Das könnte Ihnen auch gefallen
- Acupuncture Therapy Center by SlidesgoDokument49 SeitenAcupuncture Therapy Center by SlidesgoEolia EffendiNoch keine Bewertungen
- Anterior Cruciate Ligament InjuryDokument16 SeitenAnterior Cruciate Ligament InjuryEolia EffendiNoch keine Bewertungen
- Non-Operating Room Anesthesia: Anesthetic Management of Pediatric Patients With William Syndrome For Cardiac Magnetic Resonance ImagingDokument3 SeitenNon-Operating Room Anesthesia: Anesthetic Management of Pediatric Patients With William Syndrome For Cardiac Magnetic Resonance ImagingEolia EffendiNoch keine Bewertungen
- Non-Operating Room Anesthesia: April 2017Dokument26 SeitenNon-Operating Room Anesthesia: April 2017Eolia EffendiNoch keine Bewertungen
- Variations in Herpes Zoster Manifestation: Review ArticleDokument5 SeitenVariations in Herpes Zoster Manifestation: Review ArticleEolia EffendiNoch keine Bewertungen
- Legal Medicine: K.-S. Saternus, H. Maxeiner, G. Kernbach-Wighton, J. KoebkeDokument6 SeitenLegal Medicine: K.-S. Saternus, H. Maxeiner, G. Kernbach-Wighton, J. KoebkeEolia EffendiNoch keine Bewertungen
- The Medicolegal Investigation of Deaths in CustodyDokument107 SeitenThe Medicolegal Investigation of Deaths in CustodyEolia EffendiNoch keine Bewertungen
- Non-Operatingroom Anesthesia: The Principles of Patient Assessment and PreparationDokument18 SeitenNon-Operatingroom Anesthesia: The Principles of Patient Assessment and PreparationEolia EffendiNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- English Investigatory Project FahadDokument25 SeitenEnglish Investigatory Project FahadAnush DcostaNoch keine Bewertungen
- General Microbiology 1617043754Dokument176 SeitenGeneral Microbiology 1617043754ArchanaNoch keine Bewertungen
- Presented By: Dr. Hirdesh Chawla Junior Resident IiiDokument79 SeitenPresented By: Dr. Hirdesh Chawla Junior Resident IiiAzizan HannyNoch keine Bewertungen
- Routine HIV Screening in Health Care Settings: Background and DefinitionsDokument23 SeitenRoutine HIV Screening in Health Care Settings: Background and Definitionsarya maulanaNoch keine Bewertungen
- SkinDokument20 SeitenSkinDr. Mary MjeedNoch keine Bewertungen
- PPT#4 Non Mendelian Pattern of Inheritance (STUDENT COPY ONLY)Dokument54 SeitenPPT#4 Non Mendelian Pattern of Inheritance (STUDENT COPY ONLY)Ma'am Nikki CaneNoch keine Bewertungen
- Otitis Externa: Investigation and Evidence-Based TreatmentDokument45 SeitenOtitis Externa: Investigation and Evidence-Based TreatmentSonya HyekyoNoch keine Bewertungen
- Drug Name Mechanism of Action Indication Contraindications Side Effects/Adverse Effects Nursing ConsiderationDokument5 SeitenDrug Name Mechanism of Action Indication Contraindications Side Effects/Adverse Effects Nursing ConsiderationWyeth Earl Padar EndrianoNoch keine Bewertungen
- Eukaryotic and Prokaryotic Gene Structure PDFDokument2 SeitenEukaryotic and Prokaryotic Gene Structure PDFAnthony0% (1)
- FlashcardsDokument18 SeitenFlashcardsDaphne HernaezNoch keine Bewertungen
- Chapter 1 - Introduction To Cell BiologyDokument106 SeitenChapter 1 - Introduction To Cell BiologyKw Chan100% (4)
- IAL Biol WBI05 Jan18 Scientific ArticleDokument8 SeitenIAL Biol WBI05 Jan18 Scientific ArticleMoeez AkramNoch keine Bewertungen
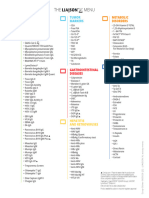
- Corp-Other-005026 2 - Liaison XL Assay Menu LRDokument1 SeiteCorp-Other-005026 2 - Liaison XL Assay Menu LRhannesfischer00Noch keine Bewertungen
- Oms 2018Dokument424 SeitenOms 2018ROBINNoch keine Bewertungen
- Full Download Test Bank For Contemporary Clinical Immunology and Serology Rittenhouse Olson PDF Full ChapterDokument13 SeitenFull Download Test Bank For Contemporary Clinical Immunology and Serology Rittenhouse Olson PDF Full Chapteraudreyrodgersezcafyxmip100% (19)
- Review Inhibitory Metabolites PDFDokument13 SeitenReview Inhibitory Metabolites PDFManika KargetiNoch keine Bewertungen
- G6 Science - U2 - Cells and OrganismsDokument92 SeitenG6 Science - U2 - Cells and OrganismsCandy Sanchez CuananNoch keine Bewertungen
- Preventing Needlestick InjuriesDokument6 SeitenPreventing Needlestick Injuriesnik adrianiNoch keine Bewertungen
- Heredity and Genetics PowerPointDokument55 SeitenHeredity and Genetics PowerPointShanelle BernalNoch keine Bewertungen
- Achondroplasia Ach: OMIM 2010Dokument56 SeitenAchondroplasia Ach: OMIM 2010Sevil GasanovaNoch keine Bewertungen
- Ap Biology 2020 Practice Exam 2 FRQDokument30 SeitenAp Biology 2020 Practice Exam 2 FRQEric ChiangNoch keine Bewertungen
- New Drugs 2018: New Drug Mechanism of Action UseDokument7 SeitenNew Drugs 2018: New Drug Mechanism of Action UsePremangshu GhoshalNoch keine Bewertungen
- Clarithromycin - Drug Information - UpToDate PDFDokument56 SeitenClarithromycin - Drug Information - UpToDate PDFNaztasia 'ola' Flowerin BNoch keine Bewertungen
- Microorganisms (The Coliform Group Bacteria) : S. D. SpenceDokument47 SeitenMicroorganisms (The Coliform Group Bacteria) : S. D. SpenceDeidra ShanNoch keine Bewertungen
- Pneumonia and GastroentiritisDokument3 SeitenPneumonia and Gastroentiritismarie100% (5)
- Mitotic Aberrations Induced by Orange Red (A Food Additive Dye) As A Potential Genotoxicant On Root Tip Cells of Onion (Allium Cepa L.)Dokument10 SeitenMitotic Aberrations Induced by Orange Red (A Food Additive Dye) As A Potential Genotoxicant On Root Tip Cells of Onion (Allium Cepa L.)satriaNoch keine Bewertungen
- A Systemic Review Covid-19 VaccineDokument13 SeitenA Systemic Review Covid-19 VaccineIJAR JOURNALNoch keine Bewertungen
- Atilano-Pdf - Assign (14) - Novel Drug Delivery SystemsDokument6 SeitenAtilano-Pdf - Assign (14) - Novel Drug Delivery SystemsAPRIL ROSE CAPUTOLANNoch keine Bewertungen
- 4-Blood (Hematopoiesis-Leukopoiesis) PDFDokument9 Seiten4-Blood (Hematopoiesis-Leukopoiesis) PDFUmair IkhlaqNoch keine Bewertungen
- Plant Breeding NotesDokument15 SeitenPlant Breeding Notesjack oumaNoch keine Bewertungen