Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- HemaDokument6 SeitenHemaAnonymous plYGwXNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- EndokrinDokument5 SeitenEndokrinAnonymous plYGwXNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- CardioDokument2 SeitenCardioAnonymous plYGwXNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- GastroDokument6 SeitenGastroAnonymous plYGwXNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- EndokrinDokument7 SeitenEndokrinAnonymous plYGwXNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- GastroDokument9 SeitenGastroAnonymous plYGwXNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- CardioDokument7 SeitenCardioAnonymous plYGwXNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- EndokrinDokument7 SeitenEndokrinAnonymous plYGwXNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- EndokrinDokument25 SeitenEndokrinAnonymous plYGwXNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- International Journal of CardiologyDokument5 SeitenInternational Journal of CardiologyAnonymous plYGwXNoch keine Bewertungen
- Association Between Lipid Fractions and Age of First Myocardial InfarctionDokument7 SeitenAssociation Between Lipid Fractions and Age of First Myocardial InfarctionAnonymous plYGwXNoch keine Bewertungen
- CardioDokument6 SeitenCardioAnonymous plYGwXNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Pancreas, Biliary Tract, and Liver: Clinical Features of COVID-19-Related Liver Functional AbnormalityDokument6 SeitenPancreas, Biliary Tract, and Liver: Clinical Features of COVID-19-Related Liver Functional AbnormalityAnonymous plYGwXNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- GastroDokument8 SeitenGastroAnonymous plYGwXNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Ca Recti PDFDokument9 SeitenCa Recti PDFAnonymous plYGwXNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Ca Recti PDFDokument9 SeitenCa Recti PDFAnonymous plYGwXNoch keine Bewertungen
- Elektrolit Urine 1 PDFDokument7 SeitenElektrolit Urine 1 PDFAnonymous plYGwXNoch keine Bewertungen
- Partial Prediction of Postpartum Graves' Thyrotoxicosis by Sensitive Bioassay For Thyroid-Stimulating Antibody Measured in Early PregnancyDokument4 SeitenPartial Prediction of Postpartum Graves' Thyrotoxicosis by Sensitive Bioassay For Thyroid-Stimulating Antibody Measured in Early Pregnancykartini ciatawiNoch keine Bewertungen
- Kimia Ar 1Dokument7 SeitenKimia Ar 1Anonymous plYGwXNoch keine Bewertungen
- Jurnal Mikro 2Dokument9 SeitenJurnal Mikro 2Anonymous plYGwXNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Severe Aplastic Anemia: A Prospective Study of The Effect of Early Marrow Transplantation On Acute MortalityDokument9 SeitenSevere Aplastic Anemia: A Prospective Study of The Effect of Early Marrow Transplantation On Acute MortalityAnonymous plYGwXNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The RIFLE and AKIN Classifications For Acute Kidney Injury: A Critical and Comprehensive ReviewDokument7 SeitenThe RIFLE and AKIN Classifications For Acute Kidney Injury: A Critical and Comprehensive ReviewAnonymous plYGwXNoch keine Bewertungen
- Severe Aplastic Anemia: A Prospective Study of The Effect of Early Marrow Transplantation On Acute MortalityDokument9 SeitenSevere Aplastic Anemia: A Prospective Study of The Effect of Early Marrow Transplantation On Acute MortalityAnonymous plYGwXNoch keine Bewertungen
- Vitamin K Deficiency in Critical Ill Patients - A Prospective Observational StudyDokument5 SeitenVitamin K Deficiency in Critical Ill Patients - A Prospective Observational Studykartini ciatawiNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Racial Disparities in Survival of Children and Young Adults With Leukemia and LymphomaDokument8 SeitenRacial Disparities in Survival of Children and Young Adults With Leukemia and LymphomaAnonymous plYGwXNoch keine Bewertungen
- GGT-HD 1Dokument8 SeitenGGT-HD 1Anonymous plYGwXNoch keine Bewertungen
- Mds SleDokument4 SeitenMds SleAnonymous plYGwXNoch keine Bewertungen
- Jurnal ICUSDokument5 SeitenJurnal ICUSAnonymous plYGwXNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Vitamin K Deficiency in Critical Ill Patients - A Prospective Observational StudyDokument5 SeitenVitamin K Deficiency in Critical Ill Patients - A Prospective Observational Studykartini ciatawiNoch keine Bewertungen
- Gastrointestinal Endoscopy Volume 71 Issue 7 2010 (Doi 10.1016/j.gie.2009.12.029) Lisette G. Capelle Annemarie C. de Vries Jelle Haringsma Fran - The Staging of Gastritis With The OLGA System by PDFDokument9 SeitenGastrointestinal Endoscopy Volume 71 Issue 7 2010 (Doi 10.1016/j.gie.2009.12.029) Lisette G. Capelle Annemarie C. de Vries Jelle Haringsma Fran - The Staging of Gastritis With The OLGA System by PDFAleida VivalloNoch keine Bewertungen
- Prostrolane Intra Articular en INGLESDokument6 SeitenProstrolane Intra Articular en INGLESjuanNoch keine Bewertungen
- Clinical Summary Guide 05Dokument2 SeitenClinical Summary Guide 05Diarti_PMIKNoch keine Bewertungen
- AM19-Proceedings-Full ASCO PDFDokument652 SeitenAM19-Proceedings-Full ASCO PDFrusgal8992100% (1)
- Soft tissue sarcoma overviewDokument123 SeitenSoft tissue sarcoma overviewOana BarbuNoch keine Bewertungen
- ScrofulodermDokument4 SeitenScrofulodermIzmi AzizahNoch keine Bewertungen
- Interventional BronchosDokument323 SeitenInterventional BronchosFranspol100% (1)
- Simple GoitreDokument13 SeitenSimple GoitreEmad WalyNoch keine Bewertungen
- Thrombo PhiliaDokument226 SeitenThrombo PhiliawalkerbestNoch keine Bewertungen
- Kjjhhgfdsasdf HJKLKJHGFDSSDFG HJKLDokument4 SeitenKjjhhgfdsasdf HJKLKJHGFDSSDFG HJKLbubble_inNoch keine Bewertungen
- 2016 Guía Europea de Prevención de La Enfermedad Cardiovascular en La PrácticaDokument68 Seiten2016 Guía Europea de Prevención de La Enfermedad Cardiovascular en La PrácticaPaty Alatorre IcazaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Digestive System: Maria Victoria M. Villarica MD OLFU College of Medicine Department of PediatricsDokument81 SeitenThe Digestive System: Maria Victoria M. Villarica MD OLFU College of Medicine Department of PediatricsSven OrdanzaNoch keine Bewertungen
- Course Work EssayDokument12 SeitenCourse Work EssayKanza NajamNoch keine Bewertungen
- Lista de Lucrari 3Dokument30 SeitenLista de Lucrari 3Anonymous 0epuGwQTJNoch keine Bewertungen
- Middle-Range Theory of Chronic Sorrow: A Framework for Understanding Recurring GriefDokument6 SeitenMiddle-Range Theory of Chronic Sorrow: A Framework for Understanding Recurring GriefRizkia100% (2)
- Adrenal Cortex Disease and PhaeochromocytomasDokument47 SeitenAdrenal Cortex Disease and PhaeochromocytomasJamaluddin Ahmad A.MNoch keine Bewertungen
- Intravenous PyelogramDokument23 SeitenIntravenous Pyelogramrachael100% (1)
- Msds Control KimiaDokument16 SeitenMsds Control KimiaEny Sucitrayati SucitrayatiNoch keine Bewertungen
- The Digestive System AvrDokument29 SeitenThe Digestive System AvrMatthew Benoza ARCEGANoch keine Bewertungen
- Imaging Classification of Vascular MalformationsDokument16 SeitenImaging Classification of Vascular MalformationsHector Hernandez-SoriaNoch keine Bewertungen
- Healthmedicinet I 2017 3Dokument667 SeitenHealthmedicinet I 2017 3tuni santeNoch keine Bewertungen
- Uveal Coloboma: The Related SyndromesDokument3 SeitenUveal Coloboma: The Related Syndromeslavinia diaNoch keine Bewertungen
- مجلة توفيقTJMSDokument89 Seitenمجلة توفيقTJMSTaghreed Hashim al-NoorNoch keine Bewertungen
- Ultrasound in Obstetrics and Gynaecology: ReviewDokument9 SeitenUltrasound in Obstetrics and Gynaecology: ReviewGustina Maryanti MooyNoch keine Bewertungen
- Herpetiform Pemphigus: Courtesy, Ronald P Rapini, MDDokument1 SeiteHerpetiform Pemphigus: Courtesy, Ronald P Rapini, MDCristian QuitoNoch keine Bewertungen
- Kingfisher Business CupcakesDokument14 SeitenKingfisher Business Cupcakesjeffrey A. FerrerNoch keine Bewertungen
- Who Edl 2018 PDFDokument30 SeitenWho Edl 2018 PDFanggoenzNoch keine Bewertungen
- Breast MRIDokument170 SeitenBreast MRICosas CuponaticNoch keine Bewertungen
- Puberdade PrecoceDokument12 SeitenPuberdade PrecoceCaio AlvesNoch keine Bewertungen
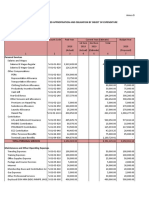
- Programmed Appropriation and Obligation by Object of ExpenditureDokument7 SeitenProgrammed Appropriation and Obligation by Object of ExpenditureKristin Villaseñor-MercadoNoch keine Bewertungen
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (13)