Das könnte Ihnen auch gefallen
- Clin Pharm Lile Antibacterial Classes and ExamplesDokument4 SeitenClin Pharm Lile Antibacterial Classes and ExamplesNicole BerryNoch keine Bewertungen
- Treatment guidelines for common infectionsDokument1 SeiteTreatment guidelines for common infectionsJoseph De JoyaNoch keine Bewertungen
- Infectious Diseases IDokument7 SeitenInfectious Diseases ITiff VoNoch keine Bewertungen
- Beta Lactam AntibioticsDokument1 SeiteBeta Lactam AntibioticsCourtney TownsendNoch keine Bewertungen
- Antibiotics ChartDokument10 SeitenAntibiotics Chartadom09Noch keine Bewertungen
- Antibiotics Chart 2Dokument10 SeitenAntibiotics Chart 2Vee MendNoch keine Bewertungen
- AntimicrobialsDokument1 SeiteAntimicrobialsRomaine Barrett100% (1)
- Antibiotic Summary - DraftDokument10 SeitenAntibiotic Summary - DraftStrept Pneumonia100% (1)
- AntibioticsDokument6 SeitenAntibioticsOccamsRazor100% (1)
- Antibiotics Summary - Flattened PDFDokument3 SeitenAntibiotics Summary - Flattened PDFmicheal1960100% (6)
- Pharm Drug ListDokument17 SeitenPharm Drug Listanon_523534678Noch keine Bewertungen
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Dokument48 SeitenNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanNoch keine Bewertungen
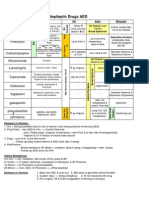
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDokument1 SeiteAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Noch keine Bewertungen
- Antibiotics 9Dokument11 SeitenAntibiotics 9Beth Morales100% (1)
- Drug Interactions 2 Paper PDFDokument2 SeitenDrug Interactions 2 Paper PDFAzima AbdelrhamanNoch keine Bewertungen
- Bumetanide Torsemide: Desmopressin - V2Dokument1 SeiteBumetanide Torsemide: Desmopressin - V2med testNoch keine Bewertungen
- Antibiotic Classification & Indications OverviewDokument16 SeitenAntibiotic Classification & Indications Overviewdaven100% (1)
- Respiratory and Cardiovascular DrugsDokument4 SeitenRespiratory and Cardiovascular DrugsNurse HoomanNoch keine Bewertungen
- AB ClassesDokument4 SeitenAB Classesrayooona88100% (2)
- Mu 002Dokument10 SeitenMu 002chandanNoch keine Bewertungen
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDokument16 SeitenThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- Antibiotic GuideDokument6 SeitenAntibiotic GuideAnnTran100% (1)
- Introduction to commonly used antibioticsDokument2 SeitenIntroduction to commonly used antibioticsAmir AmirulNoch keine Bewertungen
- Cell Wall Inhibitors and Protein Synthesis Inhibitors Antibiotics Mechanisms of ActionDokument3 SeitenCell Wall Inhibitors and Protein Synthesis Inhibitors Antibiotics Mechanisms of Actionyanks1120Noch keine Bewertungen
- SuperDrugs! Simon's Short Drug SummaryDokument5 SeitenSuperDrugs! Simon's Short Drug Summarybriancripe100% (2)
- Drug of Choice List PDFDokument2 SeitenDrug of Choice List PDFHeceas Heceas0% (1)
- A.1. Community-Acquired: Use Antibiotics JudiciouslyDokument33 SeitenA.1. Community-Acquired: Use Antibiotics JudiciouslymaxgroovesNoch keine Bewertungen
- Top-200-Drug ETSYDokument31 SeitenTop-200-Drug ETSYBetsy Brown ByersmithNoch keine Bewertungen
- Pharma ChartsDokument33 SeitenPharma ChartsNooreen Hussain100% (1)
- Chart Antibacterial Drugs PDFDokument1 SeiteChart Antibacterial Drugs PDFMunaf AlsumaryNoch keine Bewertungen
- Review Handouts For Medical Pharmacology PDFDokument21 SeitenReview Handouts For Medical Pharmacology PDFAndres F. TorresNoch keine Bewertungen
- UWorld - Psych Review Charts (From Questions)Dokument47 SeitenUWorld - Psych Review Charts (From Questions)uowhywxuuiragjadchNoch keine Bewertungen
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDokument18 SeitenPharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- Brand Generic Class Other: NAPLEX ReviewDokument72 SeitenBrand Generic Class Other: NAPLEX Reviewbapimirab654Noch keine Bewertungen
- NSAIDS and SteroidsDokument2 SeitenNSAIDS and Steroidsmed testNoch keine Bewertungen
- Diabetes Mellitus Drug ChartDokument3 SeitenDiabetes Mellitus Drug Chartlui.stephanie1751100% (1)
- List of antibiotics: generic names, brands, classes and usesDokument9 SeitenList of antibiotics: generic names, brands, classes and usesprince1500100% (1)
- SJDWHDJSDJSDDokument358 SeitenSJDWHDJSDJSDwide mind hackerNoch keine Bewertungen
- Chemotherapy NDokument28 SeitenChemotherapy NFaisal MehboobNoch keine Bewertungen
- Vancomycin Pharmacology Indications, Mechanism, and Side Effects! PDFDokument1 SeiteVancomycin Pharmacology Indications, Mechanism, and Side Effects! PDFFrancis PasayNoch keine Bewertungen
- Pharm Drug Outline AdrDokument1 SeitePharm Drug Outline AdrCess Lagera YbanezNoch keine Bewertungen
- Common Medications UsedDokument3 SeitenCommon Medications UsedRay Michael CasupananNoch keine Bewertungen
- Antibacterial Drugs SummaryDokument13 SeitenAntibacterial Drugs SummaryNeo Ramagaga100% (1)
- A-Autonomic Drugs: 1) CholinergicDokument28 SeitenA-Autonomic Drugs: 1) CholinergicMahmoud Ahmed MahmoudNoch keine Bewertungen
- Top 300 Drugs Pocket Reference Guide (2021 Edition)Von EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Bewertung: 5 von 5 Sternen5/5 (1)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesVon EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesBewertung: 4 von 5 Sternen4/5 (2)
- Bacterial Infectious Diseases Empiric TherapyDokument17 SeitenBacterial Infectious Diseases Empiric Therapykaylakmills_10135868Noch keine Bewertungen
- SKINDokument2 SeitenSKINKassem HijazyNoch keine Bewertungen
- Infectious Disease - Antibiotic Ladder PDFDokument2 SeitenInfectious Disease - Antibiotic Ladder PDFVaishali PrasharNoch keine Bewertungen
- Antiobitic Infection TX ChartDokument8 SeitenAntiobitic Infection TX ChartTLNoch keine Bewertungen
- Drugs For BacteriaDokument4 SeitenDrugs For BacteriaShabd SANoch keine Bewertungen
- PRINCIPLES OF ANTIBIOTIC SELECTION FOR COMMON INFECTIONSDokument2 SeitenPRINCIPLES OF ANTIBIOTIC SELECTION FOR COMMON INFECTIONSYukiC123Noch keine Bewertungen
- Antibiotic PrescribingDokument1 SeiteAntibiotic PrescribingJay KayNoch keine Bewertungen
- Antibiotics of ChoiceDokument6 SeitenAntibiotics of ChoiceTunas AndriantoNoch keine Bewertungen
- PDF Antibiotic Prescribing - CompressDokument1 SeitePDF Antibiotic Prescribing - CompressMaximilian BezzeghNoch keine Bewertungen
- Pneumonia - Spread SheetDokument1 SeitePneumonia - Spread SheetRobin KeaneNoch keine Bewertungen
- FinalDokument3 SeitenFinalMihalache TiberiuNoch keine Bewertungen
- 1-Co - Trimoxazol: AntibioticsDokument66 Seiten1-Co - Trimoxazol: Antibioticsmohamed mahmoudNoch keine Bewertungen
- 1a Antiinfective DrugsDokument4 Seiten1a Antiinfective DrugsMaria Donabella OngueNoch keine Bewertungen
- Im Dude HandoutDokument1 SeiteIm Dude Handoutapi-535001113Noch keine Bewertungen
- HIV and Its TreatmentDokument24 SeitenHIV and Its Treatmentaathira_kNoch keine Bewertungen
- CNS Drugs OverviewDokument42 SeitenCNS Drugs OverviewJessica Esper EmbresciaNoch keine Bewertungen
- Nevirapine Drug .Dokument11 SeitenNevirapine Drug .AminaNoch keine Bewertungen
- Pharm U WorldDokument421 SeitenPharm U Worldjonathan100% (8)
- 13 AntibioticsAntiRetroviralsAIDS PDFDokument90 Seiten13 AntibioticsAntiRetroviralsAIDS PDFjenniferluzonNoch keine Bewertungen
- Volume 42, Issue 48 - December 2, 2011Dokument64 SeitenVolume 42, Issue 48 - December 2, 2011BladeNoch keine Bewertungen
- 1-Antivirals Medicinal ChemistryDokument20 Seiten1-Antivirals Medicinal ChemistryBasil Domi0% (1)
- National Comprehensive HIV Prevention, Care, and Treatment Training For Pharmacy Professionals-Participant ManualDokument326 SeitenNational Comprehensive HIV Prevention, Care, and Treatment Training For Pharmacy Professionals-Participant ManualAYANA KORSANoch keine Bewertungen
- ARV Guidline PDFDokument12 SeitenARV Guidline PDFEndah Sri IsmayawatiNoch keine Bewertungen
- HIV Treatment and Prevention 2019: Current Standards of CareDokument9 SeitenHIV Treatment and Prevention 2019: Current Standards of Careputri vinia /ilove cuteNoch keine Bewertungen
- Discovery and Development of Nucleoside and Nucleotide Reverse-Transcriptase InhibitorsDokument8 SeitenDiscovery and Development of Nucleoside and Nucleotide Reverse-Transcriptase Inhibitorsolivia523Noch keine Bewertungen
- Pathophysiology: HIV Infection and AIDSDokument7 SeitenPathophysiology: HIV Infection and AIDSmeylin SNoch keine Bewertungen
- Are Viruses Living or Non-Living Organisms?Dokument8 SeitenAre Viruses Living or Non-Living Organisms?Sydney Cloyce NagalNoch keine Bewertungen
- Virus & Antiviral Drugs: Prof. Dr. Ishrat ImranDokument57 SeitenVirus & Antiviral Drugs: Prof. Dr. Ishrat Imransomi shaikh100% (1)
- Antiviral DrugsDokument14 SeitenAntiviral DrugsSunil100% (4)
- Lab Requisition SampleDokument1 SeiteLab Requisition SampleUser SmuggNoch keine Bewertungen
- HIV Medication Chart - Jan 2019Dokument2 SeitenHIV Medication Chart - Jan 2019Stephany SoutoNoch keine Bewertungen
- Patrick Ch17Dokument49 SeitenPatrick Ch17Caroline Lessa0% (1)
- Immunodeficiency DisordersDokument8 SeitenImmunodeficiency Disordersbpt2Noch keine Bewertungen
- Kuliah Farmakologi - Farmakokinetik Dan Farmakodinamik Antivirus Dan Antiparasit Secara UmumDokument87 SeitenKuliah Farmakologi - Farmakokinetik Dan Farmakodinamik Antivirus Dan Antiparasit Secara UmumGabriel AnindhitaNoch keine Bewertungen
- ANTIVIRAL DRUGS MOA AND MAJOR CLASSESDokument21 SeitenANTIVIRAL DRUGS MOA AND MAJOR CLASSESRex Karl TeoxonNoch keine Bewertungen
- Antiviral Drugs: Mechanisms and Treatment OptionsDokument35 SeitenAntiviral Drugs: Mechanisms and Treatment Optionsjustin rodrigoNoch keine Bewertungen
- National AIDS Control ProgramDokument29 SeitenNational AIDS Control ProgramMonalisha SinghNoch keine Bewertungen
- Chapter 10Dokument45 SeitenChapter 10Hannah BuquironNoch keine Bewertungen
- HIV & TBDokument51 SeitenHIV & TBRhea DerijeNoch keine Bewertungen
- Antibiotic Mcqs June 04Dokument6 SeitenAntibiotic Mcqs June 04Mirza GhalibNoch keine Bewertungen
- Keto LogDokument7 SeitenKeto LogKim Justin InfantadoNoch keine Bewertungen
- Hiv/Aids Stadium Iii With Opportunistic Infection: (Laporan Kasus)Dokument4 SeitenHiv/Aids Stadium Iii With Opportunistic Infection: (Laporan Kasus)yantiNoch keine Bewertungen
- Biopharm - MidtermDokument4 SeitenBiopharm - MidtermLinhNguyeNoch keine Bewertungen
- Influenza virus NA inhibitors block the viral neuraminidase enzyme, so resistance would involve amino acid changes in that enzyme. The correct answer is 1Dokument61 SeitenInfluenza virus NA inhibitors block the viral neuraminidase enzyme, so resistance would involve amino acid changes in that enzyme. The correct answer is 1Alen MehovicNoch keine Bewertungen