Das könnte Ihnen auch gefallen
- Basic One-And Two-Dimensional NMR Spectroscopy: Horst FriebolinDokument10 SeitenBasic One-And Two-Dimensional NMR Spectroscopy: Horst FriebolinHiorrana Cássia FariaNoch keine Bewertungen
- SLB Training ManualDokument111 SeitenSLB Training ManualAdriana Rezende100% (1)
- Advances in Biological and Medical Physics: Volume 1Von EverandAdvances in Biological and Medical Physics: Volume 1Noch keine Bewertungen
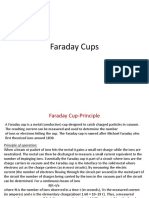
- Faraday CupsDokument10 SeitenFaraday CupsAshish SharmaNoch keine Bewertungen
- Principles and Applications of Well Logging-Hongqi Liu, 2017Dokument361 SeitenPrinciples and Applications of Well Logging-Hongqi Liu, 2017Dr. Ezaddin baban100% (6)
- Basic Considerations in Nuclear MedicineDokument12 SeitenBasic Considerations in Nuclear Medicinechberg13Noch keine Bewertungen
- Geophysical Techniques Lab Report:: Ferromagnetism, para Magnetism and DiamagnetismDokument4 SeitenGeophysical Techniques Lab Report:: Ferromagnetism, para Magnetism and DiamagnetismDeniz AkoumNoch keine Bewertungen
- Design, Construction and NMR Testing of A 1 Tesla Halbach Permanent Magnet For Magnetic ResonanceDokument5 SeitenDesign, Construction and NMR Testing of A 1 Tesla Halbach Permanent Magnet For Magnetic Resonancearesnickety100% (3)
- Thesis On TWTDokument181 SeitenThesis On TWTarshad aliNoch keine Bewertungen
- Senior Radiographer Nuclear MedicineDokument1 SeiteSenior Radiographer Nuclear Medicinetafi66Noch keine Bewertungen
- Epid PDFDokument14 SeitenEpid PDFARISA DWI SAKTINoch keine Bewertungen
- Linear Accelarator Technology - Dr. Lalit Aggarwal PDFDokument19 SeitenLinear Accelarator Technology - Dr. Lalit Aggarwal PDFKagitha Tirumala100% (1)
- Chapter 17 Single Photon Emission Computed TomographyDokument28 SeitenChapter 17 Single Photon Emission Computed TomographyJohnnie LópezNoch keine Bewertungen
- Nuclear Medicine GuideDokument3 SeitenNuclear Medicine GuidejeffsunilNoch keine Bewertungen
- Type of DetectorDokument47 SeitenType of DetectorAyesh aldiri100% (1)
- Beam Modification FinalDokument50 SeitenBeam Modification Finalapi-3726116100% (5)
- Nuclear Medicine Case StudyDokument6 SeitenNuclear Medicine Case StudyPrashant NagpureNoch keine Bewertungen
- Single-Side of Blumich (Hay)Dokument73 SeitenSingle-Side of Blumich (Hay)Dang Phuc HungNoch keine Bewertungen
- VMARTDokument92 SeitenVMARTCyc XimenaNoch keine Bewertungen
- Electron Beam Basic Concept - Dr. RavikumarDokument58 SeitenElectron Beam Basic Concept - Dr. RavikumarsuryaniNoch keine Bewertungen
- MLC CharacteristicDokument20 SeitenMLC CharacteristicMu AlimNoch keine Bewertungen
- The Radiation Chemistry of MacromoleculesVon EverandThe Radiation Chemistry of MacromoleculesMalcolm DoleNoch keine Bewertungen
- Cherenkov RadiationDokument17 SeitenCherenkov RadiationMayank GargNoch keine Bewertungen
- Brachy PDFDokument67 SeitenBrachy PDFPhys YarmoukNoch keine Bewertungen
- Vant Hof SpringerProtocols 2019 V2finalDokument38 SeitenVant Hof SpringerProtocols 2019 V2finalSusi SusantiNoch keine Bewertungen
- Photon Beam Characteristics & Basic Concepts of Treatment Planning - Dr. K J Maria Das PDFDokument63 SeitenPhoton Beam Characteristics & Basic Concepts of Treatment Planning - Dr. K J Maria Das PDFChino PlagaNoch keine Bewertungen
- Chapter 15 Special Techniques PDFDokument259 SeitenChapter 15 Special Techniques PDFSrinivas VenkataramanNoch keine Bewertungen
- SBRT PDFDokument14 SeitenSBRT PDFrubenNoch keine Bewertungen
- Radiotherapy SARP PDFDokument5 SeitenRadiotherapy SARP PDFskNoch keine Bewertungen
- A Low Field, Low Cost Halbach Magnet Array For Open Access NMRDokument4 SeitenA Low Field, Low Cost Halbach Magnet Array For Open Access NMRaresnickety100% (3)
- 3D Dose Computation AlgorithmsDokument10 Seiten3D Dose Computation AlgorithmsHashir SaeedNoch keine Bewertungen
- Raphex QuestionsDokument25 SeitenRaphex QuestionsHayrullo ShoniyozovNoch keine Bewertungen
- Aapm Report No. 16 Protocol For HeavyDokument60 SeitenAapm Report No. 16 Protocol For HeavyLaurentiu RadoiNoch keine Bewertungen
- Fluroscopy & Iitv SystemDokument87 SeitenFluroscopy & Iitv SystemMunish DograNoch keine Bewertungen
- SW ModelDokument10 SeitenSW Modelcipcirip2010Noch keine Bewertungen
- Cell Survival Curve 2Dokument16 SeitenCell Survival Curve 2Ahmed Ridwan OladotunNoch keine Bewertungen
- Amplifier Experiment Wiggler - by Science - GOVDokument161 SeitenAmplifier Experiment Wiggler - by Science - GOVBrian LopezNoch keine Bewertungen
- Solutions: Radiation Medicine QaDokument128 SeitenSolutions: Radiation Medicine QaHashir SaeedNoch keine Bewertungen
- Photon SpectraDokument8 SeitenPhoton SpectraSrinivas VenkataramanNoch keine Bewertungen
- MRI Clinical Application 1Dokument17 SeitenMRI Clinical Application 1Alberto AlbertoNoch keine Bewertungen
- Final Qa ChartDokument9 SeitenFinal Qa Chartapi-299270003Noch keine Bewertungen
- OF Co - 60 Unit: Nilesh Kumar PG Radiation Physics Department of Radiation PhysicsDokument54 SeitenOF Co - 60 Unit: Nilesh Kumar PG Radiation Physics Department of Radiation Physicsnilesh kumarNoch keine Bewertungen
- Treatment Planning AlgorithmsDokument51 SeitenTreatment Planning Algorithmskevin chenNoch keine Bewertungen
- Quantum Spectral AnalysisDokument140 SeitenQuantum Spectral AnalysisAradhita SharmaNoch keine Bewertungen
- Linear Accelarator 2020Dokument18 SeitenLinear Accelarator 2020Wafa NagiNoch keine Bewertungen
- Nuclear Medicine Tehnologist or Lead Nuclear Medicine TechnologiDokument2 SeitenNuclear Medicine Tehnologist or Lead Nuclear Medicine Technologiapi-78955179Noch keine Bewertungen
- IMRT Part 1 BJRDokument9 SeitenIMRT Part 1 BJRsusdoctorNoch keine Bewertungen
- Projection Radiography: EL5823/BE6203 Medical ImagingDokument71 SeitenProjection Radiography: EL5823/BE6203 Medical Imagingkhananu100% (1)
- Techniques Proton Radiotherapy: Bernard Gottschalk Harvard UniversityDokument39 SeitenTechniques Proton Radiotherapy: Bernard Gottschalk Harvard Universityasansone2220Noch keine Bewertungen
- Dose CalculationDokument5 SeitenDose CalculationAbdul Al-FattahNoch keine Bewertungen
- P8-9 CoverStory CT-HistoryDokument2 SeitenP8-9 CoverStory CT-Historyalem87Noch keine Bewertungen
- Body Basic - PpsDokument136 SeitenBody Basic - PpsRadiologi Mika bintaroNoch keine Bewertungen
- Treatment Planning Heterogeneity Vs Homogeneity Lung ProjectDokument13 SeitenTreatment Planning Heterogeneity Vs Homogeneity Lung Projectapi-299138743Noch keine Bewertungen
- Neutron SourcesDokument64 SeitenNeutron SourcesJenodi100% (1)
- Photon Interaction With MatterDokument16 SeitenPhoton Interaction With MatterShafuan WanNoch keine Bewertungen
- MRI Lecture NotesDokument33 SeitenMRI Lecture NotesArungoud PoshalaNoch keine Bewertungen
- IMRT Part 2 BJRDokument6 SeitenIMRT Part 2 BJRsusdoctorNoch keine Bewertungen
- Interaction of Radiation With MatterDokument16 SeitenInteraction of Radiation With MatterRachit KanchanNoch keine Bewertungen
- Review of Electron Beam Therapy PhysicsDokument36 SeitenReview of Electron Beam Therapy PhysicsMaría José Sánchez LovellNoch keine Bewertungen
- IMRT Basics: R. Alfredo C. Siochi, Ph.D. Juan Carlos Celi, PH.DDokument3 SeitenIMRT Basics: R. Alfredo C. Siochi, Ph.D. Juan Carlos Celi, PH.DSantanu SamantaNoch keine Bewertungen
- Lecture Magnetism in Solids-Trinity College-JS3015Dokument115 SeitenLecture Magnetism in Solids-Trinity College-JS3015Anonymous 9rJe2lOskxNoch keine Bewertungen
- Bok:978 94 007 1067 2Dokument479 SeitenBok:978 94 007 1067 2Olbira DuferaNoch keine Bewertungen
- Scintillation Camera Quality ControlDokument53 SeitenScintillation Camera Quality Controlknno87Noch keine Bewertungen
- Film ClassificationDokument28 SeitenFilm ClassificationprabhuNoch keine Bewertungen
- Chap 3 Resonance PhysicsDokument10 SeitenChap 3 Resonance PhysicsandreaNoch keine Bewertungen
- Quality Control in Diagnostic X Ray DepartmentDokument27 SeitenQuality Control in Diagnostic X Ray DepartmentandreaNoch keine Bewertungen
- Film ClassificationDokument28 SeitenFilm ClassificationprabhuNoch keine Bewertungen
- Filtri CavaliDokument11 SeitenFiltri CavaliandreaNoch keine Bewertungen
- Imrt VmatDokument29 SeitenImrt VmatandreaNoch keine Bewertungen
- Sistema Renina AldosteroneDokument8 SeitenSistema Renina AldosteroneandreaNoch keine Bewertungen
- Imrt VmatDokument29 SeitenImrt VmatandreaNoch keine Bewertungen
- Nxxnducnrncucjnducfndj Dmeucjdndbdyhs Wejfk Dmcufnenyfhjeeudndo Cmduncudhsnwmslosksk Djdncudncud DHD Ud DmejncudjdDokument1 SeiteNxxnducnrncucjnducfndj Dmeucjdndbdyhs Wejfk Dmcufnenyfhjeeudndo Cmduncudhsnwmslosksk Djdncudncud DHD Ud DmejncudjdandreaNoch keine Bewertungen
- Carbohydrates, Proteins, Nucleic Acids and Natural DyesDokument332 SeitenCarbohydrates, Proteins, Nucleic Acids and Natural DyesLyra AnthonyNoch keine Bewertungen
- QNMR Guideline Version001Dokument24 SeitenQNMR Guideline Version001Vaggelis DadiotisNoch keine Bewertungen
- Thermostat Algorithms For Molecular Dynamics Simulations: Phil@igc - Phys.chem - Ethz.chDokument45 SeitenThermostat Algorithms For Molecular Dynamics Simulations: Phil@igc - Phys.chem - Ethz.chrishadforuNoch keine Bewertungen
- Analytical ChemistryDokument12 SeitenAnalytical ChemistryArjayle Airobail LlevadoNoch keine Bewertungen
- Experimental BiophysicsDokument597 SeitenExperimental BiophysicsMOLGMI100% (1)
- ApplicationofNMRSpectroscopyinthePetroleumIndustry AReviewbyPNADokument47 SeitenApplicationofNMRSpectroscopyinthePetroleumIndustry AReviewbyPNACamilo Andrés GuerreroNoch keine Bewertungen
- Code Description DSMCDokument35 SeitenCode Description DSMCAnkit BansalNoch keine Bewertungen
- Quantum Dissipative SystemsDokument527 SeitenQuantum Dissipative SystemsDani Chao100% (3)
- Powerpoint Presentation PetrophysicsDokument18 SeitenPowerpoint Presentation PetrophysicsgregNoch keine Bewertungen
- Delta Release Notes v504 EDokument29 SeitenDelta Release Notes v504 Ehoesy1Noch keine Bewertungen
- Energetics of Ferromagnetism by Leon DragoneDokument30 SeitenEnergetics of Ferromagnetism by Leon DragonebarbosiNoch keine Bewertungen
- A 139215Dokument124 SeitenA 139215alirezaaghalari1980Noch keine Bewertungen
- NMR Lecture SOSDokument43 SeitenNMR Lecture SOSpoornanandhanNoch keine Bewertungen
- Carbon - 13 NMR: Nuclear Magnetic Resonance SpectrosDokument35 SeitenCarbon - 13 NMR: Nuclear Magnetic Resonance SpectrosSri Rezeki SamosirNoch keine Bewertungen
- 核磁共振部分习题及答案 3Dokument7 Seiten核磁共振部分习题及答案 3Nisal Nuwan SenarathnaNoch keine Bewertungen
- The Importance of Relaxation in The Sonobioelectromagnetic Life of A Human Cobe - D.haslerDokument4 SeitenThe Importance of Relaxation in The Sonobioelectromagnetic Life of A Human Cobe - D.haslerLeMérovingien AhadjiNoch keine Bewertungen
- Linear Vs Circular PolarizationDokument16 SeitenLinear Vs Circular Polarizationbernard smithNoch keine Bewertungen
- Take A Breath of Polarized Noble Gas: Ernst W Otten, Institutjur Physik, Johannes Gutenberg-Universitiit MainzDokument5 SeitenTake A Breath of Polarized Noble Gas: Ernst W Otten, Institutjur Physik, Johannes Gutenberg-Universitiit MainzRicky PizzoNoch keine Bewertungen
- 1 s2.0 003810987190278X MainDokument3 Seiten1 s2.0 003810987190278X Mainbruno.soaresNoch keine Bewertungen
- Sprawls Magnetic Resonance Imaging PMT PDFDokument184 SeitenSprawls Magnetic Resonance Imaging PMT PDFTHE VIRTUAL CLASSROOMNoch keine Bewertungen
- Principles and Applications of Well Logging (Hongqi Liu, 2017) @geo Pedia PDFDokument361 SeitenPrinciples and Applications of Well Logging (Hongqi Liu, 2017) @geo Pedia PDFAhmed OusamaNoch keine Bewertungen
- Chapter 12-Ans PDFDokument5 SeitenChapter 12-Ans PDFDave DM100% (1)
- Energy Level Structure and Transition ProbabilitiesDokument195 SeitenEnergy Level Structure and Transition ProbabilitiesAngela StefanNoch keine Bewertungen
- Investigation of Room Temperature Ferromagnetism in Transition Metal Doped Bifeo 3Dokument22 SeitenInvestigation of Room Temperature Ferromagnetism in Transition Metal Doped Bifeo 3BijoyKumarKuanrNoch keine Bewertungen
- 623Dokument304 Seiten623mylan_ScribdNoch keine Bewertungen
- 4.20 TYBSc Chemistry PDFDokument30 Seiten4.20 TYBSc Chemistry PDFShivam Mishra0% (1)
- Proton Precession MagnetometerDokument2 SeitenProton Precession MagnetometerprasadNoch keine Bewertungen