Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Bone TumorsDokument62 SeitenBone TumorsEvan Permana PutraNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Retinal Detachment PDFDokument8 SeitenRetinal Detachment PDFEvan Permana PutraNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Marker KankerDokument1 SeiteMarker KankerEvan Permana PutraNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- RenalstonesDokument13 SeitenRenalstonesEvan Permana PutraNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Ocular TraumaDokument109 SeitenOcular TraumaEvan Permana PutraNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Exercise MethodDokument13 SeitenExercise MethodEvan Permana PutraNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Oxygen DeliveryDokument10 SeitenOxygen DeliveryEvan Permana PutraNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Ocular TraumaDokument109 SeitenOcular TraumaEvan Permana PutraNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- SssDokument5 SeitenSssEvan Permana PutraNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Assessment of Vestibular SystemDokument31 SeitenAssessment of Vestibular SystemEvan Permana Putra100% (1)
- Kalender Siklus Dokter MudaDokument1 SeiteKalender Siklus Dokter MudaEvan Permana PutraNoch keine Bewertungen
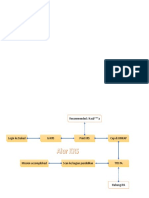
- Alur KRSDokument2 SeitenAlur KRSEvan PermanaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Natural History and Spectrum of DiseaseDokument34 SeitenNatural History and Spectrum of DiseaseEvan Permana Putra100% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Estimating RiskDokument47 SeitenEstimating RiskEvan Permana PutraNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Models of Health Behavior: DR Yusuf Abdu MisauDokument80 SeitenModels of Health Behavior: DR Yusuf Abdu MisauEvan Permana PutraNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- ATP III Guideline KolesterolDokument6 SeitenATP III Guideline KolesterolRakasiwi GalihNoch keine Bewertungen
- Genogram SymbolsDokument7 SeitenGenogram SymbolsBenor AmRi MustaqimNoch keine Bewertungen
- Guideline ADA 2010 in Hyperglicemia CrisisDokument9 SeitenGuideline ADA 2010 in Hyperglicemia CrisisAissyiyah Nur An NisaNoch keine Bewertungen
- Sepsis Dan Syok SepsisDokument13 SeitenSepsis Dan Syok SepsisEvan Permana PutraNoch keine Bewertungen
- Ophthalmology AlgorithmsDokument5 SeitenOphthalmology AlgorithmsEvan Permana PutraNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- EpistaxisDokument7 SeitenEpistaxisapi-3728652100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Diagnosis and Management of Red EyeDokument8 SeitenDiagnosis and Management of Red EyeNelly AstikaNoch keine Bewertungen
- DepresiDokument6 SeitenDepresiEvan Permana PutraNoch keine Bewertungen
- Swollen Red Eyelid PDFDokument10 SeitenSwollen Red Eyelid PDFEvan Permana PutraNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Basic Genogram Symbols GuideDokument1 SeiteBasic Genogram Symbols GuideEvan Permana Putra100% (4)
- Epidemic Curve BasicsDokument24 SeitenEpidemic Curve BasicsEvan Permana Putra100% (1)
- Treating Sepsis - The Latest EvidenceDokument1 SeiteTreating Sepsis - The Latest EvidenceEvan Permana PutraNoch keine Bewertungen
- Epidemic CurveDokument24 SeitenEpidemic CurveEvan Permana Putra50% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Investigation of Outbreak 2Dokument54 SeitenInvestigation of Outbreak 2Evan Permana PutraNoch keine Bewertungen
- Endodontic Surgery: Incision and DrainageDokument8 SeitenEndodontic Surgery: Incision and DrainageHadoo OolaNoch keine Bewertungen
- Revision Test of Chapter 1 ScienceDokument4 SeitenRevision Test of Chapter 1 ScienceYasoktaran AnanthanNoch keine Bewertungen
- Community Health Nursing Course OutlineDokument5 SeitenCommunity Health Nursing Course OutlineMeeKo VideñaNoch keine Bewertungen
- Calendar Eivv+Fivb Online Event: CT T OMEDokument1 SeiteCalendar Eivv+Fivb Online Event: CT T OMEALTEREGO ESTUDIO CREATIVONoch keine Bewertungen
- GHJKKDokument759 SeitenGHJKKVu HauNoch keine Bewertungen
- A Budget of Dumb Asses 2011Dokument2 SeitenA Budget of Dumb Asses 2011piano1985Noch keine Bewertungen
- Department of Labor: ISH Registration Flier - 07Dokument9 SeitenDepartment of Labor: ISH Registration Flier - 07USA_DepartmentOfLaborNoch keine Bewertungen
- House Hearing, 113TH Congress - A Matter of Life and Death: Examining Preventable Deaths, Patient Safety Issues, and Bonuses For Va Execs Who Oversaw ThemDokument121 SeitenHouse Hearing, 113TH Congress - A Matter of Life and Death: Examining Preventable Deaths, Patient Safety Issues, and Bonuses For Va Execs Who Oversaw ThemScribd Government DocsNoch keine Bewertungen
- Para Lec ReviewerDokument18 SeitenPara Lec ReviewerRudolph MendozaNoch keine Bewertungen
- Poikilocytosis Review TableDokument5 SeitenPoikilocytosis Review Tablekat100% (1)
- The African Post Covid-19 RealityDokument2 SeitenThe African Post Covid-19 RealityJeremiah IgwurubeNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Orthopaedic Surgery MCQsDokument23 SeitenOrthopaedic Surgery MCQsWinifred Chen70% (10)
- Unang YakapDokument5 SeitenUnang YakapMitch GatelaNoch keine Bewertungen
- Peripheral Nerve DisordersDokument33 SeitenPeripheral Nerve Disordersbpt2Noch keine Bewertungen
- Open Letter English 2010 AssignmentDokument5 SeitenOpen Letter English 2010 Assignmentapi-551077399Noch keine Bewertungen
- Planning and Designing An Isolation Facility in Hospitals Need of The Hour PDFDokument9 SeitenPlanning and Designing An Isolation Facility in Hospitals Need of The Hour PDFdzakyzahidNoch keine Bewertungen
- The Dry EyeDokument8 SeitenThe Dry EyeMohit BooraNoch keine Bewertungen
- Outline - Script Lesson Plan For Bacteria - Field IDokument3 SeitenOutline - Script Lesson Plan For Bacteria - Field Iapi-328213101Noch keine Bewertungen
- History of MedivineDokument39 SeitenHistory of Medivinelionking68Noch keine Bewertungen
- Novel Coronavirus Disease 2019 (COVID-19) : Review of Related LiteratureDokument7 SeitenNovel Coronavirus Disease 2019 (COVID-19) : Review of Related LiteratureqNoch keine Bewertungen
- How To Write An Abstract UcsbDokument14 SeitenHow To Write An Abstract UcsbJohn ReyNoch keine Bewertungen
- AMOEBIASISDokument44 SeitenAMOEBIASISJorge RabajaNoch keine Bewertungen
- Diaper (Napkin) Dermatitis A FoldDokument6 SeitenDiaper (Napkin) Dermatitis A FoldLina Mahayaty SembiringNoch keine Bewertungen
- Epidemiology BooksDokument5 SeitenEpidemiology BooksAdrin Ma'rufNoch keine Bewertungen
- What Is Pityriasis Rosea?Dokument1 SeiteWhat Is Pityriasis Rosea?andinaNoch keine Bewertungen
- Evaluation Entomological WarfareDokument62 SeitenEvaluation Entomological WarfareReid Kirby100% (1)
- bb10 Chap1Dokument116 Seitenbb10 Chap1Dulce Kriselda E. FaigmaniNoch keine Bewertungen
- Namagunga Primary Boarding School: Revision Work (Set I) Term One 2020 English Primary SixDokument12 SeitenNamagunga Primary Boarding School: Revision Work (Set I) Term One 2020 English Primary SixMonydit santinoNoch keine Bewertungen
- Hennebert's SignDokument3 SeitenHennebert's SignatmhyaNoch keine Bewertungen