Das könnte Ihnen auch gefallen
- Management of Orbital FracturesDokument12 SeitenManagement of Orbital FracturesMarisol Gallego DuqueNoch keine Bewertungen
- Cholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandCholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Soft Tissue Injuries of The Head andDokument43 SeitenSoft Tissue Injuries of The Head anddeneke100% (1)
- Operative Techniques in Otolaryngology - Head and Neck Surgery, Volume 19, Issue 2, Pages 79-160 (June 2008), Management of Facial TraumaDokument89 SeitenOperative Techniques in Otolaryngology - Head and Neck Surgery, Volume 19, Issue 2, Pages 79-160 (June 2008), Management of Facial TraumaMarianaNoch keine Bewertungen
- Panfacial FracturesDokument14 SeitenPanfacial FracturesAlejandra AguirreNoch keine Bewertungen
- OMS Resident ManualDokument84 SeitenOMS Resident ManualTaufiqurrahman Abdul DjabbarNoch keine Bewertungen
- Approaches To Frontal SinusDokument77 SeitenApproaches To Frontal SinusHossam Elden Helmy HaridyNoch keine Bewertungen
- Basic Principles of RhinoplastyDokument21 SeitenBasic Principles of Rhinoplastydrbantm100% (2)
- Excision of Preauricular Pits and SinusesDokument7 SeitenExcision of Preauricular Pits and SinusesHNoch keine Bewertungen
- Ballengers Manual of Otorhinolaryngology PDFDokument858 SeitenBallengers Manual of Otorhinolaryngology PDFIrma Sari MuliadiNoch keine Bewertungen
- Neligan Vol 3 Chapter 03 MainDokument55 SeitenNeligan Vol 3 Chapter 03 MainisabelNoch keine Bewertungen
- Surgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDokument4 SeitenSurgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDwarika Prasad BajgaiNoch keine Bewertungen
- Plastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic SurgeryDokument23 SeitenPlastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic SurgeryTugce InceNoch keine Bewertungen
- Ent Case 2Dokument29 SeitenEnt Case 2Trina CardonaNoch keine Bewertungen
- Post Graduate Degree Standard Paper - I CodeDokument7 SeitenPost Graduate Degree Standard Paper - I CodeFZ icebladeNoch keine Bewertungen
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- The Erlangen Salivary Gland Project: Part I: Sialendoscopy in Obstructive Diseases of The Major Salivary GlandsDokument60 SeitenThe Erlangen Salivary Gland Project: Part I: Sialendoscopy in Obstructive Diseases of The Major Salivary GlandsRosa Silva100% (1)
- Septum Surgery: DR Faıza FarahDokument45 SeitenSeptum Surgery: DR Faıza Farahismail mohamed aliNoch keine Bewertungen
- Benign Skin LesionsDokument75 SeitenBenign Skin LesionsEmma Enggar SafitriNoch keine Bewertungen
- 05 04 06 Cerebrospinal Fluid RhinorrheaDokument53 Seiten05 04 06 Cerebrospinal Fluid RhinorrheaiachapraNoch keine Bewertungen
- Open SeptorhinoplastyDokument6 SeitenOpen SeptorhinoplastybarbiemeNoch keine Bewertungen
- InterMod OMFSDokument36 SeitenInterMod OMFSFahad Qiam75% (4)
- Otoscopy Findings 18Dokument193 SeitenOtoscopy Findings 18Consulta Médica AriasNoch keine Bewertungen
- Endoscopic DacryocystorhinostomyDokument17 SeitenEndoscopic Dacryocystorhinostomyapi-19500641Noch keine Bewertungen
- Endoscopic Anatomy of Nose and PNS FinalDokument98 SeitenEndoscopic Anatomy of Nose and PNS FinalRahul Kurkure100% (2)
- Atlas of Operative Maxillofacial Trauma Surgery Primary Repair of Facial Injuries (UnitedVRG)Dokument834 SeitenAtlas of Operative Maxillofacial Trauma Surgery Primary Repair of Facial Injuries (UnitedVRG)Ahmad YNoch keine Bewertungen
- Branchial Cleft CystsDokument8 SeitenBranchial Cleft CystsHere LeafsNoch keine Bewertungen
- Facial NerveDokument68 SeitenFacial NerveMédecin Adrian TGNoch keine Bewertungen
- Headand NeckNeck and Head RadiologyDokument69 SeitenHeadand NeckNeck and Head RadiologyvsignatureNoch keine Bewertungen
- Basic FESS - Step-By-Step Guide With Surgical Videos PDFDokument20 SeitenBasic FESS - Step-By-Step Guide With Surgical Videos PDFMujeeb MohammedNoch keine Bewertungen
- CholesteatomaDokument29 SeitenCholesteatomawhitelotusoo7Noch keine Bewertungen
- Rhinolith: A Forgotten Identity-Series of 18 Cases With Review of LiteratureDokument5 SeitenRhinolith: A Forgotten Identity-Series of 18 Cases With Review of LiteratureGustamas Indra MaulanaNoch keine Bewertungen
- Endoscopic and Sinus CX ManualDokument136 SeitenEndoscopic and Sinus CX ManualAlejandra Oliveros VargasNoch keine Bewertungen
- Endoscopic Dacryocystorhinostomy - DCR - Surgical TechniqueDokument11 SeitenEndoscopic Dacryocystorhinostomy - DCR - Surgical TechniqueLuis De jesus SolanoNoch keine Bewertungen
- ورق مذاكره PDFDokument100 Seitenورق مذاكره PDFsalamred100% (1)
- Fellowships in OtolaryngologyDokument17 SeitenFellowships in OtolaryngologyasiyazaidiaNoch keine Bewertungen
- Head and Neck Surgical Anatomy FlyerDokument2 SeitenHead and Neck Surgical Anatomy FlyerMary BassNoch keine Bewertungen
- Impedance Audiometry - Overview, Indications, ContraindicationsDokument8 SeitenImpedance Audiometry - Overview, Indications, ContraindicationsSorin AilincaiNoch keine Bewertungen
- Surgery For Pharyngeal Pouch or Zekers DivertulaDokument19 SeitenSurgery For Pharyngeal Pouch or Zekers DivertulaKumaran Bagavathi RagavanNoch keine Bewertungen
- Grand Rounds Facial Nerve ParalysisDokument86 SeitenGrand Rounds Facial Nerve ParalysisA170riNoch keine Bewertungen
- PNS RSO LectureDokument40 SeitenPNS RSO LectureIvan de GranoNoch keine Bewertungen
- SialendosDokument60 SeitenSialendoshwalijeeNoch keine Bewertungen
- Bailey CH 9 144-155. CH 7 1-18 2Dokument62 SeitenBailey CH 9 144-155. CH 7 1-18 2laringfaring updateNoch keine Bewertungen
- Neck Mass ProtocolDokument8 SeitenNeck Mass ProtocolCharlene FernándezNoch keine Bewertungen
- Temporal Bone Dissection ManualDokument15 SeitenTemporal Bone Dissection Manualabhi2537100% (1)
- Paranasal Sinuses: Anatomy and FunctionDokument49 SeitenParanasal Sinuses: Anatomy and FunctionYoel Lia NieNoch keine Bewertungen
- Cleft Lip and Palate Management: A Comprehensive AtlasVon EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNoch keine Bewertungen
- Atlas of Topographical and Pathotopographical Anatomy of the Head and NeckVon EverandAtlas of Topographical and Pathotopographical Anatomy of the Head and NeckNoch keine Bewertungen
- Maxilofacial AoDokument239 SeitenMaxilofacial AoGustavo BermeoNoch keine Bewertungen
- Congenital Aural AtresiaDokument30 SeitenCongenital Aural Atresiaalrafeek1050Noch keine Bewertungen
- Otosclerosis Slides 061018Dokument96 SeitenOtosclerosis Slides 061018Paraguay De La Cruz JoelNoch keine Bewertungen
- Bailey's 5th Ed (2014) - Ossicular RekonstruksiDokument12 SeitenBailey's 5th Ed (2014) - Ossicular RekonstruksiMei Risanti SiraitNoch keine Bewertungen
- Preservation Rhinoplasty ProgrammeDokument11 SeitenPreservation Rhinoplasty ProgrammeSaad LahmitiNoch keine Bewertungen
- Complications of Sinus Surgery SariDokument38 SeitenComplications of Sinus Surgery SariFebryantiPBundaayabariqNoch keine Bewertungen
- Ent Manifestations of Systemic DiseasesDokument10 SeitenEnt Manifestations of Systemic DiseasesSuresh Ambi100% (1)
- Microvascular Free Flaps Used in Head and Neck Reconstruction. / Orthodontic Courses by Indian Dental AcademyDokument97 SeitenMicrovascular Free Flaps Used in Head and Neck Reconstruction. / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- FESS Instrument Set Brochure W7053245Dokument4 SeitenFESS Instrument Set Brochure W7053245Selvi YapNoch keine Bewertungen
- Ear, Nose and Throat emerg-ENT-cies: With Laura WilkinsDokument43 SeitenEar, Nose and Throat emerg-ENT-cies: With Laura WilkinsIrina AndreeaNoch keine Bewertungen
- Juvenile Nasopharyngial AngiofibromaDokument8 SeitenJuvenile Nasopharyngial AngiofibromaDr-Firas Nayf Al-ThawabiaNoch keine Bewertungen
- 02a MRCS ENT RegulationsDokument3 Seiten02a MRCS ENT RegulationsAravind NooneyNoch keine Bewertungen
- Orbital Decompression, Optic N Decompression and EndoDCRDokument97 SeitenOrbital Decompression, Optic N Decompression and EndoDCRAlok RathiNoch keine Bewertungen
- Septal Extension Graft ArticlesDokument7 SeitenSeptal Extension Graft Articlesjose orlando sturla pelleranoNoch keine Bewertungen
- Management of Congenital Aural AtresiaDokument22 SeitenManagement of Congenital Aural AtresiamelaniNoch keine Bewertungen
- Head and Neck Cancer Care in a Pandemic: Prioritizing Safe CareVon EverandHead and Neck Cancer Care in a Pandemic: Prioritizing Safe CareNoch keine Bewertungen
- Essential Tissue Healing of the Face and NeckVon EverandEssential Tissue Healing of the Face and NeckBewertung: 5 von 5 Sternen5/5 (2)
- Clinical Spectrum of Disorders of Sexual Differentiation: Original ArticleDokument5 SeitenClinical Spectrum of Disorders of Sexual Differentiation: Original ArticleInne CarolineNoch keine Bewertungen
- WHO MC - Manual - 2018 PDFDokument403 SeitenWHO MC - Manual - 2018 PDFchimbimbNoch keine Bewertungen
- Triangular FlapDokument5 SeitenTriangular FlapInne CarolineNoch keine Bewertungen
- Journal Recent Advances in Management of Maxillofacial TraumaDokument9 SeitenJournal Recent Advances in Management of Maxillofacial TraumaPrazna ShafiraNoch keine Bewertungen
- Jeyaraj 2018Dokument16 SeitenJeyaraj 2018shagun singhNoch keine Bewertungen
- Oral Surgery II. Part 6. Oral Maxillofacial TraumaDokument7 SeitenOral Surgery II. Part 6. Oral Maxillofacial TraumaMuzna AftabNoch keine Bewertungen
- Blueprints - Radiology PDFDokument134 SeitenBlueprints - Radiology PDFBenny KMNoch keine Bewertungen
- Pebrian21001@mail Unpad Ac IdDokument7 SeitenPebrian21001@mail Unpad Ac Idbahasa inggris1Noch keine Bewertungen
- 1.13 Lefort Fracturas. Facial Trauma Surgery PDFDokument21 Seiten1.13 Lefort Fracturas. Facial Trauma Surgery PDFMonica Posso ZapataNoch keine Bewertungen
- نموذج الامتيازات السريريةDokument67 Seitenنموذج الامتيازات السريريةSAFA ALYNoch keine Bewertungen
- MDS DenistryDokument34 SeitenMDS Denistrysherani999Noch keine Bewertungen
- Panfacial Fractures: Kiran S. Gadre, Balasubramanya Kumar, and Divya P. GadreDokument20 SeitenPanfacial Fractures: Kiran S. Gadre, Balasubramanya Kumar, and Divya P. Gadre19-2 W. RIFQA NURFAIDAHNoch keine Bewertungen
- Ristow 2014Dokument8 SeitenRistow 2014Glaciele Maria de SouzaNoch keine Bewertungen
- 6 Middle Facial FracturesDokument29 Seiten6 Middle Facial FracturesYoussef ElbeharyNoch keine Bewertungen
- CT MXFDokument6 SeitenCT MXFAhmed KhattabNoch keine Bewertungen
- Injuries of Maxillofacial and ManagementDokument120 SeitenInjuries of Maxillofacial and Managementdisha 146jandialNoch keine Bewertungen
- Case StudyDokument15 SeitenCase StudyMuhamad XalefaNoch keine Bewertungen
- Facial InjuryDokument40 SeitenFacial Injuryahmad iffa maududyNoch keine Bewertungen
- Facial and Mandibular FracturesDokument24 SeitenFacial and Mandibular FracturesahujasurajNoch keine Bewertungen
- Anaesthetic Challenges in Complex Maxillofacial Trauma - ADokument18 SeitenAnaesthetic Challenges in Complex Maxillofacial Trauma - APraveen RamasamyNoch keine Bewertungen
- Basic Management of - Maxillofacial Trauma1Dokument26 SeitenBasic Management of - Maxillofacial Trauma1Pratikshya KothiaNoch keine Bewertungen
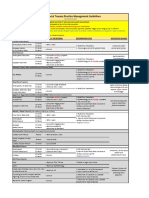
- VUMC Facial Trauma Practice Management GuidelinesDokument1 SeiteVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoNoch keine Bewertungen
- Practical Trends in Anesthesia and Intensive Care 2017Dokument202 SeitenPractical Trends in Anesthesia and Intensive Care 2017Edina KacsoNoch keine Bewertungen
- Maxillofacial TraumaDokument15 SeitenMaxillofacial TraumadewiswahyuNoch keine Bewertungen
- Facial Butress SystemDokument2 SeitenFacial Butress SystemlilaningNoch keine Bewertungen
- Log Book New Dental Officer Programme (Ndop) Ministry of Health MalaysiaDokument21 SeitenLog Book New Dental Officer Programme (Ndop) Ministry of Health MalaysiaKuruNoch keine Bewertungen
- Management of Orbital Floor Fractures: An Oculoplastic Surgeon's ViewDokument6 SeitenManagement of Orbital Floor Fractures: An Oculoplastic Surgeon's ViewTejkiran ShettyNoch keine Bewertungen