Das könnte Ihnen auch gefallen
- Ophthalmology Clerks Revalida Review 2017Dokument94 SeitenOphthalmology Clerks Revalida Review 2017Mara Medina - Borleo100% (1)
- Part 1Dokument15 SeitenPart 1solimanmahmoudaNoch keine Bewertungen
- Conjunctivitis: Radang Konjungtiva Yang Menutupi Belakang Kelopak Dan Bola Mata, Dalam Bentuk Akut Maupun KronisDokument18 SeitenConjunctivitis: Radang Konjungtiva Yang Menutupi Belakang Kelopak Dan Bola Mata, Dalam Bentuk Akut Maupun KronisnasikaceliaNoch keine Bewertungen
- OSCE RTS NotesDokument7 SeitenOSCE RTS NotesSafwaan SyedNoch keine Bewertungen
- ConjunctivitisDokument4 SeitenConjunctivitisKumar ShivamNoch keine Bewertungen
- Ocular Emergencies-Sept2013 PDFDokument22 SeitenOcular Emergencies-Sept2013 PDFKaramsi Gopinath NaikNoch keine Bewertungen
- Ettinger CH 11 - Ophthalmic Manifestations of Systemic DiseaseDokument6 SeitenEttinger CH 11 - Ophthalmic Manifestations of Systemic Diseasehalf_frozen_cho6435Noch keine Bewertungen
- Eye Problems: Dr. Gitalisa Andayani, SPMDokument88 SeitenEye Problems: Dr. Gitalisa Andayani, SPMhasanajNoch keine Bewertungen
- Referat Acute Liver FailureDokument124 SeitenReferat Acute Liver FailurepanduNoch keine Bewertungen
- Red EyeDokument54 SeitenRed EyeT786 kharNoch keine Bewertungen
- OpthalDokument15 SeitenOpthalWaiwit KritayakiranaNoch keine Bewertungen
- The Acute Painful Red Eye: History of Presenting Complaint - The Time and Speed of OnsetDokument4 SeitenThe Acute Painful Red Eye: History of Presenting Complaint - The Time and Speed of Onsetleigh_zaliNoch keine Bewertungen
- Ophthalmology NotesDokument79 SeitenOphthalmology NotesWise AmroNoch keine Bewertungen
- ConjungtivitisDokument86 SeitenConjungtivitisIvo AfianiNoch keine Bewertungen
- Kul Mata Merah PDFDokument56 SeitenKul Mata Merah PDFMuhammad HasanNoch keine Bewertungen
- Opt Halm OlogyDokument87 SeitenOpt Halm OlogyAya MahmoudNoch keine Bewertungen
- Clinical App Red Eye Without Blurred VisionDokument38 SeitenClinical App Red Eye Without Blurred VisionPriskila SamanthaNoch keine Bewertungen
- Angle Closure GlaucomaDokument21 SeitenAngle Closure Glaucomasri sinagaNoch keine Bewertungen
- Acne, Physical Dermatoses, Bacterial InfectiosDokument35 SeitenAcne, Physical Dermatoses, Bacterial InfectiosRiena Austine Leonor NarcillaNoch keine Bewertungen
- Ophtha ReviewerDokument3 SeitenOphtha ReviewerToni Sy EncinaresNoch keine Bewertungen
- Common Eye ProblemsDokument33 SeitenCommon Eye ProblemsrobyalfNoch keine Bewertungen
- Red Eye - Conjunctivitis I Dr. Nuke Erlina Mayasari, SPMDokument23 SeitenRed Eye - Conjunctivitis I Dr. Nuke Erlina Mayasari, SPMismkipendprowil2Noch keine Bewertungen
- Care For Patients With Alteration in Perception and CoordinationDokument12 SeitenCare For Patients With Alteration in Perception and Coordinationevlujtrep9690100% (1)
- SENSESDokument5 SeitenSENSESjsreyes.402Noch keine Bewertungen
- Post Test JWB NCLDokument12 SeitenPost Test JWB NCLSummer SnowNoch keine Bewertungen
- Leukoderma and VitiligoDokument82 SeitenLeukoderma and VitiligoBahaa ShaabanNoch keine Bewertungen
- Bahan Pemicu 5 Penginderaan: Ivan Buntara 405120049Dokument62 SeitenBahan Pemicu 5 Penginderaan: Ivan Buntara 405120049AdamNoch keine Bewertungen
- Red Eye TableDokument2 SeitenRed Eye TableFatimah AlsultanNoch keine Bewertungen
- Dis. of Ant ChamberDokument75 SeitenDis. of Ant Chambertajir cetajirNoch keine Bewertungen
- Differential Diagnosis of The Red Eye PDFDokument19 SeitenDifferential Diagnosis of The Red Eye PDFAjeng PuspitasariNoch keine Bewertungen
- (Ophtha) Ocular Emergencies .PenguinDokument7 Seiten(Ophtha) Ocular Emergencies .PenguinPatricia ManaliliNoch keine Bewertungen
- Case ReportDokument43 SeitenCase ReporttsazuuNoch keine Bewertungen
- 3-Painless Red EyeDokument40 Seiten3-Painless Red Eyetaha obaidNoch keine Bewertungen
- Tatalaksana Awal Kegawatdaruratan Pada Mata - Dr. Nuke Erlina Mayasari, SPMDokument23 SeitenTatalaksana Awal Kegawatdaruratan Pada Mata - Dr. Nuke Erlina Mayasari, SPMwahyu ardiNoch keine Bewertungen
- The Red EyeDokument42 SeitenThe Red EyeDenise CarbonellNoch keine Bewertungen
- Gochi Notes: Immuno-Allergy Part Vi Lecturer: Dra. Eva DizonDokument2 SeitenGochi Notes: Immuno-Allergy Part Vi Lecturer: Dra. Eva DizonJustin TayabanNoch keine Bewertungen
- Ophthalmology - Diseases of ConjunctivaDokument11 SeitenOphthalmology - Diseases of ConjunctivajbtcmdtjjvNoch keine Bewertungen
- Stockwell - The Red Eye ExpressDokument31 SeitenStockwell - The Red Eye ExpressSiti HaniwidiyaNoch keine Bewertungen
- A Painful Red Eye: Case StudyDokument2 SeitenA Painful Red Eye: Case StudyAmber WangNoch keine Bewertungen
- Eye InfectionDokument4 SeitenEye Infectionhans leeNoch keine Bewertungen
- Selected Differential Diagnosis of Red Eye: Table 1Dokument3 SeitenSelected Differential Diagnosis of Red Eye: Table 1Rian DamayantiNoch keine Bewertungen
- Ocular EmergDokument41 SeitenOcular EmergMohd SyazrinNoch keine Bewertungen
- Eye Notes From LectureDokument2 SeitenEye Notes From LectureTeehee JonesNoch keine Bewertungen
- Trauma OkuliDokument50 SeitenTrauma Okuliaditya brahmantio sujakaNoch keine Bewertungen
- Red Eye: Education Session SevenDokument20 SeitenRed Eye: Education Session SevenHendry SetiawanNoch keine Bewertungen
- Approach To Red Eye in PHC: DR - Zinab Alatawi Family Medicine MD, SRDokument57 SeitenApproach To Red Eye in PHC: DR - Zinab Alatawi Family Medicine MD, SROne life To live SaudiahNoch keine Bewertungen
- Derm Summary Table PDFDokument33 SeitenDerm Summary Table PDFVas LillaNoch keine Bewertungen
- Non Mechanical and Chemical InjuriesDokument14 SeitenNon Mechanical and Chemical InjuriesMuaz AbdullahNoch keine Bewertungen
- Penurunan VisusDokument117 SeitenPenurunan Visusdevi taqiyyahNoch keine Bewertungen
- عملي السليداتDokument92 Seitenعملي السليداتSandyDavidNoch keine Bewertungen
- Iseases of The Anterior Segment: Department of Ophthalmology Medical University of Warsaw Head: Prof. J.P. SzaflikDokument54 SeitenIseases of The Anterior Segment: Department of Ophthalmology Medical University of Warsaw Head: Prof. J.P. SzaflikAmalNoch keine Bewertungen
- HEENTDokument19 SeitenHEENTMARIAN FRACNoch keine Bewertungen
- Special Senses 2014 - 1Dokument91 SeitenSpecial Senses 2014 - 1Winz DolleteNoch keine Bewertungen
- Bacterial ConjunctivitisDokument5 SeitenBacterial ConjunctivitisBnB UsmleNoch keine Bewertungen
- Kegawatdarutan Mata Dalam Konsep DogaDokument68 SeitenKegawatdarutan Mata Dalam Konsep DogaDavi DzikirianNoch keine Bewertungen
- Pediatrics OptometryDokument59 SeitenPediatrics Optometryendalew mulugetaNoch keine Bewertungen
- Common Eye Diseases 2022Dokument33 SeitenCommon Eye Diseases 2022Shia LevyNoch keine Bewertungen
- Case Bacterial KeratitisDokument44 SeitenCase Bacterial KeratitisPagolu BavyaNoch keine Bewertungen
- 8a) Chronic DacryocystitisDokument5 Seiten8a) Chronic DacryocystitisDasNoch keine Bewertungen
- Core Challenge Workout CalendarDokument1 SeiteCore Challenge Workout CalendarJYGNoch keine Bewertungen
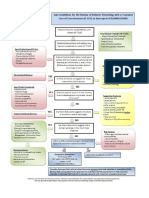
- Syncope AlgorithmDokument1 SeiteSyncope AlgorithmJYGNoch keine Bewertungen
- Background: Alpha-1 Antitrypsin DeficiencyDokument2 SeitenBackground: Alpha-1 Antitrypsin DeficiencyJYGNoch keine Bewertungen
- Drug Name Function Mechanism of ActionDokument1 SeiteDrug Name Function Mechanism of ActionJYGNoch keine Bewertungen
- Comparison of Efficacy of Lidocaine 2% Gel With Lidocaine 2% Injection in Chalazion SurgeryDokument4 SeitenComparison of Efficacy of Lidocaine 2% Gel With Lidocaine 2% Injection in Chalazion Surgeryjheimyav07Noch keine Bewertungen
- NEJMPsilocybinDokument12 SeitenNEJMPsilocybinpaul casillasNoch keine Bewertungen
- Pharmaceutics IntroductionDokument9 SeitenPharmaceutics IntroductionVIJAY KUMAR TIRUKKACHINoch keine Bewertungen
- Antenatal Diet PlanDokument7 SeitenAntenatal Diet PlanSunija Selvam100% (3)
- Annotated BibDokument3 SeitenAnnotated Bibapi-489789428Noch keine Bewertungen
- RNI For Malaysians-SummaryDokument2 SeitenRNI For Malaysians-SummaryAimi Hannani100% (1)
- Abscess Incision and Drainage NEJMDokument4 SeitenAbscess Incision and Drainage NEJMMarcela CharryNoch keine Bewertungen
- Information To Be Included Within A Coal Mining Risk AssessmentDokument2 SeitenInformation To Be Included Within A Coal Mining Risk AssessmentAlf HorsemanNoch keine Bewertungen
- Greywater Filtration Systems: For A Sustainable Water CultureDokument36 SeitenGreywater Filtration Systems: For A Sustainable Water CultureJen Beatrice DiazNoch keine Bewertungen
- Therapeutic CommanalitiesDokument8 SeitenTherapeutic CommanalitiesRoshni TripathyNoch keine Bewertungen
- The Healthy Bones Nutrition Plan and Cookbook - IntroductionDokument10 SeitenThe Healthy Bones Nutrition Plan and Cookbook - IntroductionChelsea Green PublishingNoch keine Bewertungen
- Emu HusbandryDokument126 SeitenEmu HusbandrySHANMUGAPRIYAN100% (2)
- Mary AinsworthDokument2 SeitenMary AinsworthMae Kris Sande Rapal100% (1)
- Surgical SkillsDokument47 SeitenSurgical SkillsSamah SuhailNoch keine Bewertungen
- 13.loading of Dental ImplantsDokument166 Seiten13.loading of Dental ImplantsHarpreet Singh100% (3)
- Top 10 Stress Management TechniquesDokument5 SeitenTop 10 Stress Management TechniquesMaryjane YaranonNoch keine Bewertungen
- Unit 9 TestDokument6 SeitenUnit 9 TestDavidNoch keine Bewertungen
- Drug Study RMCDokument3 SeitenDrug Study RMCNicolo Paulo TabiraraNoch keine Bewertungen
- Interferential Stimulation For The Treatment of Musculoskeletal PainDokument15 SeitenInterferential Stimulation For The Treatment of Musculoskeletal PainCTAFDocumentsNoch keine Bewertungen
- IAF MD 8 2011 Application of ISO 17011 in MDQMS (ISO 13485) Issue 1 2011Dokument17 SeitenIAF MD 8 2011 Application of ISO 17011 in MDQMS (ISO 13485) Issue 1 2011carlosprieto36Noch keine Bewertungen
- Prevention of Avoidable Blindness and Visual ImpairmentDokument3 SeitenPrevention of Avoidable Blindness and Visual ImpairmentAstidya MirantiNoch keine Bewertungen
- 7x Premature EjaculationDokument8 Seiten7x Premature EjaculationTer AbNoch keine Bewertungen
- Consciousness PsychologyDokument32 SeitenConsciousness PsychologyDeea Addine As-SoubNoch keine Bewertungen
- 2016 2017 VHSL Physical FormDokument4 Seiten2016 2017 VHSL Physical FormShreya IyerNoch keine Bewertungen
- Mood DisordersDokument1 SeiteMood DisordersTeresa MartinsNoch keine Bewertungen
- Act For Insomnia Act I by DR Guy Meadows The Sleep SchoolDokument7 SeitenAct For Insomnia Act I by DR Guy Meadows The Sleep SchoolDharmendra KumarNoch keine Bewertungen
- Fracasso - Energy Medicine 2010Dokument39 SeitenFracasso - Energy Medicine 2010api-308577129100% (1)
- Chapter 70-GuytonDokument9 SeitenChapter 70-Guytonswoljaswol1Noch keine Bewertungen
- EnglishDokument16 SeitenEnglishEugenius Divine LoveNoch keine Bewertungen
- Decup 2014Dokument8 SeitenDecup 2014Elija BrockNoch keine Bewertungen