Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Pubmed ResultDokument2 SeitenPubmed ResultArturo Martí-CarvajalNoch keine Bewertungen
- Aaronson 1989Dokument14 SeitenAaronson 1989Arturo Martí-CarvajalNoch keine Bewertungen
- Phase 2 Trial of Montelukast For Prevention of Pain in Sickle Cell Disease.Dokument2 SeitenPhase 2 Trial of Montelukast For Prevention of Pain in Sickle Cell Disease.Arturo Martí-CarvajalNoch keine Bewertungen
- Share Delayed Hemolytic Transfusion Reaction in A Sickle Cell Disease Patient: A Case Report.Dokument4 SeitenShare Delayed Hemolytic Transfusion Reaction in A Sickle Cell Disease Patient: A Case Report.Arturo Martí-CarvajalNoch keine Bewertungen
- Exogenously Applied 5-Aminolevulinic Acid Modulates Growth, Secondary Metabolism and Oxidative Defense in Sunflower Under Water Deficit Stress.Dokument2 SeitenExogenously Applied 5-Aminolevulinic Acid Modulates Growth, Secondary Metabolism and Oxidative Defense in Sunflower Under Water Deficit Stress.Arturo Martí-CarvajalNoch keine Bewertungen
- The Role of Red Blood Cell Exchange in Sickle Cell Disease in Patient With COVID-19 Infection and Pulmonary InfiltratesDokument8 SeitenThe Role of Red Blood Cell Exchange in Sickle Cell Disease in Patient With COVID-19 Infection and Pulmonary InfiltratesArturo Martí-CarvajalNoch keine Bewertungen
- Hemodynamic Effects of The Dipeptidyl Peptidase-4 Inhibitor Linagliptin With Renin-Angiotensin System Inhibitors in Type 2 Diabetic Patients With Albuminuria.Dokument7 SeitenHemodynamic Effects of The Dipeptidyl Peptidase-4 Inhibitor Linagliptin With Renin-Angiotensin System Inhibitors in Type 2 Diabetic Patients With Albuminuria.Arturo Martí-CarvajalNoch keine Bewertungen
- End Points For Sickle Cell Disease Clinical Trials: Renal and Cardiopulmonary, Cure, and Low-Resource Settings.Dokument3 SeitenEnd Points For Sickle Cell Disease Clinical Trials: Renal and Cardiopulmonary, Cure, and Low-Resource Settings.Arturo Martí-CarvajalNoch keine Bewertungen
- Transplant-Eligible Patients Must Be Referred To Tertiary Medical Centers For Consideration of haplo-HCTDokument2 SeitenTransplant-Eligible Patients Must Be Referred To Tertiary Medical Centers For Consideration of haplo-HCTArturo Martí-CarvajalNoch keine Bewertungen
- Fphys-11-00031salbutamol Worsens The Autonomic Nervous System Dysfunction of Children With Sickle Cell Disease.Dokument11 SeitenFphys-11-00031salbutamol Worsens The Autonomic Nervous System Dysfunction of Children With Sickle Cell Disease.Arturo Martí-CarvajalNoch keine Bewertungen
- Sickle Cell Disease and Quality of LifeDokument7 SeitenSickle Cell Disease and Quality of LifeArturo Martí-CarvajalNoch keine Bewertungen
- Nfestation Mechanisms of Two Woodborer Species in The Mangrove Sonneratia Alba J. Smith in Kenya and Co-Occurring Endophytic Fungi.Dokument20 SeitenNfestation Mechanisms of Two Woodborer Species in The Mangrove Sonneratia Alba J. Smith in Kenya and Co-Occurring Endophytic Fungi.Arturo Martí-CarvajalNoch keine Bewertungen
- Effects of Repleting Organic Phosphates in Banked Erythrocytes On Plasma Metabolites and Vasoactive Mediators After Red Cell Exchange Transfusion in Sickle Cell Disease.Dokument2 SeitenEffects of Repleting Organic Phosphates in Banked Erythrocytes On Plasma Metabolites and Vasoactive Mediators After Red Cell Exchange Transfusion in Sickle Cell Disease.Arturo Martí-CarvajalNoch keine Bewertungen
- Effects of Dipeptidyl Peptidase-4 Inhibitors On Renal Outcomes in Patients With Type 2 Diabetes: A Systematic Review and Meta-Analysis.Dokument13 SeitenEffects of Dipeptidyl Peptidase-4 Inhibitors On Renal Outcomes in Patients With Type 2 Diabetes: A Systematic Review and Meta-Analysis.Arturo Martí-CarvajalNoch keine Bewertungen
- When Money Talks: Judging Risk and Coercion in High-Paying Clinical TrialsDokument15 SeitenWhen Money Talks: Judging Risk and Coercion in High-Paying Clinical TrialsArturo Martí-CarvajalNoch keine Bewertungen
- Viruses 12 00204 PDFDokument21 SeitenViruses 12 00204 PDFArturo Martí-CarvajalNoch keine Bewertungen
- Linagliptin and Its Effects On Hyperglycaemia and Albuminuria in Patients With Type 2 Diabetes and Renal Dysfunction: The Randomized MARLINA-T2D Trial.Dokument10 SeitenLinagliptin and Its Effects On Hyperglycaemia and Albuminuria in Patients With Type 2 Diabetes and Renal Dysfunction: The Randomized MARLINA-T2D Trial.Arturo Martí-CarvajalNoch keine Bewertungen
- Hemolytic Transfusion Reactions in Sickle Cell Disease: Underappreciated and Potentially Fatal.Dokument7 SeitenHemolytic Transfusion Reactions in Sickle Cell Disease: Underappreciated and Potentially Fatal.Arturo Martí-CarvajalNoch keine Bewertungen
- Impact of A Paediatric-Adult Care Transition Programme On The Health Status of Patients With Sickle Cell Disease: Study Protocol For A Randomised Controlled Trial (The DREPADO Trial) .Dokument9 SeitenImpact of A Paediatric-Adult Care Transition Programme On The Health Status of Patients With Sickle Cell Disease: Study Protocol For A Randomised Controlled Trial (The DREPADO Trial) .Arturo Martí-CarvajalNoch keine Bewertungen
- Flexible Learning Spaces Facilitate Interaction, Collaboration and Behavioural Engagement in Secondary School.Dokument2 SeitenFlexible Learning Spaces Facilitate Interaction, Collaboration and Behavioural Engagement in Secondary School.Arturo Martí-CarvajalNoch keine Bewertungen
- Inactivation of Chronic Wasting Disease Prions Using Sodium HypochloriteDokument2 SeitenInactivation of Chronic Wasting Disease Prions Using Sodium HypochloriteArturo Martí-CarvajalNoch keine Bewertungen
- Weakening The Subjective Sensation of Own Hand Ownership Does Not Interfere With Rapid Finger Movements. ResultDokument2 SeitenWeakening The Subjective Sensation of Own Hand Ownership Does Not Interfere With Rapid Finger Movements. ResultArturo Martí-CarvajalNoch keine Bewertungen
- The Phenotype and Functional Activity of Mesenchymal Stromal Cells in Pediatric Patients With Non-Malignant Hematological Diseases.Dokument16 SeitenThe Phenotype and Functional Activity of Mesenchymal Stromal Cells in Pediatric Patients With Non-Malignant Hematological Diseases.Arturo Martí-CarvajalNoch keine Bewertungen
- Components of The Full Blood Count As Risk Factors For Colorectal Cancer Detection: A Systematic Review ProtocolDokument5 SeitenComponents of The Full Blood Count As Risk Factors For Colorectal Cancer Detection: A Systematic Review ProtocolArturo Martí-CarvajalNoch keine Bewertungen
- Profile of Crizanlizumab and Its Potential in The Prevention of Pain Crises in Sickle Cell Disease: Evidence To Date.Dokument5 SeitenProfile of Crizanlizumab and Its Potential in The Prevention of Pain Crises in Sickle Cell Disease: Evidence To Date.Arturo Martí-CarvajalNoch keine Bewertungen
- Decoding The Role of SOD2 in Sickle Cell Disease.Dokument9 SeitenDecoding The Role of SOD2 in Sickle Cell Disease.Arturo Martí-CarvajalNoch keine Bewertungen
- Vascular Instability and Neurological Morbidity in Sickle Cell Disease: An Integrative Framework.Dokument21 SeitenVascular Instability and Neurological Morbidity in Sickle Cell Disease: An Integrative Framework.Arturo Martí-CarvajalNoch keine Bewertungen
- Evaluation of Hydroxyurea Genotoxicity in Patients With Sickle Cell Disease.Dokument5 SeitenEvaluation of Hydroxyurea Genotoxicity in Patients With Sickle Cell Disease.Arturo Martí-CarvajalNoch keine Bewertungen
- Total Serum Magnesium Levels and Calcium-To-Magnesium Ratio in Sickle Cell Disease.Dokument8 SeitenTotal Serum Magnesium Levels and Calcium-To-Magnesium Ratio in Sickle Cell Disease.Arturo Martí-CarvajalNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- SHR User Manual UpdatedDokument37 SeitenSHR User Manual UpdatedSheyda MavisatNoch keine Bewertungen
- Vns 01092021Dokument28 SeitenVns 01092021fanmingjinNoch keine Bewertungen
- Burns: Hadi Munib Oral and Maxillofacial SurgeryDokument79 SeitenBurns: Hadi Munib Oral and Maxillofacial SurgeryAli ahmedNoch keine Bewertungen
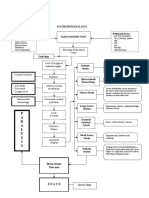
- Pathophysiology: P A R A L Y S I SDokument1 SeitePathophysiology: P A R A L Y S I SJordan Garcia AguilarNoch keine Bewertungen
- Family TiesDokument8 SeitenFamily TiesCristina Ioana NistorNoch keine Bewertungen
- Homeopathy in Dentistry: A ReviewDokument5 SeitenHomeopathy in Dentistry: A ReviewRahul MaliNoch keine Bewertungen
- Frequently Asked Questions On Tuberculosis (English) : Q: What Is Tuberculosis (TB) ?Dokument4 SeitenFrequently Asked Questions On Tuberculosis (English) : Q: What Is Tuberculosis (TB) ?Mystery ShopperNoch keine Bewertungen
- Handbook of Infant Mental Health Fourth Edition 4th Edition Ebook PDFDokument61 SeitenHandbook of Infant Mental Health Fourth Edition 4th Edition Ebook PDFjeffrey.stanton398100% (41)
- ESRD CaseDokument51 SeitenESRD Casepjerry100% (1)
- Bacteria and Immune Defenses: Helicobacter PyloriDokument4 SeitenBacteria and Immune Defenses: Helicobacter PyloriMary Rose SJ JimenezNoch keine Bewertungen
- Anamnesis Dan Pemeriksaan Fisik Diabetes Melitus Dan Sindrom Metabolik Dr. Alwi Shahab, SPPD, K-Emd Dr. Yulianto K, SPPD, K-Emd BLOK 9 2011Dokument7 SeitenAnamnesis Dan Pemeriksaan Fisik Diabetes Melitus Dan Sindrom Metabolik Dr. Alwi Shahab, SPPD, K-Emd Dr. Yulianto K, SPPD, K-Emd BLOK 9 2011tattosssNoch keine Bewertungen
- EpilepsyDokument43 SeitenEpilepsyMpt SportsNoch keine Bewertungen
- Hellp 2Dokument57 SeitenHellp 2Angela CaguitlaNoch keine Bewertungen
- Melba Case Scenario FinalDokument34 SeitenMelba Case Scenario FinalAlex Antiporda50% (2)
- Sirwan Ali Enterohemorrhagic-Escherichia-coliDokument8 SeitenSirwan Ali Enterohemorrhagic-Escherichia-coliDlzar AbubakrNoch keine Bewertungen
- The Indian Weekender 12 July 2019 (Volume 11 Issue 17)Dokument32 SeitenThe Indian Weekender 12 July 2019 (Volume 11 Issue 17)Indian Weekender ReporterNoch keine Bewertungen
- CryptococcosisDokument17 SeitenCryptococcosisKarthick AnbuNoch keine Bewertungen
- Reflux Severity Index (RSI) : 1 Month, How Did The FollowingDokument2 SeitenReflux Severity Index (RSI) : 1 Month, How Did The FollowingAnak CarolusNoch keine Bewertungen
- II-C-1 Gastrointestinal (GI) BleedingDokument4 SeitenII-C-1 Gastrointestinal (GI) BleedingDharylle CariñoNoch keine Bewertungen
- Hip Exam - OSCE Stations PDFDokument2 SeitenHip Exam - OSCE Stations PDFEmiel AwadNoch keine Bewertungen
- Peptic Ulcer DiseaseDokument17 SeitenPeptic Ulcer DiseaseAhmed Gh Al-zechrawiNoch keine Bewertungen
- Research Paper On Recombinant Dna TechnologyDokument7 SeitenResearch Paper On Recombinant Dna Technologyvagipelez1z2100% (1)
- ECG InterpretationDokument6 SeitenECG InterpretationANDREW DEL ROSARIONoch keine Bewertungen
- JHS OnlineDokument109 SeitenJHS OnlineJovil John OsuneroNoch keine Bewertungen
- Mathematical Modeling of COVID-19 Spreading With Asymptomatic Infected and Interacting PeoplesDokument23 SeitenMathematical Modeling of COVID-19 Spreading With Asymptomatic Infected and Interacting PeoplesYjhvhgjvNoch keine Bewertungen
- Konasana PoseDokument2 SeitenKonasana PoseMIBNoch keine Bewertungen
- Glycogen Storage Diseases of Muscle Chapter 39 PDFDokument26 SeitenGlycogen Storage Diseases of Muscle Chapter 39 PDFIsaac Mackliz VillegasNoch keine Bewertungen
- Co-Occurrence of Dissociative Identity Disorder and Borderline Personality DisorderDokument13 SeitenCo-Occurrence of Dissociative Identity Disorder and Borderline Personality DisorderCarla MesquitaNoch keine Bewertungen
- Downer Cow Syndrome, Creeper Cows.Dokument8 SeitenDowner Cow Syndrome, Creeper Cows.Ali H. Sadiek أ.د. علي حسن صديق100% (1)
- Activity Intolerance NCPDokument7 SeitenActivity Intolerance NCPamitNoch keine Bewertungen