Das könnte Ihnen auch gefallen
- 7.1 Summary of ContributionsDokument10 Seiten7.1 Summary of ContributionsHussainNoch keine Bewertungen
- Pulse Oximeter WirelessDokument6 SeitenPulse Oximeter WirelessJeanCarlos Chavarría HughesNoch keine Bewertungen
- Performance Evaluation of Healthcare Monitoring System Over Heterogeneous Wireless NetworksDokument10 SeitenPerformance Evaluation of Healthcare Monitoring System Over Heterogeneous Wireless NetworksRanjit KumarNoch keine Bewertungen
- Arduino Based Human Health Care Monitori PDFDokument10 SeitenArduino Based Human Health Care Monitori PDFAdriana OnticaNoch keine Bewertungen
- Ramsheeda.K: Guided By: MR - Sreekesh NamboodiriDokument27 SeitenRamsheeda.K: Guided By: MR - Sreekesh NamboodiriAsit PandaNoch keine Bewertungen
- Telemedicine SystemsDokument25 SeitenTelemedicine SystemsRohitash GuptaNoch keine Bewertungen
- Other SectionsDokument11 SeitenOther SectionsmmusfirNoch keine Bewertungen
- Survivable and Scalable Wireless Solution For E-Health and E-Emergency ApplicationsDokument5 SeitenSurvivable and Scalable Wireless Solution For E-Health and E-Emergency ApplicationskeerthiNoch keine Bewertungen
- Compressed Sensing Real-Time Energy-Eff Ecg Compression WBSN VandergheynstDokument11 SeitenCompressed Sensing Real-Time Energy-Eff Ecg Compression WBSN VandergheynstAlex WongNoch keine Bewertungen
- Wireless Body Area Networks SurveyedDokument18 SeitenWireless Body Area Networks Surveyedek9925Noch keine Bewertungen
- Networking Based Patient Monitoring System Project ReportDokument41 SeitenNetworking Based Patient Monitoring System Project ReportAbhishek Chandrakanth MugaliNoch keine Bewertungen
- Review Article: Wireless Body Area Networks For Healthcare Applications: Protocol Stack ReviewDokument24 SeitenReview Article: Wireless Body Area Networks For Healthcare Applications: Protocol Stack ReviewMargarita CuellarNoch keine Bewertungen
- Internet of Things IoT Based Real Time VDokument22 SeitenInternet of Things IoT Based Real Time VMd.Zesanul KabirNoch keine Bewertungen
- IoT Based Patient Health Monitoring SystemDokument4 SeitenIoT Based Patient Health Monitoring SystemAnonymous kw8Yrp0R5rNoch keine Bewertungen
- Optimized Congestion Management Protocol For HealthcareWireless Sensor NetworksDokument24 SeitenOptimized Congestion Management Protocol For HealthcareWireless Sensor Networksflmm09Noch keine Bewertungen
- An Intelligent and Power Efficient Biomedical Sensor Node For Wireless Cardiovascular Health MonitoringDokument12 SeitenAn Intelligent and Power Efficient Biomedical Sensor Node For Wireless Cardiovascular Health Monitoringsanjoy mondalNoch keine Bewertungen
- Mitigation of Channel Diversity and Indoor Channel Modeling For Remote Patient Monitoring SystemsDokument9 SeitenMitigation of Channel Diversity and Indoor Channel Modeling For Remote Patient Monitoring SystemsUbiquitous Computing and Communication JournalNoch keine Bewertungen
- Wireless Body Area Network Research PapersDokument6 SeitenWireless Body Area Network Research Paperslxeikcvnd100% (1)
- A Three-Tiered Architecture For Large-Scale Wireless Hospital Sensor NetworksDokument13 SeitenA Three-Tiered Architecture For Large-Scale Wireless Hospital Sensor NetworksThinh Tien NguyenNoch keine Bewertungen
- Unit-IV Healthcare: Sensor Networks in Healthcare, Use of Body Sensor Networks in Clinical Settings and Medical ResearchDokument111 SeitenUnit-IV Healthcare: Sensor Networks in Healthcare, Use of Body Sensor Networks in Clinical Settings and Medical ResearchAmith PNoch keine Bewertungen
- On The (In) Security of The Latest Generation Implantable Cardiac Defibrillators and How To Secure ThemDokument11 SeitenOn The (In) Security of The Latest Generation Implantable Cardiac Defibrillators and How To Secure ThemTom ChothiaNoch keine Bewertungen
- Wireless Sensor Networks: A Survey On The State of The Art and The 802.15.4 and Zigbee StandardsDokument41 SeitenWireless Sensor Networks: A Survey On The State of The Art and The 802.15.4 and Zigbee StandardsluckyboythongNoch keine Bewertungen
- Ubiquitous Real-Time Monitoring Critical-Care Patients Intensive Care UnitsDokument4 SeitenUbiquitous Real-Time Monitoring Critical-Care Patients Intensive Care Unitsnilanjan_chakravorttNoch keine Bewertungen
- Trust Key Management Scheme For Wireless Body Area NetworksDokument9 SeitenTrust Key Management Scheme For Wireless Body Area NetworksGeneration GenerationNoch keine Bewertungen
- 2 PatientDokument2 Seiten2 PatientJatin JacksNoch keine Bewertungen
- Patient Health Management System Using E-Health Monitoring ArchitectureDokument7 SeitenPatient Health Management System Using E-Health Monitoring Architecturejayesh tahasildarNoch keine Bewertungen
- Narrative Science: A ReviewDokument4 SeitenNarrative Science: A ReviewIjsrnet EditorialNoch keine Bewertungen
- BANs for Patient Health MonitoringDokument8 SeitenBANs for Patient Health MonitoringArnav GudduNoch keine Bewertungen
- Using Wireless Networks For Enhanced Monitoring of PatientsDokument9 SeitenUsing Wireless Networks For Enhanced Monitoring of PatientsPartho Kumar DuttaNoch keine Bewertungen
- RF and Microwave Technology Challenges For Internet-of-Things ApplicationsDokument2 SeitenRF and Microwave Technology Challenges For Internet-of-Things Applicationsmmk040891Noch keine Bewertungen
- (IJCST-V10I4P4) :kritika Yadav, Aanchal Gupta, Arun KumarDokument6 Seiten(IJCST-V10I4P4) :kritika Yadav, Aanchal Gupta, Arun KumarEighthSenseGroupNoch keine Bewertungen
- Personal Machine MachineDokument31 SeitenPersonal Machine MachineNikhil DixitNoch keine Bewertungen
- Body Area NetworkDokument15 SeitenBody Area NetworkxiaomingNoch keine Bewertungen
- projectt[1] 4th semDokument5 Seitenprojectt[1] 4th semSushmit SinghNoch keine Bewertungen
- projectt[1]_4th_sem[1]nnDokument6 Seitenprojectt[1]_4th_sem[1]nnSushmit SinghNoch keine Bewertungen
- Ding 2020Dokument14 SeitenDing 20200442- TARUNNoch keine Bewertungen
- Unit 2Dokument43 SeitenUnit 2Tilottama DeoreNoch keine Bewertungen
- WSN for Tracking Pilgrims at Tirupati FestivalDokument14 SeitenWSN for Tracking Pilgrims at Tirupati FestivalHaley HaleNoch keine Bewertungen
- 1312 - BDD Tdma Mac - JBMDokument11 Seiten1312 - BDD Tdma Mac - JBMTola AlegbeleyeNoch keine Bewertungen
- UntitledDokument10 SeitenUntitledkamnamishra1203Noch keine Bewertungen
- Real-Time Heart Pulse Monitoring Technique Using WDokument9 SeitenReal-Time Heart Pulse Monitoring Technique Using WAndreea IlieNoch keine Bewertungen
- Fog Computing in Healthcare Internet-of-Things: A Case Study On ECG Feature ExtractionDokument8 SeitenFog Computing in Healthcare Internet-of-Things: A Case Study On ECG Feature ExtractionCibyBaby PunnamparambilNoch keine Bewertungen
- Privacy Protection For Wireless Medical Sensor DataDokument14 SeitenPrivacy Protection For Wireless Medical Sensor DataSiddharth RamrakhianiNoch keine Bewertungen
- 5N13 IJESET0603123 v6 Iss3 316 3ijeset23Dokument8 Seiten5N13 IJESET0603123 v6 Iss3 316 3ijeset23parthasarathycseNoch keine Bewertungen
- A Framework For Intelligent Sensor Network With Video Camera For Structural Health Monitoring of BridgesDokument5 SeitenA Framework For Intelligent Sensor Network With Video Camera For Structural Health Monitoring of BridgesAnusha Kommineni100% (1)
- Health Monitoring SystemDokument8 SeitenHealth Monitoring SystemElizabeth HarrisNoch keine Bewertungen
- Intelligent Health Vessel ABC-DE An Electrocardiogram Cloud Computing ServiceDokument14 SeitenIntelligent Health Vessel ABC-DE An Electrocardiogram Cloud Computing ServiceNexgen TechnologyNoch keine Bewertungen
- Smart Patient Monitoring System Using WSN & AndroidDokument6 SeitenSmart Patient Monitoring System Using WSN & AndroidEditor IJRITCC0% (1)
- PATIENT MONTEXT MONITORING USING WIRELESS SENSORSDokument10 SeitenPATIENT MONTEXT MONITORING USING WIRELESS SENSORSsatish kumarNoch keine Bewertungen
- Advanced Patient or Elder Fall Detection Based On Movement and Sound DataDokument5 SeitenAdvanced Patient or Elder Fall Detection Based On Movement and Sound DataHitesh ವಿಟ್ಟಲ್ ShettyNoch keine Bewertungen
- WSN Home HealthcareDokument4 SeitenWSN Home Healthcarekichan992Noch keine Bewertungen
- 1.1. Wireless Sensor NetworksDokument19 Seiten1.1. Wireless Sensor NetworksTechnos_IncNoch keine Bewertungen
- IJSRET V5 Issue1 124Dokument7 SeitenIJSRET V5 Issue1 124Arthee PandiNoch keine Bewertungen
- Wireless Medical Sensor Networks IEEE PROJECTDokument15 SeitenWireless Medical Sensor Networks IEEE PROJECTKumar SatyamNoch keine Bewertungen
- Example For Mobile ECG Holter Design Using FMEA ModelDokument3 SeitenExample For Mobile ECG Holter Design Using FMEA ModelAudy FakhrinoorNoch keine Bewertungen
- Design Open Source Remote ECG Service Under 40 CharactersDokument19 SeitenDesign Open Source Remote ECG Service Under 40 Charactersmuhamad ilhamNoch keine Bewertungen
- Abstract: Patients at Disaster Scenes Can Greatly Benefit From Technologies That ContinuouslyDokument6 SeitenAbstract: Patients at Disaster Scenes Can Greatly Benefit From Technologies That ContinuouslyBhuwan ShresthaNoch keine Bewertungen
- Power Harvesting, Dynamic and Reliable Green Wireless Body Area Networks For Health Care ApplicationsDokument4 SeitenPower Harvesting, Dynamic and Reliable Green Wireless Body Area Networks For Health Care ApplicationsChrys StinsonNoch keine Bewertungen
- Trustworthy Data Collection From Implantable Medical Devices Via High-Speed Security Implementation Based On IEEE 1363Dokument8 SeitenTrustworthy Data Collection From Implantable Medical Devices Via High-Speed Security Implementation Based On IEEE 1363Navaneeth PurushothamanNoch keine Bewertungen
- Body Area Networks using IEEE 802.15.6: Implementing the ultra wide band physical layerVon EverandBody Area Networks using IEEE 802.15.6: Implementing the ultra wide band physical layerNoch keine Bewertungen
- ALU LTE LB WorkshopDokument47 SeitenALU LTE LB WorkshopBelieverNoch keine Bewertungen
- Grila Programe (Digitala) Next GenDokument1 SeiteGrila Programe (Digitala) Next GenMarius MihailaNoch keine Bewertungen
- Toshiba Satellite A300Dokument37 SeitenToshiba Satellite A300Nagy József100% (1)
- AirLive POE-100CAMv2 ManualDokument138 SeitenAirLive POE-100CAMv2 Manualsi1viu1Noch keine Bewertungen
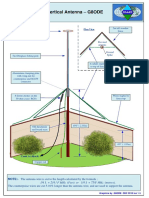
- 20m Elevated Vertical Antenna DesignDokument5 Seiten20m Elevated Vertical Antenna Designleonardo_manzanoNoch keine Bewertungen
- Homebrew 6SN7 QRP Transmitters Using Recycled MaterialsDokument7 SeitenHomebrew 6SN7 QRP Transmitters Using Recycled MaterialsavpanubisNoch keine Bewertungen
- Network Planning and DimensioningDokument26 SeitenNetwork Planning and DimensioningOvalNoch keine Bewertungen
- 09 TV 040 R 19Dokument3 Seiten09 TV 040 R 19Umut ErdenayNoch keine Bewertungen
- Mikrotik PDFDokument337 SeitenMikrotik PDFdika8Noch keine Bewertungen
- Remote Commander: EnglishDokument2 SeitenRemote Commander: EnglishJavier MontoyaNoch keine Bewertungen
- XP530A - 2015 - Service - Manual - 2PW-28197-10 (1) (432-437)Dokument6 SeitenXP530A - 2015 - Service - Manual - 2PW-28197-10 (1) (432-437)Zaki ZakiNoch keine Bewertungen
- CCNP Route All ChaptersDokument66 SeitenCCNP Route All ChaptersRobertNoch keine Bewertungen
- UMTS Link Budget Basic ParameterDokument7 SeitenUMTS Link Budget Basic ParameterexcaliburslvNoch keine Bewertungen
- 3eeecn 20190820070656Dokument2 Seiten3eeecn 20190820070656atara sindiNoch keine Bewertungen
- YAG12 - Antena JammerDokument1 SeiteYAG12 - Antena JammeruserdsrNoch keine Bewertungen
- Eccm in RadarsDokument89 SeitenEccm in Radarsnaivedya_mishraNoch keine Bewertungen
- Kathrein 800 10426Dokument2 SeitenKathrein 800 10426PavelKuzovkinNoch keine Bewertungen
- 1 AMC CANopenCommunicationManualDokument313 Seiten1 AMC CANopenCommunicationManualmaxellligue5487Noch keine Bewertungen
- Enterprise Networking AssignmentDokument19 SeitenEnterprise Networking AssignmentHarris NantikwaNoch keine Bewertungen
- User Manual RUTX09 EN-v1.1Dokument11 SeitenUser Manual RUTX09 EN-v1.1GuilhermeDeOliveiraSantosNoch keine Bewertungen
- Bovpn OSPF For Distributed Enterprise Example (En-Us)Dokument42 SeitenBovpn OSPF For Distributed Enterprise Example (En-Us)WilberRiveroOduberNoch keine Bewertungen
- MobilinkDokument39 SeitenMobilinkParas ShahabNoch keine Bewertungen
- History of the Internet in the Philippines: Milestones from 1986-1994Dokument2 SeitenHistory of the Internet in the Philippines: Milestones from 1986-1994Lloyd CruzNoch keine Bewertungen
- Seminar Report On DaknetDokument53 SeitenSeminar Report On Daknetmundravijay100% (3)
- IPCam Use GuideDokument18 SeitenIPCam Use GuidechiuhereNoch keine Bewertungen
- Manual Del Seminario LCD HD PDFDokument32 SeitenManual Del Seminario LCD HD PDFca_otiNoch keine Bewertungen
- ZXA10 C600 (V1.0) xPON System IntroductionDokument54 SeitenZXA10 C600 (V1.0) xPON System IntroductionDrone Semarang100% (3)
- 1500R Maintenance and TroubleshootingDokument24 Seiten1500R Maintenance and TroubleshootingKaushal DarjiNoch keine Bewertungen
- ST7735 V2.1 20100505Dokument167 SeitenST7735 V2.1 20100505AraoFilhoNoch keine Bewertungen
- IPTV Architecture and SolutionDokument24 SeitenIPTV Architecture and SolutionPeter ChenNoch keine Bewertungen
































![projectt[1] 4th sem](https://imgv2-2-f.scribdassets.com/img/document/722841972/149x198/0ac077f221/1713082758?v=1)
![projectt[1]_4th_sem[1]nn](https://imgv2-1-f.scribdassets.com/img/document/722841973/149x198/4afbadc431/1713082771?v=1)