Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Science 3 DLP 1 - Sense Organs and Their FunctionsDokument16 SeitenScience 3 DLP 1 - Sense Organs and Their FunctionsRussel Jane Sumonod - Maraguinot100% (3)
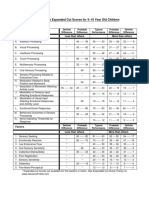
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDokument1 SeiteSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliNoch keine Bewertungen
- Physical Activity Factsheet Who Eu 201811 enDokument148 SeitenPhysical Activity Factsheet Who Eu 201811 enarief aceNoch keine Bewertungen
- Interactive Courseware For Supporting Learners Competency in Practical SkillsDokument13 SeitenInteractive Courseware For Supporting Learners Competency in Practical Skillsarief aceNoch keine Bewertungen
- Promoting Healthy LifestylesDokument2 SeitenPromoting Healthy Lifestylesarief aceNoch keine Bewertungen
- Eu Sport Factsheet enDokument2 SeitenEu Sport Factsheet enarief aceNoch keine Bewertungen
- Daily Competition Results July 23rd 2019Dokument32 SeitenDaily Competition Results July 23rd 2019arief aceNoch keine Bewertungen
- Understanding ExplosiveDokument145 SeitenUnderstanding Explosiveaggresssev100% (1)
- Tracing The Criminal Policy On Castration and Community ResponseDokument17 SeitenTracing The Criminal Policy On Castration and Community Responsearief aceNoch keine Bewertungen
- Revitalization of Funding For Savings and Loans Cooperatives As Efforts To Improve The State'S Economy After The Covid-19 PandemicDokument21 SeitenRevitalization of Funding For Savings and Loans Cooperatives As Efforts To Improve The State'S Economy After The Covid-19 Pandemicarief aceNoch keine Bewertungen
- Performance Structure Analysis of The Men's and Women's Badminton Doubles Matches in The Olympic Games From 2008 To 2016 During Playoffs StageDokument13 SeitenPerformance Structure Analysis of The Men's and Women's Badminton Doubles Matches in The Olympic Games From 2008 To 2016 During Playoffs Stagearief aceNoch keine Bewertungen
- Investigation of The Head Impact Power of A Sepak: Takraw Ball On Sepak Takraw PlayersDokument15 SeitenInvestigation of The Head Impact Power of A Sepak: Takraw Ball On Sepak Takraw Playersarief aceNoch keine Bewertungen
- Performance Structure Analysis of The Men's and Women's Badminton Doubles Matches in The Olympic Games From 2008 To 2016 During Playoffs StageDokument13 SeitenPerformance Structure Analysis of The Men's and Women's Badminton Doubles Matches in The Olympic Games From 2008 To 2016 During Playoffs Stagearief aceNoch keine Bewertungen
- Investigation of The Head Impact Power of A Sepak: Takraw Ball On Sepak Takraw PlayersDokument15 SeitenInvestigation of The Head Impact Power of A Sepak: Takraw Ball On Sepak Takraw Playersarief aceNoch keine Bewertungen
- Response of The Brain To EnrichmentDokument66 SeitenResponse of The Brain To EnrichmentCandi Kamira BalladaresNoch keine Bewertungen
- Theory of Personality Chapter-1Dokument13 SeitenTheory of Personality Chapter-1chat gaza0% (1)
- Ass. Kay Sir CyrusDokument3 SeitenAss. Kay Sir CyrusAdrian ArmendiNoch keine Bewertungen
- Fleming (2014) Pilot Randomized Controlled Trial of Dialectical Behavior Therapy Group Skills Training For ADHDDokument12 SeitenFleming (2014) Pilot Randomized Controlled Trial of Dialectical Behavior Therapy Group Skills Training For ADHDjuanNoch keine Bewertungen
- Vygotsky's Socio-Cultural Theory and Zone of Proximal DevelopmentDokument14 SeitenVygotsky's Socio-Cultural Theory and Zone of Proximal DevelopmentEmman Dela CruzNoch keine Bewertungen
- Non-Suicidal Self-Injury (NSSI) and Suicide: Criteria DifferentiationDokument7 SeitenNon-Suicidal Self-Injury (NSSI) and Suicide: Criteria DifferentiationTututWidyaNurAnggrainiNoch keine Bewertungen
- Controlling Thought Waves: Understanding Chitta Vritti and the Five VrittisDokument14 SeitenControlling Thought Waves: Understanding Chitta Vritti and the Five VrittisApexa Kerai100% (1)
- Leadership Assessment From MindtoolsDokument3 SeitenLeadership Assessment From MindtoolsigoeneezmNoch keine Bewertungen
- Cns Neurological ExaminationDokument26 SeitenCns Neurological ExaminationDr.P.NatarajanNoch keine Bewertungen
- Relapse Processes After The Extinction of Instrumental Learning: Renewal, Resurgence, and ReacquisitionDokument12 SeitenRelapse Processes After The Extinction of Instrumental Learning: Renewal, Resurgence, and ReacquisitionjsaccuzzoNoch keine Bewertungen
- MotivationDokument9 SeitenMotivationarsal169100% (1)
- Classification of Intelligence TestDokument4 SeitenClassification of Intelligence TestIndu YadavNoch keine Bewertungen
- Self-Consciousness Defines the SelfDokument2 SeitenSelf-Consciousness Defines the SelfKris TinaNoch keine Bewertungen
- DLL - English 2 - Q1 - W1Dokument4 SeitenDLL - English 2 - Q1 - W1Carino ArleneNoch keine Bewertungen
- Rebecca Brittain MSThesisDokument58 SeitenRebecca Brittain MSThesisMișa RtrNoch keine Bewertungen
- Personal Style InventoryDokument3 SeitenPersonal Style InventorymandyNoch keine Bewertungen
- How Your Brain WorksDokument7 SeitenHow Your Brain WorksMRITZNoch keine Bewertungen
- Pathophysiology of Severe Mental RetardationDokument4 SeitenPathophysiology of Severe Mental RetardationGiancarlo_Gala_4548Noch keine Bewertungen
- TYPICAL AND ATYPICAL DEVELOPMENTDokument43 SeitenTYPICAL AND ATYPICAL DEVELOPMENTJosh PelayoNoch keine Bewertungen
- Soal Penyisihan KMNR 10 Kelas 1-2Dokument12 SeitenSoal Penyisihan KMNR 10 Kelas 1-2Hari Kurniawan0% (1)
- Trauma and Self CareDokument54 SeitenTrauma and Self CarerimshaNoch keine Bewertungen
- Infant Sleep and Its Relation With CognitionDokument15 SeitenInfant Sleep and Its Relation With CognitionLara GintingNoch keine Bewertungen
- Alzheimer Disease - Risks, Symptoms and Related TestsDokument15 SeitenAlzheimer Disease - Risks, Symptoms and Related TestsMishelaNoch keine Bewertungen
- LearningDokument6 SeitenLearningSALAUDEEN SAEFULLAHNoch keine Bewertungen
- PSYC327 Lab Report Introduction - Karishma DO SarabajeetDokument6 SeitenPSYC327 Lab Report Introduction - Karishma DO SarabajeetdeepasankunyNoch keine Bewertungen
- Deafness & Hearing LossDokument39 SeitenDeafness & Hearing LossjialeongNoch keine Bewertungen
- Theories of Motivation in ManagementDokument10 SeitenTheories of Motivation in ManagementAvani TomarNoch keine Bewertungen
- Learning and Teaching Styles in Public SchoolsDokument12 SeitenLearning and Teaching Styles in Public SchoolsJeneffer Estal FragaNoch keine Bewertungen