Das könnte Ihnen auch gefallen
- Autoimmune Protocol Ebook 6 19Dokument306 SeitenAutoimmune Protocol Ebook 6 19Hrvoje100% (12)
- Standards of Care in Diabetes - 2024Dokument9 SeitenStandards of Care in Diabetes - 2024josueraulbalandranNoch keine Bewertungen
- Passive Leg RaisingDokument11 SeitenPassive Leg Raisingnaufal12345Noch keine Bewertungen
- VPP y Vvci en Sepsis-2016Dokument20 SeitenVPP y Vvci en Sepsis-2016Elsa AivarNoch keine Bewertungen
- Fluid Response Evaluation in Sepsis Hypotension and Shock A Randomized Clinical TrialDokument15 SeitenFluid Response Evaluation in Sepsis Hypotension and Shock A Randomized Clinical TrialntnquynhproNoch keine Bewertungen
- Bakker-2016-Intensive Care MedicineDokument3 SeitenBakker-2016-Intensive Care MedicineBiancaPancuNoch keine Bewertungen
- Stroke Volume Variation For Prediction of Fluid Responsiveness in Patients Undergoing Gastrointestinal SurgeryDokument8 SeitenStroke Volume Variation For Prediction of Fluid Responsiveness in Patients Undergoing Gastrointestinal SurgeryossinNoch keine Bewertungen
- Assessing Volume StatusDokument12 SeitenAssessing Volume StatusMoises Torres AlvarezNoch keine Bewertungen
- Passive Leg Raising-Induced Changes in Pulse Pressure Variation To Assess Fluid Responsiveness in Mechanically Ventilated Patients - A Multicentre Prospective Observational StudyDokument9 SeitenPassive Leg Raising-Induced Changes in Pulse Pressure Variation To Assess Fluid Responsiveness in Mechanically Ventilated Patients - A Multicentre Prospective Observational Studycardionerd101Noch keine Bewertungen
- Passive Leg Raising and Fluid Responsiveness Monnet CCM 2006Dokument6 SeitenPassive Leg Raising and Fluid Responsiveness Monnet CCM 2006Leiniker Navarro ReyNoch keine Bewertungen
- Contin Educ Anaesth Crit Care Pain-2010-Eyre-59-62Dokument4 SeitenContin Educ Anaesth Crit Care Pain-2010-Eyre-59-62deadbysunriseeNoch keine Bewertungen
- Critical Apraisal: Posisi Telungkup Secara Signifikan Mengurangi Angka Kematian Dibandingkan Dengan Posisi TelentangDokument9 SeitenCritical Apraisal: Posisi Telungkup Secara Signifikan Mengurangi Angka Kematian Dibandingkan Dengan Posisi TelentangRiakan MangkaNoch keine Bewertungen
- Review Article: de Fining Fluid Responsiveness: A Guide To Patient-Tailored Volume TitrationDokument10 SeitenReview Article: de Fining Fluid Responsiveness: A Guide To Patient-Tailored Volume TitrationmarceloNoch keine Bewertungen
- 2010 Rev Monitor PiCCO Int Anest JDokument29 Seiten2010 Rev Monitor PiCCO Int Anest JCarlos PalominoNoch keine Bewertungen
- The PiCCO MonitorDokument29 SeitenThe PiCCO MonitorClaudia IsabelNoch keine Bewertungen
- Am J Crit Care 2012 Halm 449 52Dokument5 SeitenAm J Crit Care 2012 Halm 449 52Fikri Ulil AlbabNoch keine Bewertungen
- Metanalisis Elevacion Pasiva de MMIIDokument11 SeitenMetanalisis Elevacion Pasiva de MMIImayraNoch keine Bewertungen
- Abdominal TraumaDokument60 SeitenAbdominal Traumamel_chakNoch keine Bewertungen
- Uso de Parámetros Estáticos y Dinámicos Antes de Expansión Fluidos-2016Dokument21 SeitenUso de Parámetros Estáticos y Dinámicos Antes de Expansión Fluidos-2016Elsa AivarNoch keine Bewertungen
- Abdominal TraumaDokument60 SeitenAbdominal Traumaapi-19916399Noch keine Bewertungen
- Haemodynamic MonitoringDokument6 SeitenHaemodynamic MonitoringAnusha Verghese100% (1)
- S. 14.0 Fluid Therapy - Trauma CasesDokument7 SeitenS. 14.0 Fluid Therapy - Trauma CasesroropujiNoch keine Bewertungen
- Hemodynamic Assessment in The Contemporary ICUDokument33 SeitenHemodynamic Assessment in The Contemporary ICUnacxit6Noch keine Bewertungen
- CC 9070Dokument15 SeitenCC 9070ossinNoch keine Bewertungen
- Hypovolemic Shock ResuscitationDokument21 SeitenHypovolemic Shock ResuscitationM Lutfi FananiNoch keine Bewertungen
- Vti Carotideo RevisarDokument9 SeitenVti Carotideo RevisarCurro MirallesNoch keine Bewertungen
- Bedside Hemodynamic MonitoringDokument26 SeitenBedside Hemodynamic MonitoringBrad F LeeNoch keine Bewertungen
- Summary and ConclusionDokument4 SeitenSummary and Conclusionhamodi222Noch keine Bewertungen
- Fluid Management in HFDokument47 SeitenFluid Management in HFPandu AnggoroNoch keine Bewertungen
- I - PAV+ Clinical Summary - Georgopoulos Et AlDokument2 SeitenI - PAV+ Clinical Summary - Georgopoulos Et AlJuan Genaro Martinez PeñaNoch keine Bewertungen
- University of South Wales Open Access RepositoryDokument20 SeitenUniversity of South Wales Open Access RepositoryAnastasia Dewi AprillaNoch keine Bewertungen
- Barjaktarevic 2018Dokument7 SeitenBarjaktarevic 2018Moni-k GuarnerosNoch keine Bewertungen
- Journal ReadingDokument17 SeitenJournal ReadingRhyka AchmadNoch keine Bewertungen
- How To Avoid Flud OverloadDokument7 SeitenHow To Avoid Flud OverloadEward Rod SalNoch keine Bewertungen
- Elia Jennifer Perioperative Fluid Management andDokument19 SeitenElia Jennifer Perioperative Fluid Management andSiddhartha PalaciosNoch keine Bewertungen
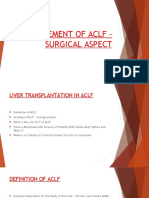
- Management of AclfDokument30 SeitenManagement of Aclfsaraswathy sNoch keine Bewertungen
- AnemiaDokument10 SeitenAnemiaRamesh VaradharajanNoch keine Bewertungen
- 1 s2.0 S1053077019303039 MainDokument6 Seiten1 s2.0 S1053077019303039 MainADELIAADENoch keine Bewertungen
- Gtcicyrcp Como Valorar La Respuesta A Volumen en La UciDokument18 SeitenGtcicyrcp Como Valorar La Respuesta A Volumen en La UciConny SaldiviaNoch keine Bewertungen
- Pre and Post Operative Care: To: DR - Biniyam. By: Biniam.MDokument56 SeitenPre and Post Operative Care: To: DR - Biniyam. By: Biniam.MBini JaminNoch keine Bewertungen
- Detection, Evaluation, and Management of Preoperative Anaemia in The Elective Orthopaedic Surgical Patient: NATA GuidelinesDokument10 SeitenDetection, Evaluation, and Management of Preoperative Anaemia in The Elective Orthopaedic Surgical Patient: NATA GuidelinesDiego Martin RabasedasNoch keine Bewertungen
- Respiratory - ARDS Vent Revised - QuestionsDokument6 SeitenRespiratory - ARDS Vent Revised - QuestionsRyan ReNoch keine Bewertungen
- Presented By: Ima Sulistiyo RDokument18 SeitenPresented By: Ima Sulistiyo RjackytungadiNoch keine Bewertungen
- HỒI SỨC DỊCHDokument15 SeitenHỒI SỨC DỊCHTrần Huỳnh Lan AnhNoch keine Bewertungen
- Polypharmacy in Patients Hospitalised For Acute Exacerbation of COPDDokument4 SeitenPolypharmacy in Patients Hospitalised For Acute Exacerbation of COPDpina distefanoNoch keine Bewertungen
- CLN 66 01 107 PDFDokument5 SeitenCLN 66 01 107 PDFGloria KartikaNoch keine Bewertungen
- RCT of Aprv Vs LPV in Ards PtsDokument11 SeitenRCT of Aprv Vs LPV in Ards PtsOldriana Prawiro HapsariNoch keine Bewertungen
- Prediction of Fluid ResponsivenessDokument4 SeitenPrediction of Fluid ResponsivenessSANTOSH KUMAR BHASKARNoch keine Bewertungen
- AppendicitisDokument11 SeitenAppendicitisWildan Farik AlkafNoch keine Bewertungen
- Thesis B LansdorpDokument244 SeitenThesis B LansdorpRizkaNoch keine Bewertungen
- Roberts2015 PDFDokument11 SeitenRoberts2015 PDFJeff LapianNoch keine Bewertungen
- Pulmonary Function TestDokument7 SeitenPulmonary Function TestGhada HusseinNoch keine Bewertungen
- Test Questions - Gastrointestinal Bleeding: QUESTION 1. The Most Frequent Cause of UGI Bleeding IsDokument40 SeitenTest Questions - Gastrointestinal Bleeding: QUESTION 1. The Most Frequent Cause of UGI Bleeding IsAtik ShaikhNoch keine Bewertungen
- Contemporary Perioperative Haemodynamic MonitoringDokument12 SeitenContemporary Perioperative Haemodynamic MonitoringrjerezrNoch keine Bewertungen
- AdsasdadsaDokument252 SeitenAdsasdadsaAmitShettyNoch keine Bewertungen
- Percutaneous Mitral Valvuloplasty Versus Perawatan Bedah Di Mitral Stenosis Dengan Berat Trikuspid RegurgitasiDokument6 SeitenPercutaneous Mitral Valvuloplasty Versus Perawatan Bedah Di Mitral Stenosis Dengan Berat Trikuspid Regurgitasiikbal rambalinoNoch keine Bewertungen
- Treatment of Steal SyndromeDokument16 SeitenTreatment of Steal SyndromeStevent RichardoNoch keine Bewertungen
- Noninvasive Monitoring 2016Dokument6 SeitenNoninvasive Monitoring 2016Maria LaiaNoch keine Bewertungen
- Clinical Review: Hemodynamic Monitoring in The Intensive Care UnitDokument8 SeitenClinical Review: Hemodynamic Monitoring in The Intensive Care Unitmasfak97Noch keine Bewertungen
- Apm 23072Dokument11 SeitenApm 23072Lucas SCaNoch keine Bewertungen
- Haematemesis and MalenaDokument39 SeitenHaematemesis and MalenaNikNoch keine Bewertungen
- Essentials in Lung TransplantationVon EverandEssentials in Lung TransplantationAllan R. GlanvilleNoch keine Bewertungen
- Intern TicklerDokument10 SeitenIntern TicklerRem AlfelorNoch keine Bewertungen
- Practice Template Red FlagsDokument32 SeitenPractice Template Red FlagsAngelaNoch keine Bewertungen
- Circular Regarding Opening of School For Class X & XII - Aug 2021Dokument2 SeitenCircular Regarding Opening of School For Class X & XII - Aug 2021Shubhangi PriyaNoch keine Bewertungen
- BIU Clinic FormsDokument4 SeitenBIU Clinic FormsMarvellous AbrahamNoch keine Bewertungen
- Igg4-Related Disease: A Reminder For Practicing PathologistsDokument8 SeitenIgg4-Related Disease: A Reminder For Practicing PathologistsMariela Judith UCNoch keine Bewertungen
- Tto QX Metastasis Cerebrales PDFDokument8 SeitenTto QX Metastasis Cerebrales PDFmilagro meza poloNoch keine Bewertungen
- Tongue DisordersDokument10 SeitenTongue DisordersMohan VeerabomalaNoch keine Bewertungen
- Writers Cramp - A Major Conundrum: Review Article44Dokument7 SeitenWriters Cramp - A Major Conundrum: Review Article44IJAR JOURNALNoch keine Bewertungen
- Pengobatan Kanker, Manajemen Nyeri, Dan Terapi PaliatifDokument31 SeitenPengobatan Kanker, Manajemen Nyeri, Dan Terapi PaliatifasihNoch keine Bewertungen
- HDU AuditDokument3 SeitenHDU AuditAsdf DgfhgNoch keine Bewertungen
- Biosecurity Sample PlanDokument56 SeitenBiosecurity Sample PlanAlvin Lee Cucio AsuroNoch keine Bewertungen
- Presentation On WalnutDokument5 SeitenPresentation On WalnutSheikh JeelaniNoch keine Bewertungen
- Doh DC 2018-0142Dokument2 SeitenDoh DC 2018-0142vanceNoch keine Bewertungen
- Reviewer For OediaDokument19 SeitenReviewer For Oedias9crhvrymhNoch keine Bewertungen
- IMCIDokument2 SeitenIMCIsweet_lily_valleyNoch keine Bewertungen
- Pengembangan Aplikasi Monitoring Penyakit Hipertensi Dan Diabetes Mellitus TerintegrasiDokument15 SeitenPengembangan Aplikasi Monitoring Penyakit Hipertensi Dan Diabetes Mellitus TerintegrasiberiNoch keine Bewertungen
- AUH Travel Declaration FormDokument2 SeitenAUH Travel Declaration FormAbdul RahmanNoch keine Bewertungen
- Covid-19 Test Report: Dr. Babasaheb Ambedkar Marathwada University, Sub Campus, OsmanabadDokument1 SeiteCovid-19 Test Report: Dr. Babasaheb Ambedkar Marathwada University, Sub Campus, OsmanabadNaren JamadarNoch keine Bewertungen
- Uji Reliabilitas Brief Peripheral NeuropathyDokument7 SeitenUji Reliabilitas Brief Peripheral NeuropathyfauzihidayatNoch keine Bewertungen
- Assignment 4: Measures of Disease Frequency: Unit 1 - Basic Course in Biomedical Research: Cycle 2 (Mar-Jun 2020)Dokument6 SeitenAssignment 4: Measures of Disease Frequency: Unit 1 - Basic Course in Biomedical Research: Cycle 2 (Mar-Jun 2020)stNoch keine Bewertungen
- Ataxia TelangiectasiaDokument2 SeitenAtaxia TelangiectasiaCS NarayananNoch keine Bewertungen
- SkripsiDokument78 SeitenSkripsiAdimas DewanggaNoch keine Bewertungen
- JURNAL Irma Rangkuti Dan Sisilmonalisa 1Dokument14 SeitenJURNAL Irma Rangkuti Dan Sisilmonalisa 1Khairani PutriNoch keine Bewertungen
- Nail DisorderDokument25 SeitenNail DisorderCherry Lou RaboyNoch keine Bewertungen
- Communicable Disease Chart Rev 3 06Dokument3 SeitenCommunicable Disease Chart Rev 3 06Margarrette RicoteNoch keine Bewertungen
- Behcet's Disease (Adamantiades Syndrome) : DefinitionDokument9 SeitenBehcet's Disease (Adamantiades Syndrome) : DefinitionNuzairah AynoorNoch keine Bewertungen
- Typhoid Fever: Presented by Sharlin MacalintalDokument18 SeitenTyphoid Fever: Presented by Sharlin MacalintalPaul JacksonNoch keine Bewertungen
- Coronavirus Disease (COVID-19) : Case Investigation FormDokument2 SeitenCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNoch keine Bewertungen