Das könnte Ihnen auch gefallen
- Sydney 2008 MarchDokument8 SeitenSydney 2008 MarchYwagar YwagarNoch keine Bewertungen
- Save A Smile, Save A Life: How Complete Health Dentistry is Revolutionizing AmericaVon EverandSave A Smile, Save A Life: How Complete Health Dentistry is Revolutionizing AmericaNoch keine Bewertungen
- Remarks (OET Writing Task)Dokument4 SeitenRemarks (OET Writing Task)Apna FsdNoch keine Bewertungen
- CVS Exam Reveals Risk FactorsDokument8 SeitenCVS Exam Reveals Risk FactorsZweNoch keine Bewertungen
- Adelaide, 5 April, 2008: PaediatricsDokument17 SeitenAdelaide, 5 April, 2008: PaediatricsYwagar YwagarNoch keine Bewertungen
- Mel 2006 Apr 29Dokument5 SeitenMel 2006 Apr 29ZweNoch keine Bewertungen
- Shadowing JournalDokument3 SeitenShadowing Journalapi-489822381Noch keine Bewertungen
- Adelaide 13th September 2008Dokument16 SeitenAdelaide 13th September 2008Ywagar YwagarNoch keine Bewertungen
- Navi SonDokument10 SeitenNavi SonI m a BUFF50% (2)
- BrisDokument9 SeitenBrisYwagar YwagarNoch keine Bewertungen
- Fully Alive: Insights into Living with Extraordinary HealthVon EverandFully Alive: Insights into Living with Extraordinary HealthNoch keine Bewertungen
- Jerome Clark C.Cid, RNDokument5 SeitenJerome Clark C.Cid, RNJerome CidNoch keine Bewertungen
- FEB 2023Dokument11 SeitenFEB 2023Parsaant SinghNoch keine Bewertungen
- Paediatrics:: Case 1nsionDokument16 SeitenPaediatrics:: Case 1nsionYwagar YwagarNoch keine Bewertungen
- Mel 2005 Aug 20Dokument5 SeitenMel 2005 Aug 20ZweNoch keine Bewertungen
- Clincal Make Up Assignment #4Dokument8 SeitenClincal Make Up Assignment #4Catlyn ChatpmanNoch keine Bewertungen
- ReflectionDokument9 SeitenReflectionVino VinnoliNoch keine Bewertungen
- Managing a Patient with Recurrent Otitis MediaDokument5 SeitenManaging a Patient with Recurrent Otitis MediaZweNoch keine Bewertungen
- Vaginal Prolapse Colpocleisis LeFort Surgery A Personal StoryVon EverandVaginal Prolapse Colpocleisis LeFort Surgery A Personal StoryNoch keine Bewertungen
- Memoirs of Living With an Asshole Or How I Was Rear-ended by Ulcerative Colitis, J-Pouchitis, and the Medical ProfessionVon EverandMemoirs of Living With an Asshole Or How I Was Rear-ended by Ulcerative Colitis, J-Pouchitis, and the Medical ProfessionNoch keine Bewertungen
- placementDokument5 Seitenplacementmanaremad2000Noch keine Bewertungen
- Posting ElectiveDokument7 SeitenPosting ElectiveThulasi tootsieNoch keine Bewertungen
- OBGyn Clinical Rotation Module 4 GuideDokument7 SeitenOBGyn Clinical Rotation Module 4 Guidehevinpatel100% (1)
- GPDokument3 SeitenGPYwagar YwagarNoch keine Bewertungen
- Blood Transfusion Reaction Vsim - Sept 16 22 NSGD 2106Dokument5 SeitenBlood Transfusion Reaction Vsim - Sept 16 22 NSGD 2106api-631170779Noch keine Bewertungen
- No Guts, No Glory: Gut Solution - The Core of Your Total Wellness PlanVon EverandNo Guts, No Glory: Gut Solution - The Core of Your Total Wellness PlanBewertung: 3.5 von 5 Sternen3.5/5 (2)
- MCQ2 QuestionDokument100 SeitenMCQ2 Question9hjk6wpxyfNoch keine Bewertungen
- Cancer: What To Do After the Doctor Says You Are Cured!Von EverandCancer: What To Do After the Doctor Says You Are Cured!Noch keine Bewertungen
- Clinical Examination GuideDokument135 SeitenClinical Examination GuideManish AryanNoch keine Bewertungen
- From Sickness to Health: How I cured my autoimmune disease without medication. A must read for anyone with an illness. Your body is sick for a reasonVon EverandFrom Sickness to Health: How I cured my autoimmune disease without medication. A must read for anyone with an illness. Your body is sick for a reasonNoch keine Bewertungen
- MCC SaeDokument98 SeitenMCC SaeAllison100% (1)
- 3rd May 2008 SydneyDokument9 Seiten3rd May 2008 SydneyYwagar YwagarNoch keine Bewertungen
- Obstetric$ and Gynecology: PCOS (Us, B8L) ItDokument5 SeitenObstetric$ and Gynecology: PCOS (Us, B8L) ItZweNoch keine Bewertungen
- Relapse!: And the Legacy of Thyroid Cancer: Living With Thyroid Cancer, #3Von EverandRelapse!: And the Legacy of Thyroid Cancer: Living With Thyroid Cancer, #3Noch keine Bewertungen
- AMC-2007 Clinical Examination RecallsDokument156 SeitenAMC-2007 Clinical Examination Recallsbreezingthru100% (1)
- ACln2007!09!08MEL Retest Wd97Dokument6 SeitenACln2007!09!08MEL Retest Wd97Ywagar YwagarNoch keine Bewertungen
- Leukemia Diagnosis and Treatment GuideDokument16 SeitenLeukemia Diagnosis and Treatment GuideRyrey Abraham PacamanaNoch keine Bewertungen
- DecemebrDokument18 SeitenDecemebrRyrey Abraham PacamanaNoch keine Bewertungen
- Journal 1 PreceptorshipDokument4 SeitenJournal 1 Preceptorshipapi-418237167Noch keine Bewertungen
- 6th MarchDokument87 Seiten6th MarchYara AhmadNoch keine Bewertungen
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDokument14 SeitenClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarNoch keine Bewertungen
- Recall June11Dokument7 SeitenRecall June11mimovodaNoch keine Bewertungen
- DischargeplanningDokument6 SeitenDischargeplanningapi-288858560Noch keine Bewertungen
- Step 3 Form 3 CorrectedDokument41 SeitenStep 3 Form 3 CorrectedSBG BPT100% (2)
- Clinical ExemplarDokument5 SeitenClinical Exemplarapi-605270704Noch keine Bewertungen
- Exam Sample:: B. Cervical Incompetence and Cervical StenosisDokument3 SeitenExam Sample:: B. Cervical Incompetence and Cervical StenosisSiraj Ul IslamNoch keine Bewertungen
- Sti Case StudyDokument2 SeitenSti Case StudyJulia BrownNoch keine Bewertungen
- A Path Through the Cancer Fields: A Guide for Patients and FamiliesVon EverandA Path Through the Cancer Fields: A Guide for Patients and FamiliesNoch keine Bewertungen
- Case Study: Hypertrophic Pyloric Stenosis in Homeless InfantDokument3 SeitenCase Study: Hypertrophic Pyloric Stenosis in Homeless InfantJonah MaasinNoch keine Bewertungen
- Ongoing Professional Practice Evaluation (Oppe) : Administrative Policies and ProceduresDokument5 SeitenOngoing Professional Practice Evaluation (Oppe) : Administrative Policies and ProceduresTary BaruNoch keine Bewertungen
- ACT For Body Image DissatisfactionDokument218 SeitenACT For Body Image Dissatisfactionflorea_ela9916100% (11)
- StubbiesDokument3 SeitenStubbiesTovar GermanNoch keine Bewertungen
- Child Psychiatric DisordersDokument8 SeitenChild Psychiatric DisordersGaurang ShirwadkarNoch keine Bewertungen
- Metals and PsychotherapyDokument10 SeitenMetals and PsychotherapycarmendegarzaNoch keine Bewertungen
- Dutch Osteoporosis Physiotherapy FlowchartDokument1 SeiteDutch Osteoporosis Physiotherapy FlowchartyohanNoch keine Bewertungen
- Best of The Best 2013 - Winner's SectionDokument38 SeitenBest of The Best 2013 - Winner's SectionTrent SpoffordNoch keine Bewertungen
- Bka Case FinalDokument26 SeitenBka Case FinalJayson SorianoNoch keine Bewertungen
- Program CraiovaDokument9 SeitenProgram Craiovaonix2000Noch keine Bewertungen
- Medsurg Cardio Ana&PhysioDokument6 SeitenMedsurg Cardio Ana&Physiorabsibala80% (10)
- UT Trauma HandbookDokument49 SeitenUT Trauma Handbooksgod34Noch keine Bewertungen
- Individual PsychologyDokument5 SeitenIndividual PsychologyRessie Joy Catherine FelicesNoch keine Bewertungen
- Reality TherapyDokument2 SeitenReality TherapyAGLDNoch keine Bewertungen
- Proptosis UnilateralDokument5 SeitenProptosis UnilateralCarlos NiveloNoch keine Bewertungen
- Peds PresentationDokument31 SeitenPeds Presentationapi-247218432Noch keine Bewertungen
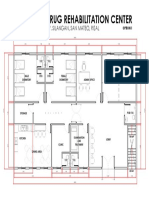
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDokument1 SeiteProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNoch keine Bewertungen
- Pharmacology Objective QuestionsDokument415 SeitenPharmacology Objective QuestionsharisNoch keine Bewertungen
- Atlas de Oncologia Clinica PDFDokument512 SeitenAtlas de Oncologia Clinica PDFAlfonso Carlos Gutierrez MartinezNoch keine Bewertungen
- Practice Test 5Dokument4 SeitenPractice Test 5Dương Lê QuýNoch keine Bewertungen
- ProposalDokument45 SeitenProposalJP firmNoch keine Bewertungen
- Acute Gingival InfectionsDokument35 SeitenAcute Gingival InfectionsAhmed Tawfig GamalNoch keine Bewertungen
- Intraoperative Radiotherapy (IORT) For Surgically Resected Brain Metastases: Outcome Analysis of An International Cooperative StudyDokument15 SeitenIntraoperative Radiotherapy (IORT) For Surgically Resected Brain Metastases: Outcome Analysis of An International Cooperative Studyuyenminh2802Noch keine Bewertungen
- Skin, Soft Tissue & BreastDokument10 SeitenSkin, Soft Tissue & BreastFarhin100% (1)
- How To Grow Medicinal MarijuanaDokument9 SeitenHow To Grow Medicinal MarijuanaRoy HarperNoch keine Bewertungen
- Healthy Hair Guide Magazine PDFDokument15 SeitenHealthy Hair Guide Magazine PDFjagan100% (1)
- Drug Development and BEDokument19 SeitenDrug Development and BEJoseph KamaleshNoch keine Bewertungen
- Nurse Practitioner VS Physical TherapistsDokument5 SeitenNurse Practitioner VS Physical Therapistspdet1Noch keine Bewertungen
- Assignment 3 4 Relapse Prevention Paper Brian MannDokument8 SeitenAssignment 3 4 Relapse Prevention Paper Brian Mannapi-301673059Noch keine Bewertungen
- Chitosan ReviewDokument20 SeitenChitosan ReviewkarthikNoch keine Bewertungen