Das könnte Ihnen auch gefallen
- Central Bank Digital Currencies: Foundational Principles and Core FeaturesDokument26 SeitenCentral Bank Digital Currencies: Foundational Principles and Core FeaturesBeverly Tran100% (1)
- Protecting Our Democracy Act 2020 Fact SheetDokument3 SeitenProtecting Our Democracy Act 2020 Fact SheetBeverly TranNoch keine Bewertungen
- Michigan Attorney General Clergy Abuse Investigation 705417 7Dokument7 SeitenMichigan Attorney General Clergy Abuse Investigation 705417 7Beverly TranNoch keine Bewertungen
- Michigan Sex Offenders Registration Act (SORA) Second Amended Complaint 62818Dokument47 SeitenMichigan Sex Offenders Registration Act (SORA) Second Amended Complaint 62818Beverly TranNoch keine Bewertungen
- Juvenile Law Center - Labeled For Life August 2020Dokument76 SeitenJuvenile Law Center - Labeled For Life August 2020Beverly TranNoch keine Bewertungen
- Mitchell v. Dakota County Social Services Et Al.Dokument23 SeitenMitchell v. Dakota County Social Services Et Al.Beverly TranNoch keine Bewertungen
- DOJ CRIPA Request For COVID-19 Nursing Home Death Data Letter To Michigan Governor Gretchen Whitmer 08-26-2020Dokument2 SeitenDOJ CRIPA Request For COVID-19 Nursing Home Death Data Letter To Michigan Governor Gretchen Whitmer 08-26-2020Beverly TranNoch keine Bewertungen
- Karimi v. Deutsche Bank Aktiengesellschaft Et Al., No. 20-Cv-08978karimi v. Deutsche Bank Aktiengesellschaft Et Al., No. 20-cv-08978Dokument36 SeitenKarimi v. Deutsche Bank Aktiengesellschaft Et Al., No. 20-Cv-08978karimi v. Deutsche Bank Aktiengesellschaft Et Al., No. 20-cv-08978Beverly TranNoch keine Bewertungen
- Appointment of Jim Jones To San Francisco Housing AuthorityDokument1 SeiteAppointment of Jim Jones To San Francisco Housing AuthorityBeverly TranNoch keine Bewertungen
- Children's Health Defense v. Facebook Complaint DKT 1-08-17 2020Dokument115 SeitenChildren's Health Defense v. Facebook Complaint DKT 1-08-17 2020Beverly Tran100% (2)
- Toledo City Council Criminal ComplaintDokument41 SeitenToledo City Council Criminal ComplaintBeverly TranNoch keine Bewertungen
- Amended Complaint in FITE V Huntington National Bank - OhioDokument17 SeitenAmended Complaint in FITE V Huntington National Bank - OhioBeverly TranNoch keine Bewertungen
- Caritas Pro Vitae Gradu TrustDokument4 SeitenCaritas Pro Vitae Gradu TrustBeverly TranNoch keine Bewertungen
- High Court of Australia PELL V THE QUEEN 2020-12-2020-04-07Dokument2 SeitenHigh Court of Australia PELL V THE QUEEN 2020-12-2020-04-07Beverly Tran100% (1)
- Michigan Western District Stay On State Supreme Court Response On Whitmer Emergency Powers 061920Dokument7 SeitenMichigan Western District Stay On State Supreme Court Response On Whitmer Emergency Powers 061920Beverly TranNoch keine Bewertungen
- Yesse Yehudah Indictment - Fulfilling Our Responsibilities Unto Mankind, Also Known As FORUMDokument28 SeitenYesse Yehudah Indictment - Fulfilling Our Responsibilities Unto Mankind, Also Known As FORUMBeverly TranNoch keine Bewertungen
- Order of Malta American Association Year of Preparation Formation ProgramDokument17 SeitenOrder of Malta American Association Year of Preparation Formation ProgramBeverly TranNoch keine Bewertungen
- 10 1001@jama 2020 4783Dokument8 Seiten10 1001@jama 2020 4783Maria RamosNoch keine Bewertungen
- Connecticut Attorney General Legal Opinion Letter On Religious Exemption On Immunizatoins 5-6-2019Dokument7 SeitenConnecticut Attorney General Legal Opinion Letter On Religious Exemption On Immunizatoins 5-6-2019Beverly TranNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hindu Law, AN Sen, Sri Sai Law Publications, 2008 EdDokument21 SeitenHindu Law, AN Sen, Sri Sai Law Publications, 2008 EdSanket KumarNoch keine Bewertungen
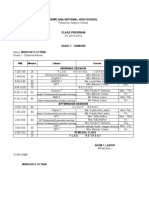
- General Class Program 2019-2020Dokument111 SeitenGeneral Class Program 2019-2020Ian MooneNoch keine Bewertungen
- Telugu LaxmiDokument2 SeitenTelugu LaxmiriyazNoch keine Bewertungen
- Case No. 69 - Antonio Vs ReyesDokument1 SeiteCase No. 69 - Antonio Vs ReyesMargie Marj GalbanNoch keine Bewertungen
- Rajeev Sarin v. State of UttrakhandDokument11 SeitenRajeev Sarin v. State of UttrakhandRUDRESH SINGHNoch keine Bewertungen
- A.C. No. 5948 January 22, 2003: AbaquetaDokument3 SeitenA.C. No. 5948 January 22, 2003: AbaquetaandangNoch keine Bewertungen
- Law of Tort CasesDokument203 SeitenLaw of Tort Caseskuboja_joram100% (2)
- Receiver Under Order XL of CPCDokument11 SeitenReceiver Under Order XL of CPCSamiun Hasib BhuiyanNoch keine Bewertungen
- Module Viii - Moral Character and Moral DevelopmentDokument30 SeitenModule Viii - Moral Character and Moral DevelopmentYani FranzNoch keine Bewertungen
- Case DoctrinesDokument2 SeitenCase DoctrinesCarl IlaganNoch keine Bewertungen
- sc13 1257Dokument29 Seitensc13 1257Henry TownsendNoch keine Bewertungen
- RA 8353 (Anti-Rape Law)Dokument4 SeitenRA 8353 (Anti-Rape Law)Niq Polido100% (1)
- 15 PLEYTOv LOMBOYdocxDokument2 Seiten15 PLEYTOv LOMBOYdocxKat RANoch keine Bewertungen
- Admin Case Pool 2: 4. Reclassification of LandsDokument131 SeitenAdmin Case Pool 2: 4. Reclassification of LandsBenedict Jonathan BermudezNoch keine Bewertungen
- Civil SocietyDokument9 SeitenCivil SocietyNadim MahmudNoch keine Bewertungen
- Aff Loss AsiloDokument4 SeitenAff Loss AsiloMikko AcubaNoch keine Bewertungen
- PNP Vs Concepcion Mining CompanyDokument4 SeitenPNP Vs Concepcion Mining CompanyWresen AnnNoch keine Bewertungen
- Hrs. of Baloy vs. CADokument1 SeiteHrs. of Baloy vs. CAalliah SolitaNoch keine Bewertungen
- 1981-People v. CuevoDokument10 Seiten1981-People v. CuevoKathleen Martin100% (1)
- The Philippine Real Estate E-Library: 3 Great Books in One CollectionDokument27 SeitenThe Philippine Real Estate E-Library: 3 Great Books in One CollectionShara Lyn100% (2)
- Supreme Court: R. B. Agrava For Appellants. Solicitor General Felix Q. Antonio For AppelleeDokument6 SeitenSupreme Court: R. B. Agrava For Appellants. Solicitor General Felix Q. Antonio For AppelleeZachary Philipp LimNoch keine Bewertungen
- Stephen Gerard Rodi v. Donald R. Ventetuolo, 941 F.2d 22, 1st Cir. (1991)Dokument16 SeitenStephen Gerard Rodi v. Donald R. Ventetuolo, 941 F.2d 22, 1st Cir. (1991)Scribd Government DocsNoch keine Bewertungen
- Neral Defences in PPCDokument3 SeitenNeral Defences in PPCFaique MemonNoch keine Bewertungen
- Corpuz v. Sto. TomasDokument9 SeitenCorpuz v. Sto. TomasJasminAubreyNoch keine Bewertungen
- Effect of Single Parenthood On The Academic Performance of Primary School PupilsDokument56 SeitenEffect of Single Parenthood On The Academic Performance of Primary School PupilsShaguolo O. Joseph100% (1)
- RULE 119 - 4 People V ChavesDokument1 SeiteRULE 119 - 4 People V ChavesPatatas SayoteNoch keine Bewertungen
- Debate: Legalization of Same-Sex MarriageDokument23 SeitenDebate: Legalization of Same-Sex MarriageDré OrquiolaNoch keine Bewertungen
- Adr NotesDokument39 SeitenAdr NotesAveakGangulyNoch keine Bewertungen
- Hermes E. Frias, Sr. vs. People of The Philippines G.R. No. 171437 - October 4, 2007Dokument1 SeiteHermes E. Frias, Sr. vs. People of The Philippines G.R. No. 171437 - October 4, 2007Myrna B Roque100% (2)
- 085 ALfredo v. BorrasDokument3 Seiten085 ALfredo v. BorrasKikoy IlaganNoch keine Bewertungen