Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- 3 Facial Exercises To Get Rid of Sagging Jowls - Face YogaDokument5 Seiten3 Facial Exercises To Get Rid of Sagging Jowls - Face YogabazediNoch keine Bewertungen
- Hidden Meanings Behind The Lines and Wrinkles On Your FaceDokument7 SeitenHidden Meanings Behind The Lines and Wrinkles On Your FacebazediNoch keine Bewertungen
- Facial Exercises - Face Yoga and Facial Fitness - News - DentagamaDokument4 SeitenFacial Exercises - Face Yoga and Facial Fitness - News - DentagamabazediNoch keine Bewertungen
- Aroma 1Dokument8 SeitenAroma 1bazediNoch keine Bewertungen
- Healing Through Face Mapping - Dark Circles Under The Eyes - IN - TotalWellnessDokument5 SeitenHealing Through Face Mapping - Dark Circles Under The Eyes - IN - TotalWellnessbazediNoch keine Bewertungen
- Old Chinese Medicine - The Role of Emotion in The Body - Motherhood CommunityDokument29 SeitenOld Chinese Medicine - The Role of Emotion in The Body - Motherhood CommunitybazediNoch keine Bewertungen
- Journal of Essential Oil Research: To Cite This Article: Antonella Verzera & Antonella Cotroneo (1992) On TheDokument10 SeitenJournal of Essential Oil Research: To Cite This Article: Antonella Verzera & Antonella Cotroneo (1992) On ThebazediNoch keine Bewertungen
- Rivers - Jane Ayurveda For Beginners - Understand and Apply Essential Ayurvedic Principles and PracticDokument146 SeitenRivers - Jane Ayurveda For Beginners - Understand and Apply Essential Ayurvedic Principles and Practicbazedi100% (1)
- 250 Recipes For Essential Oils Anti-AgingDokument94 Seiten250 Recipes For Essential Oils Anti-AgingRey David100% (6)
- Rivers - Jane Ayurveda For Beginners - Understand and Apply Essential Ayurvedic Principles and PracticDokument146 SeitenRivers - Jane Ayurveda For Beginners - Understand and Apply Essential Ayurvedic Principles and PracticbazediNoch keine Bewertungen
- Understanding Acupuncture For DepressionDokument9 SeitenUnderstanding Acupuncture For DepressionbazediNoch keine Bewertungen
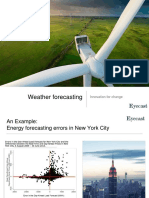
- Team 5 - Weather Forecasting - EyeCastDokument23 SeitenTeam 5 - Weather Forecasting - EyeCastbazediNoch keine Bewertungen
- The Most Used Acupuncture Points in Clinical Practice! - AcuPro Academy - Acupuncture Online CoursesDokument20 SeitenThe Most Used Acupuncture Points in Clinical Practice! - AcuPro Academy - Acupuncture Online Coursesbazedi100% (2)
- Traditional Chinese Medicine Diagnosis - FACE MAPPINGDokument5 SeitenTraditional Chinese Medicine Diagnosis - FACE MAPPINGbazediNoch keine Bewertungen
- The 13 GHOST Points in Acupuncture - AcuPro Academy - Acupuncture Online CoursesDokument17 SeitenThe 13 GHOST Points in Acupuncture - AcuPro Academy - Acupuncture Online Coursesbazedi100% (1)
- 1 s2.0 S2221169115001033 Main PDFDokument11 Seiten1 s2.0 S2221169115001033 Main PDFxiuhtlaltzinNoch keine Bewertungen
- Modeling, Control, and DYNAMIC PERFORMANCE Ro WITH PVDokument42 SeitenModeling, Control, and DYNAMIC PERFORMANCE Ro WITH PVbazediNoch keine Bewertungen
- Face Mapping in Chinese Medicine - AcuPro Academy - Acupuncture Online CoursesDokument7 SeitenFace Mapping in Chinese Medicine - AcuPro Academy - Acupuncture Online CoursesbazediNoch keine Bewertungen
- Dynamic Modeling of A Simple Reverse Osmosis Desalination Plant For Advanced Control PurposesDokument6 SeitenDynamic Modeling of A Simple Reverse Osmosis Desalination Plant For Advanced Control PurposesbazediNoch keine Bewertungen
- Modeling, Control, and Dynamic Performance Analysis of A ReverseDokument15 SeitenModeling, Control, and Dynamic Performance Analysis of A ReversebazediNoch keine Bewertungen
- Team 6 - Air QualityDokument10 SeitenTeam 6 - Air QualitybazediNoch keine Bewertungen
- Harvesting Microalgae Using Vibrating, Negatively Charged, PatternedDokument11 SeitenHarvesting Microalgae Using Vibrating, Negatively Charged, PatternedbazediNoch keine Bewertungen
- Renergy: Fresh Water For IndustryDokument10 SeitenRenergy: Fresh Water For IndustrybazediNoch keine Bewertungen
- The Use of Microalgae For Coupling Wastewater Treatment With CO BiofixationDokument12 SeitenThe Use of Microalgae For Coupling Wastewater Treatment With CO BiofixationbazediNoch keine Bewertungen
- Richard K. Nongard, Kelley T. Woods - Reframing Hypnotherapy - Evidence-Based Techniques For Your Next Hypnosis Session-Peachtree Professional Education (2018)Dokument163 SeitenRichard K. Nongard, Kelley T. Woods - Reframing Hypnotherapy - Evidence-Based Techniques For Your Next Hypnosis Session-Peachtree Professional Education (2018)bazedi100% (2)
- Advanced Control of A Reverse Osmosis de PDFDokument7 SeitenAdvanced Control of A Reverse Osmosis de PDFfet tommNoch keine Bewertungen
- Hypnosis for Weight Loss: A Revolutionary ApproachDokument33 SeitenHypnosis for Weight Loss: A Revolutionary Approachbazedi100% (1)
- (Global Environmental Studies) Aiko Endo, Tomohiro Oh - The Water-Energy-Food Nexus-Springer Singapore (2018)Dokument330 Seiten(Global Environmental Studies) Aiko Endo, Tomohiro Oh - The Water-Energy-Food Nexus-Springer Singapore (2018)bazediNoch keine Bewertungen
- Design 10,000 m3/d SWRO plantDokument78 SeitenDesign 10,000 m3/d SWRO plantbazediNoch keine Bewertungen
- The Water Energy and Food Security Nexus in The Arab Region Water Security in A New WorldDokument239 SeitenThe Water Energy and Food Security Nexus in The Arab Region Water Security in A New WorldMuhiddin ChandraNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- MR NITIN PDFDokument2 SeitenMR NITIN PDFVenkat Nitin GuttaNoch keine Bewertungen
- Crohn's Disease Case Study: Matt SimsDokument14 SeitenCrohn's Disease Case Study: Matt SimsKipchirchir AbednegoNoch keine Bewertungen
- Integumentary SystemDokument22 SeitenIntegumentary SystemEunice Angela FulguerasNoch keine Bewertungen
- Michael Goss - Death CertificateDokument1 SeiteMichael Goss - Death CertificateAlex EstradaNoch keine Bewertungen
- Prelim Exam - PEC 1 Human Anatomy and PhysiologyDokument2 SeitenPrelim Exam - PEC 1 Human Anatomy and PhysiologyColeen BentoyNoch keine Bewertungen
- Defn: Periodic Spasm of Bronchial Smooth Muscles, Increased Secretion, andDokument5 SeitenDefn: Periodic Spasm of Bronchial Smooth Muscles, Increased Secretion, andSambit BeheraNoch keine Bewertungen
- Uses of Inhaler DevicesDokument39 SeitenUses of Inhaler Devicesluis_chubeeNoch keine Bewertungen
- Nnewfile 2Dokument2 SeitenNnewfile 2mahariyaNoch keine Bewertungen
- HPNDokument32 SeitenHPNkaren GoNoch keine Bewertungen
- Common Side Effects of OtezlaDokument57 SeitenCommon Side Effects of OtezlaMica JeremijevicNoch keine Bewertungen
- Perez TMC-213 Module-2Dokument4 SeitenPerez TMC-213 Module-2NISHA MIKLE MACULNoch keine Bewertungen
- Womens Gynecologic Health Third EditionDokument912 SeitenWomens Gynecologic Health Third Editionmandy nations100% (4)
- Understanding Toxic Goiter and Its Nursing CareDokument22 SeitenUnderstanding Toxic Goiter and Its Nursing CareJohn Matley Caampued100% (2)
- Clinical and Social Factors Associated With Violent Behavior in Persons With Schizophrenia Spectrum DisordersDokument6 SeitenClinical and Social Factors Associated With Violent Behavior in Persons With Schizophrenia Spectrum DisordersIJAR JOURNALNoch keine Bewertungen
- 2Dokument4 Seiten2Emmyr JohnNoch keine Bewertungen
- Artificial PancreasDokument5 SeitenArtificial PancreasShreeja SPNoch keine Bewertungen
- Balance and Fall Prevention: By, Sankari Nedunsaliyan Physiotherapist Dip in PT (MAL), BSC Hons Applied Rehab (UK)Dokument63 SeitenBalance and Fall Prevention: By, Sankari Nedunsaliyan Physiotherapist Dip in PT (MAL), BSC Hons Applied Rehab (UK)Ali ImranNoch keine Bewertungen
- Evaluasi Program Pemberian Tablet Tambah Darah Pada Remaja Putri Anemia Dan Non Anemia Di Wilayah Puskesmas AntapaniDokument9 SeitenEvaluasi Program Pemberian Tablet Tambah Darah Pada Remaja Putri Anemia Dan Non Anemia Di Wilayah Puskesmas AntapaniAgung JayaNoch keine Bewertungen
- Drugs Acting On Respiratory SystemDokument52 SeitenDrugs Acting On Respiratory SystemIrwan M. Iskober100% (4)
- COVID-19 Hypercoagulability Mechanisms ReviewDokument13 SeitenCOVID-19 Hypercoagulability Mechanisms ReviewMartha OktaviaNoch keine Bewertungen
- EM Boot Camp Course ManualDokument531 SeitenEM Boot Camp Course ManualshortysdavidNoch keine Bewertungen
- CETEBE Leafleat 165x235mm 4pagesDokument2 SeitenCETEBE Leafleat 165x235mm 4pagestsveta.bozhinovaNoch keine Bewertungen
- Aluminium Foil For Smoking DrugsDokument6 SeitenAluminium Foil For Smoking Drugscamille64Noch keine Bewertungen
- Ohio Voter Rights CoalitionDokument19 SeitenOhio Voter Rights CoalitionsrichardsonNoch keine Bewertungen
- Test Bank For Evidence Based Practice in Nursing Healthcare 4th EditionDokument36 SeitenTest Bank For Evidence Based Practice in Nursing Healthcare 4th Editiontyphous.madrierdvfzai100% (47)
- Community DentistryDokument11 SeitenCommunity DentistryMunir AkhtarNoch keine Bewertungen
- 490.082 Microsite PublicDokument16 Seiten490.082 Microsite PublicA.J. YounesNoch keine Bewertungen
- Happy Hearts BrochureDokument2 SeitenHappy Hearts Brochuresuperindian87Noch keine Bewertungen
- Guidelines For The Medicines and Therapeutics CommitteeDokument20 SeitenGuidelines For The Medicines and Therapeutics CommitteeLorezza Miranda Aguilar100% (1)
- Guide to Bursitis Causes, Symptoms, and TreatmentDokument8 SeitenGuide to Bursitis Causes, Symptoms, and TreatmentAgeededin HartNoch keine Bewertungen