Das könnte Ihnen auch gefallen
- The COVID-19 Food Relief Program in Nepal: Assessment and Lessons for the FutureVon EverandThe COVID-19 Food Relief Program in Nepal: Assessment and Lessons for the FutureNoch keine Bewertungen
- 5 6273901644027528058 PDFDokument60 Seiten5 6273901644027528058 PDFYuan Zhi YiNoch keine Bewertungen
- BBBP Guidelines 2019Dokument103 SeitenBBBP Guidelines 2019State Resource Centre for Women Andhra PradeshNoch keine Bewertungen
- Nutrition Evaluation Report Vol IDokument106 SeitenNutrition Evaluation Report Vol IShiny Mehjabin MansuraNoch keine Bewertungen
- Nutrition Strategy BookletDokument114 SeitenNutrition Strategy BookletramyaNoch keine Bewertungen
- IDinsight THR+Report Raj+JhaDokument28 SeitenIDinsight THR+Report Raj+JhaSamia MehrajNoch keine Bewertungen
- PC 1 CM Stunting Reduction Program For FY (2017-21)Dokument64 SeitenPC 1 CM Stunting Reduction Program For FY (2017-21)f.a.shah78Noch keine Bewertungen
- WB Spending Better To Reduce Stunting in Indonesia Findings From A Public Expenditure ReviewDokument46 SeitenWB Spending Better To Reduce Stunting in Indonesia Findings From A Public Expenditure ReviewefenditubeNoch keine Bewertungen
- Anm 1 241220Dokument384 SeitenAnm 1 241220Chirag BharwadNoch keine Bewertungen
- Enhancing The LivelihoodDokument31 SeitenEnhancing The Livelihoodgirish1070100% (1)
- CBE Guidelines EnglishDokument32 SeitenCBE Guidelines EnglishYogesh GaurNoch keine Bewertungen
- Book Proyash Layout Eng PDFDokument40 SeitenBook Proyash Layout Eng PDFshahriarrajNoch keine Bewertungen
- Budget For Children in AP - FinalDokument261 SeitenBudget For Children in AP - Finaldolon bhattacharyyaNoch keine Bewertungen
- Final Rep CABA, UnicefDokument65 SeitenFinal Rep CABA, UnicefIrada Parajuli GautamNoch keine Bewertungen
- PC-1 IRMNCH and NP Punjab 2015-17Dokument120 SeitenPC-1 IRMNCH and NP Punjab 2015-17Ejaz AhmadNoch keine Bewertungen
- FP2020 VisionDokument197 SeitenFP2020 Visionannu panchalNoch keine Bewertungen
- SRSP Annual Review 2016Dokument42 SeitenSRSP Annual Review 2016zeenixNoch keine Bewertungen
- Beti Bachao Beti PadhaoDokument99 SeitenBeti Bachao Beti Padhaoghosh.srikanta404Noch keine Bewertungen
- Appeals - 01 - 2017 - Darfur Programme in Sudan - SDN 171Dokument43 SeitenAppeals - 01 - 2017 - Darfur Programme in Sudan - SDN 171Mojahid AzizNoch keine Bewertungen
- Nurses in Implementation of National Rural Health Mission: Dr. Pratima Mittra Sr. Consultant, RCH - Ii / NRHM NihfwDokument32 SeitenNurses in Implementation of National Rural Health Mission: Dr. Pratima Mittra Sr. Consultant, RCH - Ii / NRHM NihfwPabhat KumarNoch keine Bewertungen
- Revised Guidelines BBBP - 26th April, 2018 - 1Dokument111 SeitenRevised Guidelines BBBP - 26th April, 2018 - 1PIYUSH KUMAR 9D 31Noch keine Bewertungen
- BestpracDokument87 SeitenBestpracGortonTroyNoch keine Bewertungen
- Child Survival Action Plan - Sierra Leone 2023-2025Dokument36 SeitenChild Survival Action Plan - Sierra Leone 2023-2025Saurav AmanNoch keine Bewertungen
- Bi-Annual Report 2018 - 2019 2019 - 2020: Institute For Youth and Development (Iyd)Dokument36 SeitenBi-Annual Report 2018 - 2019 2019 - 2020: Institute For Youth and Development (Iyd)Vernika AgrawalNoch keine Bewertungen
- #1 State of ECCD in The Philippines - 2019Dokument108 Seiten#1 State of ECCD in The Philippines - 2019philipjudeacidreNoch keine Bewertungen
- Interim Narrative Semi Annual Report CDG Final ISAF Jun18Dokument24 SeitenInterim Narrative Semi Annual Report CDG Final ISAF Jun18Kato SOLOMONNoch keine Bewertungen
- National Social and Behaviour Change Communication Strategy For Integrated Ecd Nutrition and Wash 2018-2024Dokument78 SeitenNational Social and Behaviour Change Communication Strategy For Integrated Ecd Nutrition and Wash 2018-2024rukwavuNoch keine Bewertungen
- Kap Kes - Indra 2021Dokument6 SeitenKap Kes - Indra 2021SRI HARTATIKNoch keine Bewertungen
- ME Framework NHSP II Final 08 May 2012Dokument43 SeitenME Framework NHSP II Final 08 May 2012abdirizak husseinNoch keine Bewertungen
- ME Framework NHSP II Final 08 May 2012Dokument43 SeitenME Framework NHSP II Final 08 May 2012YGDNoch keine Bewertungen
- Kjidf IntroDokument16 SeitenKjidf IntroDhananjay ThackerayNoch keine Bewertungen
- Dadra and Nagar HaveliDokument86 SeitenDadra and Nagar HaveliAnuradha 1Noch keine Bewertungen
- Final Frame Work DistDokument19 SeitenFinal Frame Work DistMahesh Sriramula100% (1)
- PHE Implementation Models and Mechanisms: Session 5Dokument16 SeitenPHE Implementation Models and Mechanisms: Session 5Ynich Đ OnasopmacNoch keine Bewertungen
- Idl 57581Dokument71 SeitenIdl 57581Nikhitha S NairNoch keine Bewertungen
- NEHAP 2030 Version 1Dokument78 SeitenNEHAP 2030 Version 1jemma chayocasNoch keine Bewertungen
- Micronutrient Deficiencies and Interventions in Cambodia - InformationDokument104 SeitenMicronutrient Deficiencies and Interventions in Cambodia - InformationJoel ConkleNoch keine Bewertungen
- The ADB Health Sector: Implementation of The OPH and Workplan by Susann RothDokument5 SeitenThe ADB Health Sector: Implementation of The OPH and Workplan by Susann RothADB Health Sector GroupNoch keine Bewertungen
- HNP SIP Draft 3.0 - Master Doc - 27.02.2015 MinDokument70 SeitenHNP SIP Draft 3.0 - Master Doc - 27.02.2015 MinShahidul Islam ChowdhuryNoch keine Bewertungen
- Zambia's First 1 000 Most Critical Days Programme A Case StudyDokument24 SeitenZambia's First 1 000 Most Critical Days Programme A Case StudyGlory ShanunguNoch keine Bewertungen
- FP2020-Vision-in IndiaDokument162 SeitenFP2020-Vision-in IndiaNeenu RajputNoch keine Bewertungen
- West Bengal SDG NitiAayog Feb2018Dokument16 SeitenWest Bengal SDG NitiAayog Feb2018esa2reportNoch keine Bewertungen
- Health Annual Report 2011Dokument21 SeitenHealth Annual Report 2011Naila AnsariNoch keine Bewertungen
- 5 Year Plans of India: By: Alka Mishra M. Sc. Nursing 1 YrDokument73 Seiten5 Year Plans of India: By: Alka Mishra M. Sc. Nursing 1 YrSiva KumarNoch keine Bewertungen
- IndonesiaGood PracticesDokument8 SeitenIndonesiaGood PracticesEleonora HopeNoch keine Bewertungen
- National RMNCAH&N Strategy 2016-2020Dokument44 SeitenNational RMNCAH&N Strategy 2016-2020Dr. Rafi KhattakNoch keine Bewertungen
- ARNEC Webinar Series 2, No.2 - Focus On Health and Nutrition - Presentation Slides Deck - 11 JanDokument77 SeitenARNEC Webinar Series 2, No.2 - Focus On Health and Nutrition - Presentation Slides Deck - 11 JansyarenNoch keine Bewertungen
- MEStrategyActionPlan PRE PRINTDokument84 SeitenMEStrategyActionPlan PRE PRINThoàng đặngNoch keine Bewertungen
- National Programmes: DR Nishant Verma Assistant Professor Department of Pediatrics King George's Medical UniversityDokument51 SeitenNational Programmes: DR Nishant Verma Assistant Professor Department of Pediatrics King George's Medical UniversityVaishali AmbilkarNoch keine Bewertungen
- NNF Newborn Screening Consultative Meet Final ReportDokument26 SeitenNNF Newborn Screening Consultative Meet Final Reportlovina candra kiranaNoch keine Bewertungen
- Beti Bachao Beti Padhao (BBBP) Beti Bachao Beti Padhao (BBBP) Beti Bachao BetiDokument28 SeitenBeti Bachao Beti Padhao (BBBP) Beti Bachao Beti Padhao (BBBP) Beti Bachao BetiKingNoch keine Bewertungen
- Yumbe District Advocacy Strategy 2020-2030Dokument17 SeitenYumbe District Advocacy Strategy 2020-2030yumbengo forumNoch keine Bewertungen
- A'AGO Project - Improving Sexual and Reproductive Health Outcomes of Afari Young PeopleDokument26 SeitenA'AGO Project - Improving Sexual and Reproductive Health Outcomes of Afari Young PeopleJodel PierreNoch keine Bewertungen
- Projects, Programs, Policies and StrategiesDokument55 SeitenProjects, Programs, Policies and StrategiesBangladesh 71Noch keine Bewertungen
- Aipmnh Annual Work Plan 2012 Indonesian PDFDokument67 SeitenAipmnh Annual Work Plan 2012 Indonesian PDFsalmanNoch keine Bewertungen
- Ank ProfileDokument43 SeitenAnk ProfileAbhishekNoch keine Bewertungen
- HRH Profile Balochistan 2012Dokument35 SeitenHRH Profile Balochistan 2012Munir HussainNoch keine Bewertungen
- Tanzania National Guidelines Initiating Managing CbrchsDokument23 SeitenTanzania National Guidelines Initiating Managing CbrchsPaulNoch keine Bewertungen
- WFP 0000003294Dokument125 SeitenWFP 0000003294AgazyanHintsaNoch keine Bewertungen
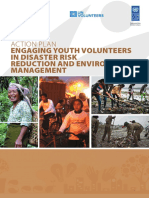
- Action Plan - Engaging Youth Volunteers in Disaster Risk Reduction and Environment ManagementDokument88 SeitenAction Plan - Engaging Youth Volunteers in Disaster Risk Reduction and Environment ManagementMDRRMO BulaNoch keine Bewertungen
- Ten Rules For Writing FictionDokument19 SeitenTen Rules For Writing FictionBISTIRNA BARUANoch keine Bewertungen
- Jara Aankh Mein Bhar Lo PaaniDokument4 SeitenJara Aankh Mein Bhar Lo PaaniBISTIRNA BARUANoch keine Bewertungen
- Remembering Lata MangeshkarDokument4 SeitenRemembering Lata MangeshkarBISTIRNA BARUANoch keine Bewertungen
- The Joy of Being Completely AloneDokument11 SeitenThe Joy of Being Completely AloneBISTIRNA BARUANoch keine Bewertungen
- Agniputra by Sunil GangopadhyayDokument61 SeitenAgniputra by Sunil GangopadhyayBISTIRNA BARUANoch keine Bewertungen
- Pakistanis Mourn Lata Mangeshkar TooDokument5 SeitenPakistanis Mourn Lata Mangeshkar TooBISTIRNA BARUANoch keine Bewertungen
- Magic of Her Voice Will Live ForeverDokument2 SeitenMagic of Her Voice Will Live ForeverBISTIRNA BARUANoch keine Bewertungen
- J Sai DeepakDokument1 SeiteJ Sai DeepakBISTIRNA BARUANoch keine Bewertungen
- Last Letter - Ted Hughes Poem On Sylvia Plath's DeathDokument4 SeitenLast Letter - Ted Hughes Poem On Sylvia Plath's DeathBISTIRNA BARUA0% (1)
- Sigmund FreudDokument2 SeitenSigmund FreudBISTIRNA BARUANoch keine Bewertungen
- A Tribute To Late DR Bhabendra Nath SaikiaDokument2 SeitenA Tribute To Late DR Bhabendra Nath SaikiaBISTIRNA BARUANoch keine Bewertungen
- Meri Awaaz Hi Pehchaan HaiDokument3 SeitenMeri Awaaz Hi Pehchaan HaiBISTIRNA BARUANoch keine Bewertungen
- Martin HeideggerDokument2 SeitenMartin HeideggerBISTIRNA BARUANoch keine Bewertungen
- 4TH Semester B.A., LL.B B.A., LL.B (H)Dokument14 Seiten4TH Semester B.A., LL.B B.A., LL.B (H)BISTIRNA BARUANoch keine Bewertungen
- Guide To Copyright and PermissionsDokument7 SeitenGuide To Copyright and PermissionsBISTIRNA BARUANoch keine Bewertungen
- Weather Forecast For Ambubachi Mela: Regional Meteorological Centre L.G.B.I. Airport Guwahati - 781 015 (Assam)Dokument1 SeiteWeather Forecast For Ambubachi Mela: Regional Meteorological Centre L.G.B.I. Airport Guwahati - 781 015 (Assam)BISTIRNA BARUANoch keine Bewertungen
- Cotton University: $/i/.dn!ru!/dlr4ioDokument2 SeitenCotton University: $/i/.dn!ru!/dlr4ioBISTIRNA BARUANoch keine Bewertungen
- in of Of: TransportDokument5 Seitenin of Of: TransportBISTIRNA BARUANoch keine Bewertungen
- Inquest Report : ....................... Police Station Case No..........................Dokument6 SeitenInquest Report : ....................... Police Station Case No..........................BISTIRNA BARUANoch keine Bewertungen
- Looking For Ismael SheikhDokument15 SeitenLooking For Ismael SheikhBISTIRNA BARUANoch keine Bewertungen
- Bhabendra Nath SaikiaDokument10 SeitenBhabendra Nath SaikiaBISTIRNA BARUANoch keine Bewertungen
- Tata Steel Code of ConductDokument16 SeitenTata Steel Code of ConductBISTIRNA BARUA100% (1)
- Preparing IAS Officer Trainees For The Role of District Magistrate: A Competency-Based ApproachDokument46 SeitenPreparing IAS Officer Trainees For The Role of District Magistrate: A Competency-Based ApproachBISTIRNA BARUANoch keine Bewertungen
- The Poetry of Ajit BaruaDokument22 SeitenThe Poetry of Ajit BaruaBISTIRNA BARUANoch keine Bewertungen
- Assamese PoetryDokument7 SeitenAssamese PoetryBISTIRNA BARUANoch keine Bewertungen
- Microsoft - Interim - Offer - Letter - Kumari - Nivedita - Nivedita KumariDokument2 SeitenMicrosoft - Interim - Offer - Letter - Kumari - Nivedita - Nivedita KumariZoe ChauhanNoch keine Bewertungen
- KYKO - A People Management System With Its Own Psychometric Personality Assessment TestsDokument72 SeitenKYKO - A People Management System With Its Own Psychometric Personality Assessment TestsBernard Ah Thau Tan100% (2)
- Engstrom Auto Mirro Plant Case Studies FFDokument2 SeitenEngstrom Auto Mirro Plant Case Studies FFNikku SinghNoch keine Bewertungen
- Tugas PPIC Solver 1Dokument2 SeitenTugas PPIC Solver 1Roy Emmanuel KristedjaNoch keine Bewertungen
- GCSE AQA Business Studies Unit 1 - RevisionDokument24 SeitenGCSE AQA Business Studies Unit 1 - RevisionwizlanNoch keine Bewertungen
- 911 Dispatcher Cover Letter No ExperienceDokument4 Seiten911 Dispatcher Cover Letter No Experiencebetevopelah3100% (2)
- Empform - Dha - InstDokument2 SeitenEmpform - Dha - Instmiqbaaalll0% (1)
- Short Case Studies and CaseletsDokument2 SeitenShort Case Studies and CaseletsDarpan NemadeNoch keine Bewertungen
- Hcil - Honda Cars Interview Call Letter.Dokument3 SeitenHcil - Honda Cars Interview Call Letter.qwerty1871900% (1)
- Labour LawDokument17 SeitenLabour LawHESHVIENIE A P VIJAYARATNAMNoch keine Bewertungen
- Myanmar Salary Survey 2021 - WebDokument32 SeitenMyanmar Salary Survey 2021 - WebKaung Set LinNoch keine Bewertungen
- Chavez Vs NLRCDokument17 SeitenChavez Vs NLRCnaomi_mateo_4Noch keine Bewertungen
- UfoneDokument25 SeitenUfonefarah arshadNoch keine Bewertungen
- Advertisement For Hiring Junior Engineer-1 For Tata Steel KalinganagarDokument1 SeiteAdvertisement For Hiring Junior Engineer-1 For Tata Steel Kalinganagar2309220Noch keine Bewertungen
- OCIP Safety ManualDokument62 SeitenOCIP Safety Manualhercules1152000Noch keine Bewertungen
- Index To West Bengal Service Rules Govt. of W.B PDFDokument4 SeitenIndex To West Bengal Service Rules Govt. of W.B PDFSOUMITRA MUDINoch keine Bewertungen
- One Minute ManagerDokument13 SeitenOne Minute Managerapi-3825047100% (1)
- Final Exam - Safety4mechatronics - Jan2019Dokument2 SeitenFinal Exam - Safety4mechatronics - Jan2019Eng. Ibrahim Abdullah AlruhmiNoch keine Bewertungen
- HRM - QuizDokument8 SeitenHRM - Quizkingsley_psbNoch keine Bewertungen
- Capstone Final ProjectDokument33 SeitenCapstone Final Projectapi-361089634Noch keine Bewertungen
- External Environment - Task Environment: (1) MarketsDokument14 SeitenExternal Environment - Task Environment: (1) MarketsYousab KaldasNoch keine Bewertungen
- Mattel and The Toy Recalls FinalDokument25 SeitenMattel and The Toy Recalls FinalSimon Pollard100% (2)
- The Minimum Wage Debate EssayDokument5 SeitenThe Minimum Wage Debate EssayWilliam Tracy AdamsNoch keine Bewertungen
- Discussed Topics: (Based On The Syllabus and Notes Consensus) General ProvisionsDokument2 SeitenDiscussed Topics: (Based On The Syllabus and Notes Consensus) General ProvisionsKimberly RamosNoch keine Bewertungen
- Recruitment and Retention Strategies-A Magnet Hospital Prevention ModelDokument10 SeitenRecruitment and Retention Strategies-A Magnet Hospital Prevention ModelNelson SousaNoch keine Bewertungen
- Exemple CV Filetype PDFDokument2 SeitenExemple CV Filetype PDFNancyNoch keine Bewertungen
- HR Metrics and OutsourcingDokument35 SeitenHR Metrics and OutsourcingUma Devi AnanthNoch keine Bewertungen
- Woolbert Job ApplicationDokument1 SeiteWoolbert Job ApplicationDrew RittenhouseNoch keine Bewertungen
- Presentation 5Dokument3 SeitenPresentation 5api-356401960Noch keine Bewertungen
- (Update) Chapter 10 - Inheritance and PolymorphismDokument4 Seiten(Update) Chapter 10 - Inheritance and PolymorphismEng SayidNoch keine Bewertungen
- Unwanted Advances: Sexual Paranoia Comes to CampusVon EverandUnwanted Advances: Sexual Paranoia Comes to CampusBewertung: 4 von 5 Sternen4/5 (22)
- Gender Trouble: Feminism and the Subversion of IdentityVon EverandGender Trouble: Feminism and the Subversion of IdentityBewertung: 4 von 5 Sternen4/5 (317)
- Feminine Consciousness, Archetypes, and Addiction to PerfectionVon EverandFeminine Consciousness, Archetypes, and Addiction to PerfectionBewertung: 5 von 5 Sternen5/5 (90)
- Never Chase Men Again: 38 Dating Secrets to Get the Guy, Keep Him Interested, and Prevent Dead-End RelationshipsVon EverandNever Chase Men Again: 38 Dating Secrets to Get the Guy, Keep Him Interested, and Prevent Dead-End RelationshipsBewertung: 4.5 von 5 Sternen4.5/5 (387)
- The Will to Change: Men, Masculinity, and LoveVon EverandThe Will to Change: Men, Masculinity, and LoveBewertung: 5 von 5 Sternen5/5 (384)
- Sex and the City and Us: How Four Single Women Changed the Way We Think, Live, and LoveVon EverandSex and the City and Us: How Four Single Women Changed the Way We Think, Live, and LoveBewertung: 4.5 von 5 Sternen4.5/5 (22)
- Summary: Fair Play: A Game-Changing Solution for When You Have Too Much to Do (and More Life to Live) by Eve Rodsky: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: Fair Play: A Game-Changing Solution for When You Have Too Much to Do (and More Life to Live) by Eve Rodsky: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (1)
- King, Warrior, Magician, Lover: Rediscovering the Archetypes of the Mature MasculineVon EverandKing, Warrior, Magician, Lover: Rediscovering the Archetypes of the Mature MasculineBewertung: 4 von 5 Sternen4/5 (65)
- Period Power: Harness Your Hormones and Get Your Cycle Working For YouVon EverandPeriod Power: Harness Your Hormones and Get Your Cycle Working For YouBewertung: 4 von 5 Sternen4/5 (25)
- Crones Don't Whine: Concentrated Wisdom for Juicy WomenVon EverandCrones Don't Whine: Concentrated Wisdom for Juicy WomenBewertung: 2.5 von 5 Sternen2.5/5 (3)
- Unlikeable Female Characters: The Women Pop Culture Wants You to HateVon EverandUnlikeable Female Characters: The Women Pop Culture Wants You to HateBewertung: 4 von 5 Sternen4/5 (18)
- For the Love of Men: From Toxic to a More Mindful MasculinityVon EverandFor the Love of Men: From Toxic to a More Mindful MasculinityBewertung: 4.5 von 5 Sternen4.5/5 (56)
- The End of Gender: Debunking the Myths about Sex and Identity in Our SocietyVon EverandThe End of Gender: Debunking the Myths about Sex and Identity in Our SocietyBewertung: 4 von 5 Sternen4/5 (126)
- She: Understanding Feminine PsychologyVon EverandShe: Understanding Feminine PsychologyBewertung: 4.5 von 5 Sternen4.5/5 (34)
- From the Core: A New Masculine Paradigm for Leading with Love, Living Your Truth & Healing the WorldVon EverandFrom the Core: A New Masculine Paradigm for Leading with Love, Living Your Truth & Healing the WorldBewertung: 4.5 von 5 Sternen4.5/5 (16)
- Yearning: Race, Gender, and Cultural Politics, 2nd EditionVon EverandYearning: Race, Gender, and Cultural Politics, 2nd EditionBewertung: 4 von 5 Sternen4/5 (2)
- Family Shepherds: Calling and Equipping Men to Lead Their HomesVon EverandFamily Shepherds: Calling and Equipping Men to Lead Their HomesBewertung: 5 von 5 Sternen5/5 (66)
- He: Understanding Masculine PsychologyVon EverandHe: Understanding Masculine PsychologyBewertung: 4.5 von 5 Sternen4.5/5 (23)
- You're Cute When You're Mad: Simple Steps for Confronting SexismVon EverandYou're Cute When You're Mad: Simple Steps for Confronting SexismBewertung: 4 von 5 Sternen4/5 (271)
- What Do We Need Men For?: A Modest ProposalVon EverandWhat Do We Need Men For?: A Modest ProposalBewertung: 4 von 5 Sternen4/5 (9)