Worsens bone pain
• Early menopause • Muscle weakness
• Early pregnancy • Dull aching of hips, lower back, pelvis, legs and ribs
• Smoking • Worse at night esp. when pressure is applied
• Sedentary lifestyle • Waddling gait
• Alcoholism • OSTEOPOROSIS
• Low body fat • Back pain (due to collapsed vertebra)
• Low calcium itake • Loss of height over time
• High caffeine intake • Stooped posture
• Prolonged bed rest • Prone to bone fractures much more easily
• Anorexia
• -Medical Risk Factors:
• Corticosteroids
• Diuretics
• Thyroid hormone preparations
• Epidemiology
-Fracture of the vertebrae and fracture of other bones such as
the proximal humerus, distal forearm, wrist proximal femur
(hip), and pelvis.
• Types:
• Type 1 Postmenopausal
-Type 1 or postmenopausal osteoporosis occurs in 5% to 20%
of women, affecting those within 15 to 20 years of
menopause, with a peak incidence in the 60s and early 70s.
The incidence in women is eight times higher than that in men.
The frequency of postmenopausal osteoporosis accounts for
the overall female-male ratio of 2:1 to 3:1.
• Type 2 Involutional
-Type 2 is generally seen in older age population a d has been
referred to as Senile Osteoporosis. Women are more prone to
develop Osteoporosis because of the contribution of the loss
estrogen to accelerated bone loss in the postmenopausal
female population. It occurs in women or men more than 70
years of age and usually is associated with decreased bone
formation along with decreased ability of the kidney to produce
1,25(OH)2D3. The vitamin D deficiency results in decreased
calcium absorption, which increases the PTH level and
therefore bone resorption. In type 2 osteoporosis, cortical and
trabecular bone is lost, primarily leading to increased risk of
hip, long bone, and vertebral fractures.
• Type 3 Secondary Osteoporosis
-Type 3 or secondary osteoporosis occurs equally in men and
women and at any age. In men, most cases are due to disease
or to drug therapy, but in 30% to 45% of affected individuals no
cause can be identified. In various series of osteoporotic De Lisa
patients, secondary osteoporosis accounts for about 40% of • Pharmacologic and nutritional treatment of bone mass
the total number of osteoporotic fractures seen by a physician. deficiency (Skeletal Osteopenia/Osteoporosis)
This type of osteoporosis is associated with a variety of ✓ Treatment of osteoporosis is directed at
conditions, including hormonal imbalances (eg, Cushing's preservation or improvement of bone mass at
syndrome); cancer (notably multiple myeloma); gastrointestinal the specific target sites. Because bone mass is
disorders (especially inflammatory bowel disease causing the principal, although not the only,
malabsorption); drug use (eg, corticosteroids, cancer determinant of fracture, such preservation or
chemotherapy, anticonvulsants, heparin, barbiturates, valporic improvement of bone mass s associated with a
acid, gonadotropin-releasing hormone [GnRH], excessive use reduce risk of fracture.
of aluminum-containing antacids); chronic renal failure; ✓ Mode of action of specific osteoporosis
hyperthyroidism; hypogonadism in men; immobilization; therapies
osteogenesis imperfecta and related disorders; inflammatory
• Nutritional adjuncts
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
o Calcium o Other bisphosphonates
✓ Mainstay of osteoporosis prevention o Tibolone
and treatment. Generally safe: milk • General Recommendations for Osteoporosis Therapy
and dairy products and calcium ✓ The above pharmacology should be
supplements are acceptable sources completed by avoidance of life-styles
of calcium. known to result in bone loss, including
o Vitamin D cigarette smoking, excessive alcohol
✓ 4 hundred to 800 UI if vitamin D, intake, a lack of exercise, lack of
administered in a multivitamins form, calcium intake, and so forth
is reasonable treatment for ✓ The use of calcium, a multiple vitamin
osteoporosis; whether the active with vitamin D, and a consideration of
forms of vitamin D such as calcitriol the approved forms of therapy for
are beneficial in osteoporosis is osteoporosis may definitely be of
unproven. value in preventing progression of
o Protein disease.
✓ Protein supplementation has been
shown to favorably affect outcomes in
• PATIENT ASSESSMENT FOR REHABILITION
✓ Depends on accurate diagnosis of the
patients who have sustained hip
degree of bone loss, as well as a
fractures.
determination of the degree of frailty
• Pharmacologic agents and propensity of the patient to fall.
o Bisphosphonates
✓ Have the ability to preserve and
increase bone mass at the spine and
• MANAGEMENT OF OSTEPOROSIS-RELATED
DISABILITY
hip, as well as to prevent fractures at
o Psychosocial considerations
each of these skeletal sites.
o Exercises
o Estrogen
1. Principle of specificity
✓ Mainstay of osteoporosis in women.
2. Principle of progression
Data exist to indicate estrogens may
3. Principle of reversibility
preserve bone mass at multiple
4. Principle of initial values
skeletal sites and prevent fracture.
5. Principle of diminishing returns
o Calcitonin
✓ Calcitonin studies do indicate its
ability to preserve bone density, and • Vertebral fracture
possibly prevent fractures. One of its o A multidisciplinary team approach is beneficial
benefits is its potential ability to to ensuring maintenance of function in this
decrease pain after acute population. Non-pharmacologic interventions
compression fracture in the spine, should be parentally used to manage chronic
presumably through a stimulation of back pain. Chronic back pain in the
beta-endorphins osteoporotic patient is managed by having the
o Raloxifene patient assume adequate recumbent bed rest
✓ Raloxifene (Evista) is FDA-approved for 20-30 minutes twice daily. This program is
in this class, for the treatment of supplemented by encouraging adjustments in
postmenopausal osteoporosis, and life-style, medications, physical agents,
prevention of bone loss in recently orthoses, and other therapies considered
postmenopausal women; it is not useful for chronic pain.
recommended for relief of • Hip fracture
menopausal symptoms (74). The use o These patient require the care of physiatrist,
of raloxifene physical therapist, and occupational therapist,
provides modest increases in bone as well as of nurses and social workers. The
mass, but reduction in the risk of benefits of the multidisciplinary approach have
vertebral fracture is 40% to 50%, and been documented as resulting in fewer
there is no reduction in nonvertebral transfers of acute emergencies, fewer
fractures (45). It also appears to postoperative complications, improved
reduce ambulation at the time if discharge, and fewer
the risk of estrogen-dependent breast discharge to nursing homes
cancer, but increases the risk of deep • Wrist fracture
vein thrombosis to a degree similar to o The primary goal of treatment to return of pain-
that of estrogen. Newer research in free normal function of the hand and wrist.
this class focuses on increased Initial casting usually extends above the elbow
benefit to and restricts movement of both elbow and
bones, heart and breast tissue wrist. During the period of mobilization, usually
hormone 6-8 weeks, strength and flexibility should be
o Parathyroid maintained in the upper extremities.
✓ Parathyroid hormone, or fragments of
the intact peptide molecule may be of
• Back supports and bracing in osteoporosis
o Bracing will be of value at certain times and in
in osteoporosis when administered
certain conditions associated with osteoporotic
parentally. Such as usage is based on
fractures. When able, it is best to utilize one’s
presumed anabolic effect of
own muscles to support the skeleton. However,
parathyroid hormone when
bracing is extremely useful to aid the patient
administered as a fragment, and it
who is in too much pain to function without
may be of value in established
support and is also helpful to prevent soft-
osteoporosis in terms of stimulating
tissue deformity and excessive loading of the
bone formation.
vertebral bodies
o Experimental therapies
✓ Estrogen agonist or antagonist such • Fall and fractures
as reloxifene, tamoxifen, idioxifene, o Because hip fractures have multifactorial
and droloxifene may have value in causes, interventions must aim not only at
preserving bone mass in increasing muscular strength, balance, and
osteoporosis. flexibility and reducing the forces of impact
when a fall occurs. Of utmost importance in the
• Non-FDA-Approved Drugs
success of a program aimed at preventing falls
o Sodium fluoride
is the educational component in reduction of
o Calcitriol
risk factors for falling. Home visit from
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
occupational therapist have been shown to be the disease. The DorsoOsteo Care spinal orthosis was
helpful in this. developed specifically for this purpose.
• Mechanism of falls The mode of operation is simple: The orthosis helps you
➢ Risk Factors for Falls straighten your upper body, thereby strengthening your
1. Environmental musculature, increasing bone regeneration and improving your
2. Medical posture.
3. Neuromuscular The DorsoOsteo Care is easy to put on and made of a soft,
4. Demographic comfortable and breathable material.
• Fear of falling
Bisphosphonates are a class of drugs that prevent the loss
of bone mass, used to treat osteoporosis and similar diseases.
❖ Physical medicine and rehabilitation strategies can be of
They are the most commonly prescribed drugs used to treat
value in the management of the osteoporotic patient and
osteoporosis.[1] They are called bisphosphonates because they
are currently underused. These strategies are used to
have two phosphonate(PO(OH)
reduce disability resulting from impairments in bone and
2) groups.
structure, muscle strength, and coordination.
Evidence shows that they reduce the risk of fracture in post-
Braddom
menopausal women with osteoporosis.[2][3][4][5][6]
Treatment
Bone undergoes constant turnover and is kept in balance
osteoporosis is a multifactorial condition and its treatment has
(homeostasis) by osteoblasts creating bone
several facets, so it requires a team approach. Endocrine
and osteoclasts destroying bone. Bisphosphonates inhibit the
consultation is needed, along with interventions from specialist in
digestion of bone by encouraging osteoclasts to
physical medicine and rehabilitation, pharmacology, psychology
undergo apoptosis, or cell death, thereby slowing bone loss.[7]
and nutrition. The prevention of falls decreases the risk of
The uses of bisphosphonates include the prevention and
fracture. A recent controlled trial demonstrated significant
treatment of osteoporosis, Paget's disease of bone, bone
improvement in risk of fall, balance, and unsteadiness of gait
metastasis (with or without hypercalcaemia), multiple
after 4-week spinal proprioceptive extension exercise dynamic
myeloma, primary hyperparathyroidism, osteogenesis
(SPEED) program.
imperfecta, fibrous dysplasia, and other conditions that exhibit
Exercise
bone fragility.
The efficacy of exercise for improving bone mass is supported by
hormonal and nutritional factors. To meet the challenge of
Bisphosphonates for Osteoporosis
mechanical load, skeletal tissue must have engaged bone mass
Examples
and proper architecture to withstand the physical strain that
imposed on it. It is fortunate that normal musculoskeletal Generic Name Brand Name
structure is highly adaptable and can meet the challenge of usual alendronate Fosamax
mechanical load. ibandronate Boniva
Posture Training Program and The Osteoporotic Skeletal
Frame risedronate Actonel, Atelvia
Orthoses and the Osteoporotic Spine zoledronic acid Reclast
❖ Treatment of Osteoporosis You take most bisphosphonates by mouth-every day, once or
➢ Medical Therapy of Spinal Osteoporosis twice a week, or even once a month. Zoledronic acid is
Calcitonin therapy decreases the rate of bone given intravenously (IV), usually only once each year. One form
loss in osteoporotic patients. Calcitonin works of ibandronate is also given intravenously, usually every 3
through the inhibition of bone resorption. months.
➢ Rehabilitation of Patients with Spinal How It Works
Osteoporosis Bisphosphonates are antiresorptive medicines, which means
✓ Acute fracture in the spine creates they slow or stop the natural process that dissolves bone tissue,
pain lasts about 1 to 2 weeks and resulting in maintained or increased bone density and strength.
sometimes requires bed rest. A This may prevent the development of osteoporosis.
transcutaneous electrical nerve If osteoporosis already has developed, slowing the rate of bone
stimulation (TENS) unit might also thinning reduces the risk of broken bones.
help in the treatment of chronic back Bisphosphonates may be taken by men or women.
pain secondary to spinal osteoporosis Why It Is Used
of the type II variety. After 2-week Bisphosphonates are commonly used for the prevention and
period, ambulation should be initiated treatment of osteopenia and osteoporosis.
if possible. Bisphosphonates are also used to treat other bone diseases
✓ The main reason for the application of such asPaget's disease.
thoracic orthosis is to prevent further How Well It Works
fracture by limiting motion in the Studies show that bisphosphonates increase bone thickness and
spine. may lower the risk of fractures.1
Therapy depends on the cause and type of osteoporosis. Initially Side Effects
it is intended to influence the bone metabolism in order to prevent All medicines have side effects. But many people don't feel the
bone fractures. If bone fractures have already occurred as a side effects, or they are able to deal with them. Ask your
result of osteoporosis, their acute treatment is required: this pharmacist about the side effects of each medicine you take.
means alleviating the pain associated with the fracture as well. Side effects are also listed in the information that comes with
Osteoporosis treatment is also intended to reduce or entirely your medicine.
eliminate possible permanent complaints. Here are some important things to think about:
Left untreated, bone degeneration continues so that the bones • Usually the benefits of the medicine are more important
become increasingly brittle. Beginning with osteoporosis than any minor side effects.
treatment as early as possible is therefore important. • Side effects may go away after you take the medicine
Orthoses can help stabilise and straighten the spine. They for a while.
improve the body posture and activate the torso musculature.
The products shown are fitting examples. Whether a product is
• If side effects still bother you and you wonder if you
should keep taking the medicine, call your doctor. He or she
actually suitable for you and whether you are capable of
may be able to lower your dose or change your medicine. Do not
exploiting the functionality of the product to its fullest depends on
suddenly quit taking your medicine unless your doctor tells you
many different factors. Amongst others, your physical condition,
to.
fitness and a detailed medical examination are key. Your doctor
or orthopedic technician will also decide which fitting is most
suited to you. We are happy to support you.
Activation of the musculature
Good treatment options for osteoporosis (bone degeneration) are
available in the meantime. Even at an early stage, promoting
muscle activity is helpful in order to delay the rapid progress of
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
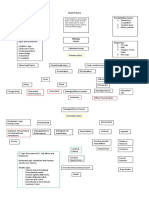
Parkinson’s disease Extrapyramidal- drug induced movements disorders that produce
• Epidemiology acute and tardive symptoms
• Progressive disorder of the central nervous system Wilson’s disease- autosomal recessive genetic disorder in which
• James Parkinson “paralysis agitans” copper accumulates in the body. Manifests n neurological or
• An extrapyramidal disorder by Kinnier Wilson psychiatric and liver symptoms
• Affects 7-10 million people worldwide Note:
• 2% of people older than 65 years of age has PD Alzheimers disease- is a type of dementia that causes
• Second to Alzheimer’s disease problems with memory, thinking and behavior. Symptoms
Note: usually develop slowly and get worse over time, becoming
Progressive disorder of the cns with motor and non motor severe enough to interfere with daily tasks.
symptoms, motor symptoms: rigidity, bradykinesia, tremor. Diffuse lewy body diseas- Lewy body dementia, these abnormal
Extrapyramidal- drug induced movement disorders. proteins are diffuse throughout other areas of the brain, including
the cerebral cortex. The brain chemical acetylcholine is depleted,
• Epidemiology causing disruption of perception, thinking and behavior.
• Increase substantially in the coming years due to the Subsancia nigra-reward and movement
aging of the population
• Common in men than women • Parkinson- plus syndrome
• Average onset: 50-60 years old • Affects the substancia nigra
• Early onset: less than 40 years old • Produces parkinsonian symptoms with other neurological
• Young onset: between 21 and 40 years of age sign
• Juvenile onset: less than 21 years old 1. Alzheimer’s disease- progressive type of dementia
• Etiology 2. Diffuse Lewy body disease (DLBD)
• Can be both genetic and environmental Features:
• Parkinsonism- generic term used to describe a group of • Indistinguishable rigidity and bradykinesia from PD
disorders with primary disturbances in the dopamine • typically do not show measurable improvement from the
systems of the basal ganglia. administration of anti-Parkinson medications such as
1. Idiopathic Parkinsonism levodopa (L-dopa) therapy
2. Secondary Parkinsonism • Cardinal Features:
3. Parkinson-Plus Syndrome • Rigidity
Note: • Bradykinesia
Basal ganglia- a group of structures linked to the thalamus in the • Postural Instability
base of the brain and involved in coordination of movement. • Tremor
• Disruption in daily functions
• Etiology • depression
• PARKINSONISM note:
• Idiopathic Parkinsonism Triad of PD:
• Secondary Parkinsonism • RIGIDITY
1. Postencephalitic Parkinsonism • BRADYKINESIA
2. Toxic Parkinsonism • PSTURAL INSTABILITY
3. Drug-Induced Parkinsonism (DIP)
• Parkinsonism-plus syndrome
1. Alzheimer’s disease
2. Diffuse Lewy body disease (DLBD)
3. Normal pressure hydrocephalus (NPH)
4. Creutzfeldt-Jakob disease (CJD)
5. Wilson’s disease (WD)
6. Juvenile Huntington’s disease
• Parkinson’s disease
• Also known as Idiopathic Parkinsonism
• Idiopathic or genetic mutation
• Most common. 78% are affected
• Two clinical subgroups(symptoms):
1. Postural instability and gait disturbances
2. Tremor predominant
Genes:
1. Casual genes that produces the disease
2. Genes that don’t cause the PD but increase the risk of
developing it
• Secondary parkinsonism
• Postencephalictic Parkinsonism-influenza epidemic of
encephalitis lethargica
• Toxic Parkinsonism- exposed to environmental toxins and
industrial chemicals.
• Drug-induced Parkinsonism- drugs that produce
extrapyramidal dysfunction that mimics signs of PD.
Ex:
1. Neuroleptic drugs
• Rare cases:
• Metabolic conditions
- Hypoparathyroidism
- Hyperparathyroidism
Note:
Postencephalictic- parkinsonian symptoms occurred. may slow
virus na nagiinfect ng brain
- Occurred nung 1917-1926, many indi were affected
Toxic parkinsonism- parkinsonian symptoms occur in harmful
chemicals like AGENT ORANGE- a herbicide in the US. Then
manganese, carbon monoxide etc etc.
MPTP- is a prodrug to the neurotoxin MPP+, which causes
permanent symptoms of Parkinson's disease by destroying
dopaminergic neurons in the substantia nigra of the brain. It has
been used to study disease models in various animal studies.
Drug induced- blocks the dopamine receptors
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
IV. Medical Diagnosis • Familial incidence: 5%
❖ The diagnosis of Parkinson disease is primarily clinical made Sullivan:
by a neurologist.
❖ Bedside cognitive evaluation can be normal early in the • Affects 7-10 million people worldwide
disease process. • 2% of people older than 65 years of age has PD
▪ A detailed history of your current and past • Second to Alzheimer’s disease
medications, to make sure you are not taking • Increase substantially in the coming years due to the
medications that can cause symptoms similar to aging of the population
PD. • Common in men than women (1.2 to 1.5 frequently)
▪ A detailed medical history and physical • Average onset: 50-60 years old
examination. • Early onset: less than 40 years old
▪ A detailed neurological examination during which a • Young onset: between 21 and 40 years of age
neurologist will ask you to perform tasks to assess • Juvenile onset: less than 21 years old
the agility of arms and legs, muscle tone, your gait
Etiology:
and your balance.
• Parkinsonism- generic term used to describe a group of
❖ In order to diagnose a patient with Parkinson’s disease, the disorders with primary disturbances in the dopamine
following must be observed/assessed: systems of the basal ganglia
✓ Tremor or paucity of spontaneous movements • Idiopathic parkinsonism or parkinson’s disease- most
✓ Resistance to movement of the limb during ROM common form, affecting 78% of pts.
examination • Secondary parkinsonism is a result from different
✓ Motor examination—which in PD is asymmetric in the identifiable cause
early stages of the disease • Parkinsonism plus syndromes refers to those conditions
✓ Gait observation that mimics PD.
*If a patient uses more than five steps to complete a 180
degree turn, PD should be considered. Parkinson’s disease
✓ It is also helpful to watch for certain cardinal symptoms
such early vertical eye movement abnormalities, early • Idiopathic or genetically identififed
autonomic failure or hyperreflexia, Babinski’s sign, • 2 clinical subgroups:
ataxia and peripheral neuropathy. 1. Postural instability and gait disturbances
2. Tremor predominant
❖ Triad of Parkinsonism
Genetic- represents 10% cases overall. PARK1, PINK1,LRRK2,
➢ Tremor
DJ-1, and glucocerebrosidase, are some examples.
➢ Rigidity 2 categories:
➢ Bradykinesia 1. Casual genes that causes the mutation
2. Associated genes that increases in developing PD.
❖ Parkinson Disease is diagnosed based on the patient’s
medical history and symptoms evaluated during the Secondary Parkinsonism
neurological examination so in order to rule out other
neurological disorders, CT scan, MRI or PET may be used. • Postencpehalictic Parkinsonism
• Toxic Parkinsonism- individuals that are exposed to
❖ The differential diagnosis of Parkinson Disease is wide. The toxins and industrial chemicals
rigidity can be mistaken for the stiffness of arthritis, the • Drug induces parkinsonism- variety of drugs that can
postural changes can be associated to osteoporosis or produce extrapyramidal dysfunction that mimics PD:
degenerative spine disease, the bradykinesia and masklike 1. Neuroleptic drugs
facies can be mistaken for depression. 2. Antidepressant drugs
3. Antihypertensive drugs
• Rare cases: metabolic conditions.
❖ As Parkinson Disease advances: 1. BG calcification
➢ Obstructive and restrictive pulmonary disease 2. Hypothyroidism
➢ Speech can be rapid and monotonous and have low 3. Hyperthyroidism
volume with poor articulation and inappropriate periods 4. Wilson’s disease
of silence
Parkinson-plus Syndrome
➢ Hand writing can become small and cramped
(microphagia)
• A group of neurodegenerative diseases can affect the
➢ Dementia and depression
substancianigra and produce parkinsonian symptoms
Autonomic dysfunction with increased salivation, drooling, along with neurological signs.
orthostasis, increased perspiration, constipation, hyperreflexic • Diseases include:
bladder with incontinence, dysphagia 1. progressive supranuclear palsy (PSPO)
2. Alzheimer’s disease
I. INTRODUCTION 3. diffuse Lewy body disease (DLBD)
4. normal pressure hydrocephalus (NPH)
Parkinson’s disease
5. Creutzfeldt-Jakob disease (CJD)
6. Wilson’s disease (WD)
• A progressive disorder of the central nervous system
7. juvenile Huntington’s disease
• James Parkinson “paralysis agitans”
• An extrapyramidal disorder by Kinnier Wilson
Epidemiology: Lindsay:
Severe and permanent parkinsonism has been inadvertently
produced in individuals who injected a synthetic heroin containing
• Annual incidence: 20 per 10000 the chemical MPTP (1-methyl-4-phenyl-1,2,3,6- tetra/
hydropyridine)
• Prevalence: 90 per 100000
• Sex: Male:Female-3:2
• Age of onset: 50y/old
Downloaded by sheila roma sibug (srasibug@gmail.com)
lOMoARcPSD|3537447
Downloaded by sheila roma sibug (srasibug@gmail.com)
Das könnte Ihnen auch gefallen
- Non-Modifiable, Partially Modifiable, and Modifiable Risk Factors for Atherothrombotic DiseaseDokument15 SeitenNon-Modifiable, Partially Modifiable, and Modifiable Risk Factors for Atherothrombotic DiseaseWiljohn de la CruzNoch keine Bewertungen
- Cva (Npte)Dokument16 SeitenCva (Npte)papermannerNoch keine Bewertungen
- Medicina 4 Neuro Neumo PDFDokument19 SeitenMedicina 4 Neuro Neumo PDFKarol M MChNoch keine Bewertungen
- Stroke CMDokument1 SeiteStroke CMMariel Febreo MerlanNoch keine Bewertungen
- Nursing Care of Stroke - NewDokument4 SeitenNursing Care of Stroke - Newninda saputriNoch keine Bewertungen
- Stroke Signs, Risks, and Nursing CareDokument1 SeiteStroke Signs, Risks, and Nursing CareMariel Febreo MerlanNoch keine Bewertungen
- Neurology MnemonicsDokument11 SeitenNeurology MnemonicsOstaz100% (1)
- Symptom differential and workup guideDokument5 SeitenSymptom differential and workup guidemonica ortizNoch keine Bewertungen
- Brain OdemaDokument2 SeitenBrain OdemaMohamed Nasreldin HamdoonNoch keine Bewertungen
- Cerebrovascular Syndromes: The Neurosurgical AtlasDokument8 SeitenCerebrovascular Syndromes: The Neurosurgical AtlasEduardo Reyna MartínezNoch keine Bewertungen
- Step 2 CS Differential DiagnosesDokument4 SeitenStep 2 CS Differential DiagnosesnaimNoch keine Bewertungen
- Ischemic Stroke: The Normal Blood Supply To The Brain Is DisruptedDokument5 SeitenIschemic Stroke: The Normal Blood Supply To The Brain Is DisruptedMelchora Lea Castro SorianoNoch keine Bewertungen
- OCCLUSIONS & PATHOLOGIES OF THE CNS BLOOD SUPPLYDokument1 SeiteOCCLUSIONS & PATHOLOGIES OF THE CNS BLOOD SUPPLYFaye Stephanie CantagoNoch keine Bewertungen
- Pericarditis Vs Mi: Internal Medicine: CvsDokument6 SeitenPericarditis Vs Mi: Internal Medicine: CvsRojales FrancisNoch keine Bewertungen
- Subdural Hemotoma PathopgysiologyDokument1 SeiteSubdural Hemotoma PathopgysiologyChris-Gen 'JHAII' SeratoNoch keine Bewertungen
- Stroke RehabilitationDokument57 SeitenStroke RehabilitationWahyu FajarNoch keine Bewertungen
- PT Management & Problems of The CV System - Part 3 Cheat SheetDokument3 SeitenPT Management & Problems of The CV System - Part 3 Cheat SheetGayle MarieNoch keine Bewertungen
- Medicine Cheat SheetsDokument16 SeitenMedicine Cheat SheetsRisa Muthmainah100% (1)
- Hypertensive ICHDokument49 SeitenHypertensive ICHmingchuan chuNoch keine Bewertungen
- Res 113Dokument197 SeitenRes 113Belinda ELISHANoch keine Bewertungen
- Osms - It/alzheimers-Disease: Pathology & CausesDokument1 SeiteOsms - It/alzheimers-Disease: Pathology & Causesdysa ayu shalsabilaNoch keine Bewertungen
- Oxford Stroke ClassificationDokument1 SeiteOxford Stroke ClassificationSyimah UmarNoch keine Bewertungen
- Disease/syndrome Inciting Incident Structures Affected PoliomyelitisDokument12 SeitenDisease/syndrome Inciting Incident Structures Affected PoliomyelitismrhemmatNoch keine Bewertungen
- Neurorehabilitation 1: Stroke, TBI, MS, PD, GBS, and ALS ExaminationDokument439 SeitenNeurorehabilitation 1: Stroke, TBI, MS, PD, GBS, and ALS ExaminationDuncan D'AmicoNoch keine Bewertungen
- StrokeDokument6 SeitenStrokeDana CastroNoch keine Bewertungen
- Clinical Medicine Cheat Sheet Ebook PDFDokument18 SeitenClinical Medicine Cheat Sheet Ebook PDFMokaNoch keine Bewertungen
- Medgeeks Clinical Cheat SheetsDokument18 SeitenMedgeeks Clinical Cheat SheetsRishikesh AsthanaNoch keine Bewertungen
- Epinephrine cardiac arrest arrhythmias anaphylaxisDokument1 SeiteEpinephrine cardiac arrest arrhythmias anaphylaxisMia GarciaNoch keine Bewertungen
- 12 NeoDokument1 Seite12 Neogocelij948Noch keine Bewertungen
- FINALe ISCHEMIC STROKES NEUROSURGDokument13 SeitenFINALe ISCHEMIC STROKES NEUROSURGadrian kristopher dela cruzNoch keine Bewertungen
- Pathophysiology of Head TraumaDokument2 SeitenPathophysiology of Head TraumaGrace Jane Dionaldo100% (1)
- Concept Map TBIDokument2 SeitenConcept Map TBIraquel maniego67% (3)
- REHABILITASI MEDIK PADA PENDERITA STROKEDokument55 SeitenREHABILITASI MEDIK PADA PENDERITA STROKEKrisma susantiNoch keine Bewertungen
- Medicine Revision - Neurology TableDokument10 SeitenMedicine Revision - Neurology TableUnomoshNoch keine Bewertungen
- Vascular Disturbances (Module C) Cerebrovascular Accident (Cva)Dokument3 SeitenVascular Disturbances (Module C) Cerebrovascular Accident (Cva)RosmaryNoch keine Bewertungen
- Tentiran Bedah SarafDokument56 SeitenTentiran Bedah Sarafnazila hanaNoch keine Bewertungen
- Neurology LocalizationDokument6 SeitenNeurology LocalizationPramod ThapaNoch keine Bewertungen
- Cutting Edge Acute Stroke Management StrategiesDokument15 SeitenCutting Edge Acute Stroke Management StrategiesLuis Miguel VillanuevaNoch keine Bewertungen
- Gagal Jantung ULM-1Dokument66 SeitenGagal Jantung ULM-1EeqNoch keine Bewertungen
- Genetics MnemonicsDokument5 SeitenGenetics MnemonicsYASSERNoch keine Bewertungen
- Clerkship Secrets Part 1Dokument33 SeitenClerkship Secrets Part 1obanoyenfawaz98Noch keine Bewertungen
- Gambar. Gambaran Karakteristik CephalgiaDokument4 SeitenGambar. Gambaran Karakteristik Cephalgiadella rafika sariNoch keine Bewertungen
- Traumatic Brain Injuries Study GuideDokument18 SeitenTraumatic Brain Injuries Study GuideCarl Elexer Cuyugan Ano100% (1)
- Neurologic DisturbancesssDokument2 SeitenNeurologic DisturbancesssSJane FeriaNoch keine Bewertungen
- Rehab Cheat SheetDokument18 SeitenRehab Cheat SheetZ A100% (3)
- Cardio My Opa Thies ChartDokument2 SeitenCardio My Opa Thies ChartSolomon Seth SallforsNoch keine Bewertungen
- Stroke ClinicsDokument136 SeitenStroke ClinicsIvonne GómezNoch keine Bewertungen
- Stroke CVDDokument9 SeitenStroke CVDangel.senido0198Noch keine Bewertungen
- Hemorrhagic Stroke: Darpen Subhashbhai Mori Group 2, MD 3BDokument13 SeitenHemorrhagic Stroke: Darpen Subhashbhai Mori Group 2, MD 3BDarpen MoriNoch keine Bewertungen
- Terminology of PsychiatryDokument6 SeitenTerminology of PsychiatryHassan.shehri100% (1)
- 5 Major Stroke Syndromes: Recognition, Action & OutcomesDokument43 Seiten5 Major Stroke Syndromes: Recognition, Action & OutcomesweezerNoch keine Bewertungen
- Disease Comparison ChartDokument36 SeitenDisease Comparison ChartSara S. CastañedaNoch keine Bewertungen
- 64 Yr Old Male With Previous History of Heart Attack Came To Casualty With C/o Sudden Onset of Pain in The Right Leg Below The Knee. On ExaminationDokument47 Seiten64 Yr Old Male With Previous History of Heart Attack Came To Casualty With C/o Sudden Onset of Pain in The Right Leg Below The Knee. On ExaminationSyed Irfan ArifNoch keine Bewertungen
- Patoflowdiagram Stroke: Stroke Non Hemoragic Stroke HemoragicDokument1 SeitePatoflowdiagram Stroke: Stroke Non Hemoragic Stroke HemoragicSelvi IceNoch keine Bewertungen
- Neurology - Weakness PatternsDokument2 SeitenNeurology - Weakness PatternsAnisah AliNoch keine Bewertungen
- Dementia Recentupdates 130920080812 Phpapp01Dokument58 SeitenDementia Recentupdates 130920080812 Phpapp01SantanuNoch keine Bewertungen
- Left Mca Infarct Nobe PathoDokument1 SeiteLeft Mca Infarct Nobe PathoNoveeNoch keine Bewertungen
- Paediatrics: Acyanotic Heart DiseaseDokument5 SeitenPaediatrics: Acyanotic Heart Diseasecgao30Noch keine Bewertungen
- Neurology Multiple Choice Questions With Explanations: Volume IIVon EverandNeurology Multiple Choice Questions With Explanations: Volume IIBewertung: 5 von 5 Sternen5/5 (2)
- Hidden Disabilities and Conditions: Creating an Inclusive WorkplaceVon EverandHidden Disabilities and Conditions: Creating an Inclusive WorkplaceNoch keine Bewertungen
- Chapter 2-9Dokument48 SeitenChapter 2-9sheila roma sibugNoch keine Bewertungen
- Chapter 2Dokument13 SeitenChapter 2sheila roma sibugNoch keine Bewertungen
- Chapter 2 Physical Therapy ModalitiesDokument54 SeitenChapter 2 Physical Therapy Modalitiessheila roma sibugNoch keine Bewertungen
- Schucmann Retest ADokument10 SeitenSchucmann Retest Asheila roma sibugNoch keine Bewertungen
- CHAPTER 12 NeuromusculoskeletalDokument8 SeitenCHAPTER 12 Neuromusculoskeletalsheila roma sibugNoch keine Bewertungen
- Chapter 2 Physical Therapy ModalitiesDokument54 SeitenChapter 2 Physical Therapy Modalitiessheila roma sibugNoch keine Bewertungen
- Javascript The Web Warrior Series 6Th Edition Vodnik Test Bank Full Chapter PDFDokument31 SeitenJavascript The Web Warrior Series 6Th Edition Vodnik Test Bank Full Chapter PDFtina.bobbitt231100% (10)
- Overlord Volume 1 - The Undead King Black EditionDokument291 SeitenOverlord Volume 1 - The Undead King Black EditionSaadAmir100% (11)
- International Standard Knowledge Olympiad - Exam Syllabus Eligibility: Class 1-10 Class - 1Dokument10 SeitenInternational Standard Knowledge Olympiad - Exam Syllabus Eligibility: Class 1-10 Class - 1V A Prem KumarNoch keine Bewertungen
- Addendum Dokpil Patimban 2Dokument19 SeitenAddendum Dokpil Patimban 2HeriYantoNoch keine Bewertungen
- Role of Rahu and Ketu at The Time of DeathDokument7 SeitenRole of Rahu and Ketu at The Time of DeathAnton Duda HerediaNoch keine Bewertungen
- Communication Tourism PDFDokument2 SeitenCommunication Tourism PDFShane0% (1)
- MVD1000 Series Catalogue PDFDokument20 SeitenMVD1000 Series Catalogue PDFEvandro PavesiNoch keine Bewertungen
- Detailed Lesson PlanDokument5 SeitenDetailed Lesson PlanHazel Mae HerreraNoch keine Bewertungen
- TITLE 28 United States Code Sec. 3002Dokument77 SeitenTITLE 28 United States Code Sec. 3002Vincent J. Cataldi91% (11)
- Database Interview QuestionsDokument2 SeitenDatabase Interview QuestionsshivaNoch keine Bewertungen
- Red Orchid - Best PracticesDokument80 SeitenRed Orchid - Best PracticeslabiaernestoNoch keine Bewertungen
- Sample Letter of Intent To PurchaseDokument2 SeitenSample Letter of Intent To PurchaseChairmanNoch keine Bewertungen
- What Is Love? - Osho: Sat Sangha SalonDokument7 SeitenWhat Is Love? - Osho: Sat Sangha SalonMichael VladislavNoch keine Bewertungen
- Arpia Lovely Rose Quiz - Chapter 6 - Joint Arrangements - 2020 EditionDokument4 SeitenArpia Lovely Rose Quiz - Chapter 6 - Joint Arrangements - 2020 EditionLovely ArpiaNoch keine Bewertungen
- EAPP Q2 Module 2Dokument24 SeitenEAPP Q2 Module 2archiviansfilesNoch keine Bewertungen
- DRRR STEM 1st Quarter S.Y.2021-2022Dokument41 SeitenDRRR STEM 1st Quarter S.Y.2021-2022Marvin MoreteNoch keine Bewertungen
- Inline check sieve removes foreign matterDokument2 SeitenInline check sieve removes foreign matterGreere Oana-NicoletaNoch keine Bewertungen
- 12 Preliminary Conference BriefDokument7 Seiten12 Preliminary Conference Briefkaizen shinichiNoch keine Bewertungen
- 740LIDokument13 Seiten740LIm FaisalNoch keine Bewertungen
- DLL - Science 6 - Q3 - W3Dokument6 SeitenDLL - Science 6 - Q3 - W3AnatasukiNoch keine Bewertungen
- My PDSDokument16 SeitenMy PDSRosielyn Fano CatubigNoch keine Bewertungen
- Supply Chain AssignmentDokument29 SeitenSupply Chain AssignmentHisham JackNoch keine Bewertungen
- MiQ Programmatic Media Intern RoleDokument4 SeitenMiQ Programmatic Media Intern Role124 SHAIL SINGHNoch keine Bewertungen
- Mastering ArpeggiosDokument58 SeitenMastering Arpeggiospeterd87Noch keine Bewertungen
- IndiGo flight booking from Ahmedabad to DurgaPurDokument2 SeitenIndiGo flight booking from Ahmedabad to DurgaPurVikram RajpurohitNoch keine Bewertungen
- Digi-Notes-Maths - Number-System-14-04-2017 PDFDokument9 SeitenDigi-Notes-Maths - Number-System-14-04-2017 PDFMayank kumarNoch keine Bewertungen
- Compound SentenceDokument31 SeitenCompound Sentencerosemarie ricoNoch keine Bewertungen
- TAX & DUE PROCESSDokument2 SeitenTAX & DUE PROCESSMayra MerczNoch keine Bewertungen
- Examination of InvitationDokument3 SeitenExamination of InvitationChoi Rinna62% (13)
- AI Capstone Project Report for Image Captioning and Digital AssistantDokument28 SeitenAI Capstone Project Report for Image Captioning and Digital Assistantakg29950% (2)