Beruflich Dokumente
Kultur Dokumente
Mortality After Incident Cancer in People With and Without Type 2 Diabetes
Hochgeladen von
Walida FadillahOriginaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Mortality After Incident Cancer in People With and Without Type 2 Diabetes
Hochgeladen von
Walida FadillahCopyright:
Verfügbare Formate
Epidemiology/Health Services Research
O R I G I N A L A R T I C L E
Mortality After Incident Cancer in People
With and Without Type 2 Diabetes
Impact of metformin on survival
CRAIG J. CURRIE, PHD1 EDWIN A.M. GALE, MD3 growth of cancer cells, including reducing
CHRIS D. POOLE, PHD2 JEFFREY A. JOHNSON, PHD4 the concentration of circulating insulin,
SARA JENKINS-JONES, MSC2 CHRISTOPHER Ll. MORGAN, MSC
2
inducing apoptosis, and activating meta-
bolic pathways such as LKB1/AMP-activated
protein kinase (AMPK) (12). However,
OBJECTIVEdType 2 diabetes is associated with an increased risk of several types of cancer there are concerns about confounding by
and with reduced survival after cancer diagnosis. We examined the hypotheses that survival indication because metformin-treated
after a diagnosis of solid-tumor cancer is reduced in those with diabetes when compared with
those without diabetes, and that treatment with metformin influences survival after cancer di-
patients have different clinical character-
agnosis. istics than other diabetes-related treat-
ment groups, such as those treated with
RESEARCH DESIGN AND METHODSdData were obtained from .350 U.K. primary insulin. Metformin is now recommended
care practices in a retrospective cohort study. All individuals with or without diabetes who as the first-line treatment for all patients
developed a first tumor after January 1990 were identified and records were followed to Decem- with type 2 diabetes, and is also under
ber 2009. Diabetes was further stratified by treatment regimen. Cox proportional hazards models consideration for use in nondiabetic pa-
were used to compare all-cause mortality from all cancers and from specific cancers. tients as an adjunctive therapy for can-
RESULTSdOf 112,408 eligible individuals, 8,392 (7.5%) had type 2 diabetes. Cancer mor- cer. There is therefore an urgent need to
tality was increased in those with diabetes, compared with those without (hazard ratio 1.09 [95% understand its potential effect on cancer
CI 1.06–1.13]). Mortality was increased in those with breast (1.32 [1.17–1.49]) and prostate prognosis.
cancer (1.19 [1.08–1.31]) but decreased in lung cancer (0.84 [0.77–0.92]). When analyzed by This study aimed to characterize pat-
diabetes therapy, mortality was increased relative to nondiabetes in those on monotherapy with terns of survival after incident cancer in
sulfonylureas (1.13 [1.05–1.21]) or insulin (1.13 [1.01–1.27]) but reduced in those on metfor- people with type 2 diabetes, compare
min monotherapy (0.85 [0.78–0.93]). these with survival patterns in the nondia-
CONCLUSIONSdThis study confirmed that type 2 diabetes was associated with poorer betic population, and, in particular, de-
prognosis after incident cancer, but that the association varied according to diabetes therapy termine if postcancer survival was related
and cancer site. Metformin was associated with survival benefit both in comparison with other to the type of medication used to treat
treatments for diabetes and in comparison with a nondiabetic population. diabetes.
Diabetes Care 35:299–304, 2012
RESEARCH DESIGN AND
METHODS
C
ertain types of cancers are more diabetes may respond less effectively to
common in people with diabetes some cancer therapies, or that they may Data and subjects
than in those without (1–3), and di- tolerate them less well. Anonymous, routine data compiled from
abetes is also associated with reduced sur- Patients who take metformin for type .350 primary care practices in the U.K.
vival after cancer (4,5). Interpretation of 2 diabetes have a lower overall risk of were analyzed in a retrospective cohort
these observations is, however, con- cancer and lower cancer mortality than study. Available data included patient de-
founded by the greater comorbidity and those on other glucose-lowering therapies mographics, medical history (including di-
reduced life expectancy associated with (9–11). This finding has emerged consis- agnoses and health contacts), biochemistry
diabetes, and by the possibility that those tently from both randomized and obser- and microbiology test results, and pharma-
with diabetes may have less effective can- vational studies, and a number of ceutical prescriptions. Ethnicity was recorded
cer screening (6–8), leading to delayed di- mechanisms have been proposed by sparsely for general practice locality but
agnosis. It is also possible that people with which metformin might suppress the not at all for individuals and is therefore
not included in our study. Diagnostic in-
c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c formation was recorded using the Read
From the 1Department of Primary Care and Public Health, School of Medicine, Cardiff University, Cardiff, U.K.; code classification, used throughout gen-
2
Global Epidemiology, Pharmatelligence, Cardiff, U.K.; 3Diabetes and Metabolism, School of Clinical eral practice in the U.K. (13).
Sciences, University of Bristol, Bristol, U.K.; and the 4School of Public Health, University of Alberta, Ed-
monton, Alberta, Canada.
Corresponding author: Craig J. Currie, currie@cardiff.ac.uk. Observational time periods
Received 13 July 2011 and accepted 28 October 2011. Subjects were selected from practices
DOI: 10.2337/dc11-1313 from 1990, or from the date of the
This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10 practice’s acceptable mortality ratio,
.2337/dc11-1313/-/DC1.
© 2012 by the American Diabetes Association. Readers may use this article as long as the work is properly whichever was later. The acceptable mor-
cited, the use is educational and not for profit, and the work is not altered. See http://creativecommons.org/ tality ratio ensures that the mortality pat-
licenses/by-nc-nd/3.0/ for details. terns reported by practices are as expected
care.diabetesjournals.org DIABETES CARE, VOLUME 35, FEBRUARY 2012 299
Cancer mortality in type 2 diabetes
based on the application of national mor- cancer diagnosis and those with hemato- cancer-specific sites: breast, prostate, color-
tality statistics. This helps remove the po- logical cancers prior to the solid tumor ectum, lung, bladder, ovary/endometrium,
tential bias from a survivor effect. The final were excluded. pancreas, and liver, selected because of
observation was in December 2009. In order to examine the impact of their high frequency or their identification
A minimum wash-in period of 2 years selected glucose-lowering therapies, sub- as a cancer of particular interest in the
from general practice registration to can- jects with type 2 diabetes were further diabetic population.
cer diagnosis was used to ensure that the subdivided by selected regimens at cancer Kaplan-Meier analysis was used to
identified cancer was the first cancer oc- diagnosis: metformin, sulfonylurea, and estimate mean and median survival. Cox
currence. Subjects’ records were followed insulin monotherapy. Patients were clas- proportional hazards models were used
over time and were censored due to death, sified into these monotherapy groups by to account for differences in cohort char-
departure from the general practice, or 31 their treatment in the 90 days before their acteristics. The reference group was the
December 2009, whichever occurred cancer diagnosis. A sensitivity analysis nondiabetic group for all analyses other
first. considered only those people treated with than those limited to the diabetic popu-
these specific monotherapy regimens lation, where the reference group was
Patient selection 90 days after cancer diagnosis. In all cases, metformin monotherapy. The specifica-
Selection was based upon a first diagnosis monotherapy with glucose-lowering tion of the baseline Cox model included
of a solid tumor. Cancer diagnoses recorded therapies was indicated by a time-fixed, three covariates: age, sex, and smoking
in general practice routine data in the binary covariate. status, before the addition of other cova-
U.K. have been empirically validated and riates. Comorbidity was classified using the
have a high positive predictive value (14). Data analysis Charlson index (15), adapted in order to
Diabetes was identified by a Read code The primary outcome measure was all- exclude diabetes and the index cancer as
indicative of diabetes and was flagged as cause mortality. The data lacked sufficient predictor variables. Additional covariates
type 1 or type 2 diabetes. Type 1 diabetes detail to capture cancer-specific mortality included year of cancer diagnosis, Town-
was subsequently excluded from all anal- accurately. The analysis was first applied send index of deprivation, HbA1c, and the
yses. Individuals aged ,35 years at to all cancers and then replicated for number of general practice contacts, which
Table 1dBaseline characteristics of cohorts at cancer diagnosis
Type 2 diabetes treatment groups
Type 2 Insulin
Nondiabetes diabetes Met mono Sulf mono mono Met + Sulf Met + insulin
Patients, n (%) 104,016 8,392 1,428 (17.0) 1,519 (18.1) 654 (7.8) 1,125 (13.4) 290 (3.5)
Follow-up, total (median), years 353,056 (2.0) 22,037 (1.6) 3,794 (1.8) 4,351 (1.6) 1,699 (1.5) 3,221 (1.9) 605 (1.3)
Age, mean (SD), years 67.5 (13.0) 71.7 (9.5) 70.4 (9.8) 74.1 (8.9) 70.4 (9.4) 71.9 (8.8) 67.8 (8.7)
Sex
Male, n (%) 49,146 (47.2) 4,940 (58.9) 791 (55.4) 918 (60.4) 379 (58.0) 688 (61.2) 163 (56.2)
Female, n (%) 54,870 (52.8) 3,452 (41.1) 637 (44.6) 601 (39.6) 275 (42.0) 437 (38.8) 127 (43.8)
Smoking
Current, n (%) 22,207 (21.3) 1,341 (16.0) 241 (16.9) 248 (16.3) 113 (17.3) 163 (14.5) 43 (14.8)
Ex, no. (%) 24,422 (23.5) 3,129 (37.3) 541 (37.9) 505 (33.2) 249 (38.1) 418 (37.2) 126 (43.4)
Diabetes duration, mean (SD),
years N/A 7.7 (7.0) 5.3 (5.5) 6.9 (5.9) 12.8 (8.6) 9.2 (6.7) 13.5 (7.4)
BMI, mean (SD), kg/m2 25.9 (4.3) 29.4 (5.1) 30.7 (5.1) 27.7 (4.5) 28.9 (5.1) 29.4 (4.8) 31.6 (5.3)
Systolic BP, mean (SD), mmHg 139.6 (19.8) 138.6 (19.3) 137.8 (18.3) 140.7 (21.0) 139.4 (19.9) 138.9 (17.9) 137.9 (17.6)
Cholesterol, mean (SD), mmol/L 5.1 (1.2) 4.4 (1.1) 4.3 (1.1) 4.5 (1.2) 4.3 (1.1) 4.3 (1.1) 4.1 (1.0)
HbA1c, mean (SD), % N/A 7.4 (1.5) 7.1 (1.3) 7.4 (1.5) 8.4 (1.6) 7.7 (1.5) 8.3 (1.5)
Other morbidity
Large vessel disease, n (%) 15,787 (15.2) 2,665 (31.8) 393 (27.5) 513 (33.8) 265 (40.5) 359 (31.9) 104 (35.9)
Renal disease, n (%) 964 (0.9) 628 (7.5) 87 (6.1) 127 (8.4) 75 (11.5) 75 (6.7) 22 (7.6)
Primary care contacts preceding
year, mean (SD) 7.0 (6.9) 11.2 (9.5) 10.8 (9.0) 10.3 (9.1) 13.6 (11.7) 10.8 (8.8) 12.6 (9.6)
Charlson index, mean (SD) 2.5 (0.9) 4.2 (1.4) 3.9 (1.2) 4.2 (1.5) 4.9 (1.7) 4.2 (1.3) 4.5 (1.5)
Charlson index (age adjusted),
mean (SD) 4.8 (1.8) 6.9 (1.8) 6.5 (1.7) 7.2 (1.9) 7.4 (2.0) 7.0 (1.7) 6.8 (1.8)
Charlson index (adjusted*),
mean (SD) 0.5 (0.8) 0.8 (1.1) 0.6 (0.9) 0.9 (1.1) 1.1 (1.3) 0.8 (1.0) 0.8 (1.0)
Townsend index of deprivation,
mean (SD) 2.7 (1.4) 2.9 (1.4) 2.9 (1.4) 2.9 (1.4) 2.9 (1.3) 2.8 (1.4) 2.9 (1.4)
Met, metformin; mono, monotherapy; Sulf, sulfonylurea. *Index adjusted to exclude diabetes and the index cancer.
300 DIABETES CARE, VOLUME 35, FEBRUARY 2012 care.diabetesjournals.org
Currie and Associates
was log transformed because of severe
KPY, per thousand patient-years. *Cox model specification: age at baseline, sex, smoking history, Charlson comorbidity index, and year of diagnosis.
Other
Prostate
Pancreas
Ovary/endometrium
Lung
Liver
Colorectal
Breast
Bladder
Overall
Cancer site
Table 2dUnadjusted mean and median survival from time of cancer diagnosis and adjusted* relative mortality, by cancer site
skewed distribution.
The threshold for statistical signifi-
cance was set at the conventional level of
a = 0.05, and 95% CIs for hazard ratios
(HRs) were calculated. Records with miss-
ing data were excluded automatically in the
respective models. We tested the propor-
104,016 42,602 120.7
25,507 11,727 143.8
11,611 8,916 870.9
13,388 5,742 136.8
24,393 4,796
15,256 4,894
Cases
tional hazards assumption for the Cox
1,944 1,532 1,343.6
4,732 1,832 111.9
1,217
5,968 2,287 102.5
models by examining the Pearson correla-
tion between Schoenfeld residuals and the
Deaths n/PKPY Mean (95% CI), years Median (SE), years Cases Deaths n/PKPY Mean (95% CI), years Median (SE), years
rank of survival time for cases that pro-
876 742.0
gressed to an event (16).
RESULTS
38.8
89.3
Subjects and baseline
No diabetes
14.3 (14.1–14.4)
characteristics
8.6 (8.4–8.7)
9.1 (8.8–9.3)
1.2 (1–1.4)
9.9 (9.6–10.3)
1.8 (1.7–1.9)
2.4 (2.0–2.8)
8.6 (8.4–8.8)
9.4 (9.1–9.7)
9.5 (9.4–9.5)
Data were available for 112,602 people
with solid tumors. Of these, 194 (0.2%)
had type 1 diabetes and were excluded.
Of the remaining 112,408 subjects, 8,392
(7.5%) had type 2 diabetes. Table 1 shows
the baseline characteristics by nondiabe-
tes and diabetes and by subsets of glu-
cose-lowering therapy at the time of
19.6 (0.4)
5.2 (0.2)
7.9 (0.1)
0.3 (0.0)
7.9 (0.5)
0.5 (0.0)
0.5 (0.0)
5.5 (0.2)
7.8 (0.3)
7.1 (0.9)
cancer diagnosis.
Those with type 2 diabetes were older
(71.7 years, SD 9.5, vs. 67.5 years, SD 13.0;
P , 0.001), more likely to be male (58.9 vs.
47.2%; P , 0.001), and had greater base-
2,008 1,005 208.0
1,385
1,285
1,182
8,392 3,780 171.5
364
394
856
243
675
line morbidity, whether measured in terms
of vascular disease (31.8 vs. 15.2%; P ,
0.001), prior general practice contacts
465 105.5
288 1,184.1
136 112.7
595 689.2
163 661.0
532 147.5
328
268 113.4
(11.2 vs. 7.0%; P , 0.001), or the Charlson
index after adjusting for age (6.9 vs. 4.8
units; P , 0.001), when compared with
76.9
the nondiabetic group. Those with type 2
diabetes had a higher BMI (29.4 vs. 25.9
Type 2 diabetes
kg/m2; P , 0.001), but other modifiable
10.4 (9.5–11.3)
6.1 (5.6–6.5)
7.5 (6.9–8.0)
1.1 (0.8–1.3)
8.6 (7.3–9.8)
2.2 (1.8–2.6)
2.4 (1.5–3.2)
7.3 (6.6–8)
8.3 (7.5–9.1)
7.0 (6.7–7.3)
risk factors were more favorable; for exam-
ple, the proportion of current smokers
(16.0 vs. 21.3%; P , 0.001) and choles-
terol (4.4 vs. 5.1 mmol/L; P , 0.001).
There were also differences in baseline
characteristics between diabetes-related
treatment regimens. For example, 40% of
people treated with insulin-only regimens
3.2 (0.3)
6.7 (0.2)
0.3 (0.0)
8.4 (0.9)
0.7 (0.0)
0.7 (0.1)
6.2 (0.4)
4.6 (0.1)
5.1 (0.3)
9.4 (0.8)
were found to have a record of large vessel
disease at cancer diagnosis versus 27% of
those treated with metformin monotherapy
(P , 0.001) (Table 1).
1.32 (1.17–1.49)
1.19 (1.08–1.31)
0.98 (0.86–1.12)
0.87 (0.72–1.04)
0.84 (0.77–0.92)
0.88 (0.74–1.05)
1.00 (0.91–1.10)
1.16 (1.02–1.32)
1.24 (1.20–1.29)
Adjusted relative mortality
Overall mortality
HR (95% CI)
The median (SE) and mean (95% CI)
for overall survival were 6.8 (0.08) and
d
9.3 years (9.2–9.4), respectively. There
was a significant difference in the unad-
justed, overall hazard of mortality in peo-
ple with diabetes versus nondiabetes (HR
,0.001
,0.001
,0.001
0.001
0.764
0.120
0.157
0.992
0.027
d
1.24 [95% CI 1.20–1.29]) (Supplemen-
P
tary Fig. 1A). After the inclusion of other
care.diabetesjournals.org DIABETES CARE, VOLUME 35, FEBRUARY 2012 301
Cancer mortality in type 2 diabetes
When comparing different mono-
therapies in patients with diabetes, those
receiving sulfonylurea monotherapy (HR
1.48 [1.29–1.71]) or insulin alone (1.33
[1.18–1.58]) had significantly increased
mortality relative to metformin monother-
apy. The combination therapies metformin
and sulfonylurea (1.09 [0.94–1.27]) and
insulin and metformin (1.28 [0.96–1.64])
were not significant.
In site-specific analysis, reduced mor-
tality was observed in subjects treated
with metformin monotherapy at the time
of diagnosis for liver (HR 0.47 [0.24–
0.91]) and ovarian/endometrial cancer
(0.48 [0.28–0.81]), although no mortal-
ity differences were noted for the other
cancer sites (Table 3). In sensitivity analysis
considering patients treated with mono-
therapy for 90 days after a cancer diagnosis,
significant differences were noted for lung
(0.77 [0.59–1.00]) and ovarian/endometrial
cancer (0.42 [0.23–0.77]).
CONCLUSIONSdWe set out to de-
termine whether a diagnosis of solid-
tumor cancer was associated with shorter
survival in people with type 2 diabetes
when compared with those without di-
abetes, and whether metformin influ-
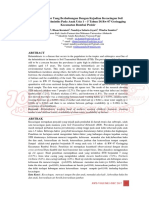
Figure 1dAdjusted* survival using alternative diabetes-related treatment regimens: mono- enced this. The study confirmed that
therapy within 90 days of cancer diagnosis. Note: the patterns of survival in the insulin and survival was reduced in those with di-
sulfonylurea groups are the same. *Cox model specification: age, sex, smoking status, year of abetes after a diagnosis of cancer. After
cancer diagnosis, and Charlson comorbidity index. controlling for confounding factors, type
2 diabetes was associated with an ;10%
increase in mortality for all cancers in
comparison with those who did not
variables into the model (age at baseline, mortality in patients with breast (HR have diabetes. This observation should,
sex, smoking status, Charlson index, and 1.32 [1.17–1.49]) or prostate cancer however, be considered with some cau-
year of cancer diagnosis), the HR re- (HR 1.19 [1.08–1.31]) compared with tion because the increased mortality may
mained significant at 1.10 (1.07–1.14) those without diabetes. Conversely, di- have been related to the diabetes rather
(Supplementary Fig. 1F). BMI was signif- abetes was associated with improved than to the cancer. When prognosis was
icant in the model, although it had no lung cancer survival compared with examined by cancer type, bladder, breast,
meaningful impact on the other HRs, but those without diabetes (HR 0.84 [0.77– and prostate cancers were associated with
was excluded from the analysis because of 0.92]). diminished survival. The increased mor-
missing data, which disproportionately af- tality for breast cancer confirms previous
fected the nondiabetic group. When the Mortality by glucose-lowering data reporting a significant HR of 1.4 for
models were run with BMI included, there therapy those with diabetes versus those without
was no impact upon the HRs for diabetes People with diabetes receiving metformin (11). Here, however, diabetes was associated
versus nondiabetes. monotherapy for 90 days before cancer with slightly longer survival from lung can-
diagnosis had significantly reduced over- cer (1.8 vs. 2.2 years).
Mortality by cancer site all mortality (HR 0.85 [0.78–0.93]), The study also showed that metfor-
Mortality differences by diabetes status var- compared with those without diabetes min therapy in the period preceding di-
ied considerably by cancer site (Table 2). (Fig. 1). In contrast, those treated with agnosis was associated with a better
For example, women with breast cancer sulfonylurea monotherapy (1.13 [1.05– prognosis after a diagnosis of cancer,
had a mean survival time of 10.4 years 1.21]) or insulin alone (1.13 [1.01– compared not only with other forms of
if they had diabetes, versus 14.3 years if 1.27]) had increased mortality. For diabetes therapy but also with the non-
they did not. In lung cancer, however, combination therapy, there was no sig- diabetic population.
mean survival times were 2.2 and 1.8 nificant association with mortality: met- Although these data need cautious in-
years, respectively. When adjusted using formin and insulin (1.08 [0.88–1.33]) terpretation, they suggest that exposure to
the Cox model (Table 2), diabetes was and metformin and sulfonylurea (0.91 metformin after diagnosis is associated with
associated with significantly greater [0.83–1.01]). improved survival for the majority of sites,
302 DIABETES CARE, VOLUME 35, FEBRUARY 2012 care.diabetesjournals.org
Currie and Associates
Table 3dAdjusted* survival by cancer site in people exposed versus not exposed to metformin immediately before and after
cancer diagnosis
6Metformin (immediately before cancer diagnosis) 6Metformin (#3 months after cancer diagnosis)
Cancer site Cases Deaths HR (95% CI) P Cases Deaths HR (95% CI) P
All cancer 112,408 46,382 0.899 (0.814–0.993) 0.036 94,363 33,444 0.903 (0.815–1.001) 0.054
Bladder 6,643 2,555 0.888 (0.556–1.417) 0.619 5,954 2,114 0.958 (0.643–1.426) 0.834
Breast 25,575 5,124 0.963 (0.675–1.373) 0.836 24,186 4,671 0.967 (0.695–1.345) 0.846
Colorectum 14,673 6,274 0.889 (0.666–1.187) 0.427 12,443 4,733 0.881 (0.669–1.161) 0.370
Liver 1,460 1,039 0.467 (0.241–0.906) 0.024 819 514 0.932 (0.507–1.715) 0.823
Lung 12,467 9,511 0.834 (0.665–1.045) 0.115 7,345 5,204 0.767 (0.590–0.997) 0.048
Ovary/endometrium 5,863 2,223 0.480 (0.283–0.814) 0.007 5,021 1,661 0.423 (0.233–0.767) 0.005
Pancreas 2,308 1,820 1.256 (0.853–1.849) 0.247 1,142 841 0.652 (0.381–1.114) 0.118
Prostate 16,641 5,359 1.266 (0.967–1.658) 0.086 15,480 4,819 1.232 (0.967–1.571) 0.091
Other cancers 26,778 12,477 0.894 (0.747–1.070) 0.224 21,973 8,887 0.889 (0.727–1.087) 0.252
*Cox model specification: age, sex, smoking history, Townsend index of deprivation, Charlson comorbidity index, number of primary care contacts (log trans-
formed), and year of diagnosis.
although this was only statistically signifi- of the overall diabetic population. This cre- (10%) overall difference may reflect re-
cant for cancers of the ovary/endometrium ates some difficulty in interpretation. For duced survival due to diabetes rather than a
and the lung. Interestingly, this list did not example, the observation that those on worse outcome from the cancer. We also
include breast cancer, for which metfor- metformin alone preceding a diagnosis of observed a reduced mortality in diabetic pa-
min is being studied in controlled trials as cancer had a better prognosis might indi- tients treated with metformin monotherapy
an anticancer agent. These findings add to cate that these individuals were healthier or whether before or after cancer diagnosis,
the evidence that metformin may be of better able to resist cancer than those on as compared with those on other forms of
benefit in the prevention and/or treatment other therapies. Equally, however, it therapy for diabetes. The most striking
of some, but potentially not all, types of might simply mean that they were more observation was that diabetic patients
cancer. However when used in combina- likely to have remained on long-term treated with metformin had lower mor-
tion with either sulfonylurea or insulin, metformin therapy after a diagnosis of tality than that of the background popula-
there was no significant difference in HR. cancer. Confounding by indication may tion, raising the possibility that metformin
The difference in hazard between those also, and for similar reasons, be a concern might come to play a wider role in cancer
with diabetes and those without was lower when it comes to the observed lack of prevention and therapy.
in our study than has, to our knowledge, survival benefit for those allocated to sul-
been reported previously. For example, fonylureas or insulin.
van de Poll-Franse et al. (17) reported an Other limitations include the lack of AcknowledgmentsdThis study was funded
HR of 1.4, a value that was replicated al- statistical power within some of the low- in part by the European Foundation for the
most exactly in a related meta-analysis by incidence cancers; thus, we restricted Study of Diabetes. J.A.J. is a Senior Scholar with
Barone et al. (5). This may in part be due to ourselves to analysis of metformin expo- Alberta Innovates-Health Solutions and holds a
the additional covariates used in our anal- sure as a simple binary variable. We did Canada Research Chair in Diabetes Health
ysis, but these differences do warrant fur- not have reliable data on cancer staging at Outcomes. C.J.C. has received research grants
ther investigation. diagnosis. Patients with and without di- from various health-related organizations, in-
This study had both strengths and abetes may therefore have been diagnosed cluding Astellas, Diabetes UK, the European
limitations. The most obvious strength at different stages of the condition. We Association for the Study of Diabetes, the
Engineering and Physical Sciences Research
was the large number of cancer and also did not have detailed information on Council, Ferring, GlaxoSmithKline (GSK), Lilly,
mortality events in the overall analysis. cancer treatments received, which may Medtronic, the Medical Research Council,
These data from general clinical practice have differed between those with and Merck, Pfizer, sanofi-aventis, and the National
may be considered representative of the without diabetes. Furthermore, we did Health Service, and consults for Amylin, Aryx,
general population, and the considerable not have reliable data on cause of death Astellas, Boehringer Ingelheim, Bristol-Myers
detail of the drug exposure data was also a and therefore relied on all-cause mortality Squibb, Diabetes UK, Eisel, Ferring, GSK, Ipsen,
major advantage. Analysis of drug expo- as the outcome measure. Patients may Lilly, Medtronic, Merck, Pfizer, sanofi-aventis,
sure is, however, complicated by changes therefore have died of causes other than and Takeda. C.D.P. consults for Astellas, Ferring,
in therapy, and we avoided this problem cancer, and overall mortality will clearly Lilly, Medtronic, Novo Nordisk, sanofi-aventis,
by restricting the analysis to those who be greater for patients with diabetes due and Wyeth (Pfizer). S.J.-J. and C.Ll.M. are em-
remained on monotherapy before or to associated vascular causes. This may be ployed by a research consultancy receiving
funding from pharmaceutical companies. No
after a diagnosis of cancer. In consequence, particularly pertinent for tumors with a other potential conflicts of interest relevant to
our analysis was restricted to those on long survival period. this article were reported.
monotherapy with metformin, insulin, In summary, this analysis confirms that C.J.C. contributed to discussion and wrote,
and sulfonylureas or to those treated with patients with diabetes who are diagnosed reviewed, and edited the manuscript. C.D.P.
metformin in combination with either sul- with cancer have a shorter survival relative researched data and wrote the manuscript.
fonylureas or insulin, representing ;60% to nondiabetes, but this relatively small S.J.-J. researched data and reviewed and edited
care.diabetesjournals.org DIABETES CARE, VOLUME 35, FEBRUARY 2012 303
Cancer mortality in type 2 diabetes
the manuscript. E.A.M.G. and J.A.J. reviewed a systematic review and meta-analysis. 12. Kourelis TV, Siegel RD. Metformin and
and edited the manuscript. C.Ll.M. researched JAMA 2008;300:2754–2764 cancer: new applications for an old drug.
data, contributed to discussion, and wrote the 6. Lipscombe LL, Hux JE, Booth GL. Re- Med Oncol. 8 February 2011 [Epub ahead
manuscript. C.Ll.M. is the guarantor of this duced screening mammography among of print]
work and, as such, had full access to all the women with diabetes. Arch Intern Med 13. NHS Connecting for Health. Read codes
data in the study and takes responsibility for 2005;165:2090–2095 [Internet]. Available from http://www.
the integrity of the data and the accuracy of the 7. Maruthur NM, Bolen SD, Brancati FL, connectingforhealth.nhs.uk/system-
data analysis. Clark JM. The association of obesity and sandservices/data/readcodes. Accessed 4
cervical cancer screening: a systematic May 2011
review and meta-analysis. Obesity (Silver 14. Zhang H, Hammad TA, Giovannuci E,
References Spring) 2009;17:375–381 Kang E, Christiani DC. Validation of cancer
1. Vigneri P, Frasca F, Sciacca L, Pandini G, 8. Maruthur NM, Bolen S, Brancati FL, Clark diagnoses recorded in the General Practice
Vigneri R. Diabetes and cancer. Endocr JM. Obesity and mammography: a sys- Research Database. Pharmacoepidemiol
Relat Cancer 2009;16:1103–1123 tematic review and meta-analysis. J Gen Drug Saf 2010;19(Suppl. 1):S1–S347
2. Nicolucci A. Epidemiological aspects of Intern Med 2009;24:665–677 15. Charlson ME, Pompei P, Ales KL,
neoplasms in diabetes. Acta Diabetol 9. Evans JMM, Donnelly LA, Emslie-Smith MacKenzie CR. A new method of classifying
2010;47:87–95 AM, Alessi DR, Morris AD. Metformin and prognostic comorbidity in longitudinal
3. Giovannucci E, Harlan DM, Archer MC, reduced risk of cancer in diabetic patients. studies: development and validation.
et al. Diabetes and cancer: a consensus BMJ 2005;330:1304–1305 J Chronic Dis 1987;40:373–383
report. Diabetes Care 2010;33:1674– 10. Libby G, Donnelly LA, Donnan PT, 16. Kleinbaum DG, Klein M. Survival Analysis:
1685 Alessi DR, Morris AD, Evans JMM. New A Self-Learning Text. 2nd ed. New York,
4. Lipscombe LL, Goodwin PJ, Zinman B, users of metformin are at low risk of in- NY, Springer, 2005.
McLaughlin JR, Hux JE. The impact of cident cancer: a cohort study among people 17. van de Poll-Franse LV, Houterman S,
diabetes on survival following breast with type 2 diabetes. Diabetes Care 2009; Janssen-Heijnen ML, Dercksen MW,
cancer. Breast Cancer Res Treat 2008; 32:1620–1625 Coebergh JWW, Haak HR. Less aggres-
109:389–395 11. Currie CJ, Poole CD, Gale EAM. The in- sive treatment and worse overall survival
5. Barone BB, Yeh HC, Snyder CF, et al. fluence of glucose-lowering therapies on in cancer patients with diabetes: a large
Long-term all-cause mortality in cancer cancer risk in type 2 diabetes. Diabetologia population based analysis. Int J Cancer
patients with preexisting diabetes mellitus: 2009;52:1766–1777 2007;120:1986–1992
304 DIABETES CARE, VOLUME 35, FEBRUARY 2012 care.diabetesjournals.org
Das könnte Ihnen auch gefallen
- 2011 - Metformin - Multi-Faceted Protection Against CancerDokument22 Seiten2011 - Metformin - Multi-Faceted Protection Against CancerVladDaculNoch keine Bewertungen
- Insulin and MMDokument9 SeitenInsulin and MMAkreditasi InternaNoch keine Bewertungen
- Ournal of Linical Ncology: OriginalDokument12 SeitenOurnal of Linical Ncology: OriginalHadeer EhabNoch keine Bewertungen
- Metformin and Reduced Risk of Hepatocellular Carcinoma in Diabetes With CLDDokument9 SeitenMetformin and Reduced Risk of Hepatocellular Carcinoma in Diabetes With CLDNararto PrijogoNoch keine Bewertungen
- Precision Medicine in Type 2 Diabetes: R. B. Prasad & L. GroopDokument9 SeitenPrecision Medicine in Type 2 Diabetes: R. B. Prasad & L. Groopbuat downloadNoch keine Bewertungen
- Cud BdiabetesDokument10 SeitenCud BdiabetesShitanjni WatiNoch keine Bewertungen
- Cardiovascular Safety Profile of Currently Available Diabetic DrugsDokument17 SeitenCardiovascular Safety Profile of Currently Available Diabetic Drugsvina_nursyaidahNoch keine Bewertungen
- Original ArticleDokument9 SeitenOriginal Articlepaulobrasil.ortopedistaNoch keine Bewertungen
- Incidence and Predictors of All-Cause and Site-Specific Cancer in Type 2 Diabetes: The Fremantle Diabetes StudyDokument11 SeitenIncidence and Predictors of All-Cause and Site-Specific Cancer in Type 2 Diabetes: The Fremantle Diabetes StudyKami KamiNoch keine Bewertungen
- Manejo Pte Diabetico IopDokument11 SeitenManejo Pte Diabetico Iopheiddy MendozaNoch keine Bewertungen
- Clinical and Behavioral Factors Associated With Management Outcome in Hospitalized Patients With Diabetic Foot UlcerDokument5 SeitenClinical and Behavioral Factors Associated With Management Outcome in Hospitalized Patients With Diabetic Foot UlcerIndah Nevhita LNoch keine Bewertungen
- 4 PBDokument6 Seiten4 PBAdinda RamadhantyNoch keine Bewertungen
- Personalized Cancer Care B. Wilson, UsydDokument13 SeitenPersonalized Cancer Care B. Wilson, UsydJacob BrownNoch keine Bewertungen
- 2018 A Global Overview of Precision Medicine in Type 2 DiabetesDokument12 Seiten2018 A Global Overview of Precision Medicine in Type 2 Diabetesguanyulin01Noch keine Bewertungen
- 590 FullDokument5 Seiten590 FullHafizah ZubaidiNoch keine Bewertungen
- The Case For PharmacyDokument32 SeitenThe Case For PharmacyLunar EclipseNoch keine Bewertungen
- Reusch2017 PDFDokument2 SeitenReusch2017 PDFPablo ParicahuaNoch keine Bewertungen
- Colorectal and Prostate Cancer Risk in Diabetes Metformin, An Actor Behind The SceneDokument9 SeitenColorectal and Prostate Cancer Risk in Diabetes Metformin, An Actor Behind The Scenefranciscrick69Noch keine Bewertungen
- Combination Therapy With Sulfonylureas and Metformin and The Prevention of Death in Type 2 Diabetes: A Nested Case-Control StudyDokument8 SeitenCombination Therapy With Sulfonylureas and Metformin and The Prevention of Death in Type 2 Diabetes: A Nested Case-Control StudyLyka MahrNoch keine Bewertungen
- The Influence of Metformin in The Etiology of Selected CancersDokument7 SeitenThe Influence of Metformin in The Etiology of Selected CancersMuhammad Reza IrzantoNoch keine Bewertungen
- Article 830Dokument7 SeitenArticle 830Debby Astasya AnnisaNoch keine Bewertungen
- Medical Care of Cancer Patients - (24 Diabetes and The Cancer Patient)Dokument7 SeitenMedical Care of Cancer Patients - (24 Diabetes and The Cancer Patient)martinus.urbanusNoch keine Bewertungen
- Biomolecules 11 01022Dokument25 SeitenBiomolecules 11 01022meliaaammeNoch keine Bewertungen
- Prostate InternationalDokument5 SeitenProstate InternationalayuNoch keine Bewertungen
- Type Diabetes and Multiple Myeloma The Latest Insights 2329 6917.1000e110Dokument2 SeitenType Diabetes and Multiple Myeloma The Latest Insights 2329 6917.1000e110Akreditasi InternaNoch keine Bewertungen
- Reduction in The Incidence of Type 2 Diabetes With Lifestyle Intervention or Metformin-1Dokument11 SeitenReduction in The Incidence of Type 2 Diabetes With Lifestyle Intervention or Metformin-1AlexandreNoch keine Bewertungen
- Review Metformin in Cancer: Translational ChallengesDokument13 SeitenReview Metformin in Cancer: Translational ChallengesliMvuxNoch keine Bewertungen
- Deleterious Dozen DMT2Dokument18 SeitenDeleterious Dozen DMT2cecilia zavala100% (1)
- Art:10.1007/s10552 012 0057 0Dokument11 SeitenArt:10.1007/s10552 012 0057 0chava_samsungNoch keine Bewertungen
- Fasting and Fasting Mimicking Diets in Cancer Prevention and TherapyDokument11 SeitenFasting and Fasting Mimicking Diets in Cancer Prevention and TherapyRicky FontNoch keine Bewertungen
- Piis2405803319302195 PDFDokument13 SeitenPiis2405803319302195 PDFPancho ArancibiaNoch keine Bewertungen
- Cohort 043 Niageng DzakiyahDokument14 SeitenCohort 043 Niageng Dzakiyahniageng wardaniNoch keine Bewertungen
- 2015 Article 574Dokument14 Seiten2015 Article 574La Ode Muhammad FitrawanNoch keine Bewertungen
- Am J Clin Nutr 2007 85 289sDokument4 SeitenAm J Clin Nutr 2007 85 289sthanosssNoch keine Bewertungen
- PrediabetesDokument11 SeitenPrediabetesAna MayNoch keine Bewertungen
- 10 14338 - Ijpt-22-00021 1Dokument12 Seiten10 14338 - Ijpt-22-00021 1Raul Matute MartinNoch keine Bewertungen
- Nihms 1020972Dokument11 SeitenNihms 1020972Carlos Alfredo Pedroza MosqueraNoch keine Bewertungen
- Diabetes Mellitus and Obesity As Risk Factors For Pancreatic CancerDokument13 SeitenDiabetes Mellitus and Obesity As Risk Factors For Pancreatic CancerAsunción AncoNoch keine Bewertungen
- Clinical Case Studies: Management of Dyslipidemia in Type 2 Diabetic Patient: A Case ReportDokument3 SeitenClinical Case Studies: Management of Dyslipidemia in Type 2 Diabetic Patient: A Case ReportBaek ShinNoch keine Bewertungen
- Liew - Anti Glycemic AgentsDokument42 SeitenLiew - Anti Glycemic AgentsA9 El-EbidiNoch keine Bewertungen
- Jama Echouffotcheugui 2023 RV 230007 1680895578.04302Dokument11 SeitenJama Echouffotcheugui 2023 RV 230007 1680895578.04302Buton InspirasiNoch keine Bewertungen
- 1 PDFDokument8 Seiten1 PDFsarahdianraniNoch keine Bewertungen
- My Nature CureDokument16 SeitenMy Nature Curehemraj.koiralaNoch keine Bewertungen
- Optimal Glycemic Target Level For Colon Cancer Patients With DiabetesDokument6 SeitenOptimal Glycemic Target Level For Colon Cancer Patients With DiabetesDieyAnt AzuraNoch keine Bewertungen
- Diabetes & Metabolic Syndrome: Clinical Research & Reviews: Bladder Cancer With Pioglitazone: A Caseecontrol StudyDokument7 SeitenDiabetes & Metabolic Syndrome: Clinical Research & Reviews: Bladder Cancer With Pioglitazone: A Caseecontrol StudyМалиша МанићNoch keine Bewertungen
- Evaluating The Impact of AMPK Activation, A Target of MetforminDokument10 SeitenEvaluating The Impact of AMPK Activation, A Target of Metforminiancaruso27Noch keine Bewertungen
- 1 SMDokument10 Seiten1 SMtommy areanNoch keine Bewertungen
- Higado Graso y CancerDokument9 SeitenHigado Graso y CancerCynthia CastilloNoch keine Bewertungen
- Demensia DMDokument5 SeitenDemensia DMNadia Rezki ErlizaNoch keine Bewertungen
- Type 2 Diabetes: Assessing The Relative Risks and Benefits of Glucose-Lowering MedicationsDokument10 SeitenType 2 Diabetes: Assessing The Relative Risks and Benefits of Glucose-Lowering MedicationsmosabNoch keine Bewertungen
- Knowledge Gap in DiabetesDokument3 SeitenKnowledge Gap in Diabetesamit545Noch keine Bewertungen
- Metformin in Patients With Type 2 Diabetes Mellitus and Heart Failure: A ReviewDokument10 SeitenMetformin in Patients With Type 2 Diabetes Mellitus and Heart Failure: A ReviewShaeli MalikNoch keine Bewertungen
- Metformin For Diabetes Prevention: Insights Gained From The Diabetes Prevention Program/Diabetes Prevention Program Outcomes StudyDokument11 SeitenMetformin For Diabetes Prevention: Insights Gained From The Diabetes Prevention Program/Diabetes Prevention Program Outcomes StudyRosa Villanueva CarrascoNoch keine Bewertungen
- AACE 2013 DM Consensus Statement 1Dokument48 SeitenAACE 2013 DM Consensus Statement 1As-sifa KharismaNoch keine Bewertungen
- Brit J Clinical Pharma - 2019 - Ahmadizar - Associations of Statin Use With Glycaemic Traits and Incident Type 2 DiabetesDokument10 SeitenBrit J Clinical Pharma - 2019 - Ahmadizar - Associations of Statin Use With Glycaemic Traits and Incident Type 2 DiabetesGianella VegasNoch keine Bewertungen
- Graduation Projects of 5 Year Students 2018/2019 1-Nameer Afaat Nassar Title: Approaches For The Treatment of Neuropathic PainDokument3 SeitenGraduation Projects of 5 Year Students 2018/2019 1-Nameer Afaat Nassar Title: Approaches For The Treatment of Neuropathic PainaillNoch keine Bewertungen
- Antioxidants 12 00904Dokument27 SeitenAntioxidants 12 00904Gabriela VazquezNoch keine Bewertungen
- Diabetes, Insulin Treatment, and Cancer Risk: What Is The Evidence?Dokument4 SeitenDiabetes, Insulin Treatment, and Cancer Risk: What Is The Evidence?Nuno DuarteNoch keine Bewertungen
- Chung2020 Article PrecisionMedicineInDiabetesACoDokument23 SeitenChung2020 Article PrecisionMedicineInDiabetesACoFilipa Figueiredo100% (1)
- Bartholins Gland Squamous Cell Carcinoma A Rare VDokument5 SeitenBartholins Gland Squamous Cell Carcinoma A Rare VWalida FadillahNoch keine Bewertungen
- Bartholins Gland Carcinomas A 20 Plus-Year ExperiDokument4 SeitenBartholins Gland Carcinomas A 20 Plus-Year ExperiWalida FadillahNoch keine Bewertungen
- Neodymium-YAG Iridotomy in Closure Glaucoma: Preliminary StudyDokument5 SeitenNeodymium-YAG Iridotomy in Closure Glaucoma: Preliminary StudyWalida FadillahNoch keine Bewertungen
- Accepted Manuscript: Diabetes Research and Clinical PracticeDokument28 SeitenAccepted Manuscript: Diabetes Research and Clinical PracticeWalida FadillahNoch keine Bewertungen
- FullDokument10 SeitenFullWalida FadillahNoch keine Bewertungen
- Molecules 16 02075 v2 PDFDokument9 SeitenMolecules 16 02075 v2 PDFWalida FadillahNoch keine Bewertungen
- Kpaake Thaddeus Terkimbi ProjectDokument59 SeitenKpaake Thaddeus Terkimbi ProjectsimonNoch keine Bewertungen
- 374-Article Text-761-3-10-20210101Dokument7 Seiten374-Article Text-761-3-10-20210101GeniaaldafitriaasgenNoch keine Bewertungen
- Knowledge Regarding Sexually Transmitted Disease (STD'S) Among B.Sc. Nursing First Year StudentsDokument3 SeitenKnowledge Regarding Sexually Transmitted Disease (STD'S) Among B.Sc. Nursing First Year StudentsEditor IJTSRDNoch keine Bewertungen
- Legionella - A Reemerging PathogenDokument9 SeitenLegionella - A Reemerging PathogenBam ManNoch keine Bewertungen
- PSM Ankit SunailDokument28 SeitenPSM Ankit Sunailnaveen gunturi50% (6)
- Barangay Health Governance Body 2018Dokument44 SeitenBarangay Health Governance Body 2018Donna Lei G. RosarioNoch keine Bewertungen
- Name: Ayanna Spence Grade: 11U Teacher: MR Haughton Subject: Biology Date: September 13, 2019Dokument18 SeitenName: Ayanna Spence Grade: 11U Teacher: MR Haughton Subject: Biology Date: September 13, 2019skeetsamNoch keine Bewertungen
- Final Issue BriefDokument8 SeitenFinal Issue Briefapi-549336558Noch keine Bewertungen
- CPD 1, 2016Dokument4 SeitenCPD 1, 2016DrDiya AlkayidNoch keine Bewertungen
- Infection and Bacterial InvasionDokument40 SeitenInfection and Bacterial InvasionTrisha BravoNoch keine Bewertungen
- CommonunitsA5 (4) PDF For Website812201441122Dokument2 SeitenCommonunitsA5 (4) PDF For Website812201441122Vijay Pal SinghNoch keine Bewertungen
- National Health Policy-2002: By: Mr. M. Sivananda ReddyDokument12 SeitenNational Health Policy-2002: By: Mr. M. Sivananda ReddySaumitra SahaiNoch keine Bewertungen
- 14 Infection ControlDokument27 Seiten14 Infection ControlMichelle Joy M. VicenteNoch keine Bewertungen
- Skrining Must - WordDokument3 SeitenSkrining Must - WordM Rendy RamadhanNoch keine Bewertungen
- Incident Reporting and Investigation ProcedureDokument12 SeitenIncident Reporting and Investigation ProcedureSyakira Bahiah100% (1)
- Amref's Annual Report For Year Two of The Katine ProjectDokument23 SeitenAmref's Annual Report For Year Two of The Katine ProjectLizFordNoch keine Bewertungen
- b28354990 PDFDokument582 Seitenb28354990 PDFSAAD ALHALAFINoch keine Bewertungen
- Obstetrical History and Assessment ActivityDokument3 SeitenObstetrical History and Assessment ActivityNielette R. BASALNoch keine Bewertungen
- Leptospirosis FactsDokument1 SeiteLeptospirosis FactsZenitha FauziaNoch keine Bewertungen
- STDs An Its Effects To The Mother and ChildDokument25 SeitenSTDs An Its Effects To The Mother and Childalixyshanjf.rvNoch keine Bewertungen
- Contraception MethodsDokument38 SeitenContraception MethodsDaisy NdhlovuNoch keine Bewertungen
- Security, Disease, Commerce - Ideologies of Postcolonial Global Health - Nicholas B. KingDokument28 SeitenSecurity, Disease, Commerce - Ideologies of Postcolonial Global Health - Nicholas B. KingbcallenmNoch keine Bewertungen
- Student - Handbook 2015 - NMD - Final PDFDokument49 SeitenStudent - Handbook 2015 - NMD - Final PDFCarlBuscatoNoch keine Bewertungen
- Assessment Exam Nle Enhancement Second Semester With AnswersDokument105 SeitenAssessment Exam Nle Enhancement Second Semester With AnswersPRINCESS TAHANoch keine Bewertungen
- Breed - : Neuter Certificate Additional Iformation About Your PetDokument2 SeitenBreed - : Neuter Certificate Additional Iformation About Your PetVanessa Joyce Selisana100% (1)
- Quarantine PresentationDokument35 SeitenQuarantine PresentationMelikteNoch keine Bewertungen
- Bag TechniqueDokument3 SeitenBag TechniquePrince Rener Velasco PeraNoch keine Bewertungen
- Maternal and Neonatal Outcomes of Preterm Premature Rupture of Membranes Before ViabilityDokument10 SeitenMaternal and Neonatal Outcomes of Preterm Premature Rupture of Membranes Before ViabilitymudeyNoch keine Bewertungen
- Why Abortion Should Be Legalized Argumentative EssayDokument2 SeitenWhy Abortion Should Be Legalized Argumentative EssayArina RahimiNoch keine Bewertungen
- Ss. 11. Dr. Dhani R. Sepsis Hiv3Dokument43 SeitenSs. 11. Dr. Dhani R. Sepsis Hiv3budi darmantaNoch keine Bewertungen