Das könnte Ihnen auch gefallen
- Intra-Operative Care CompetencyDokument2 SeitenIntra-Operative Care CompetencyTryll Susa100% (1)
- JEE ZoonosisDokument30 SeitenJEE ZoonosisbabekayyasaNoch keine Bewertungen
- Chemical Pharma Report 2019Dokument124 SeitenChemical Pharma Report 2019CIO White PapersNoch keine Bewertungen
- GMP in Pharmaceutical Industry: Global cGMP & Regulatory ExpectationsVon EverandGMP in Pharmaceutical Industry: Global cGMP & Regulatory ExpectationsBewertung: 5 von 5 Sternen5/5 (2)
- Gnap 1995 Conducted A Survey On Teacher Workload Which Was Used in Exercise 16 of Chapter 5 A 3Dokument2 SeitenGnap 1995 Conducted A Survey On Teacher Workload Which Was Used in Exercise 16 of Chapter 5 A 3Charlotte0% (1)
- The Impact of Financial Stability On Student Academic PerformanceDokument2 SeitenThe Impact of Financial Stability On Student Academic PerformanceYvonne AdrianoNoch keine Bewertungen
- National Pharmacovigilance Roadmap 2020Dokument39 SeitenNational Pharmacovigilance Roadmap 2020TafereMulawNoch keine Bewertungen
- PvPI EditedDokument29 SeitenPvPI Editedneeraj devarintiNoch keine Bewertungen
- Pharmacovigilance Programme of India The Journey Travelled and The Way ForwardDokument8 SeitenPharmacovigilance Programme of India The Journey Travelled and The Way ForwardPreeti KharbNoch keine Bewertungen
- Pharma - 2015-16 PDFDokument108 SeitenPharma - 2015-16 PDFclive.mascarenhas909Noch keine Bewertungen
- Office THE: OF SecretaryDokument12 SeitenOffice THE: OF SecretaryJomelle WongNoch keine Bewertungen
- Bridging Gaps in Pharmacovigilance With Social Media Listening and Competitive IntelligenceDokument31 SeitenBridging Gaps in Pharmacovigilance With Social Media Listening and Competitive IntelligenceYosua HonasanNoch keine Bewertungen
- PEPFAR Indicator Reference GuidanceDokument206 SeitenPEPFAR Indicator Reference GuidanceTuntufye AbelNoch keine Bewertungen
- Drug Approval System in MalaysiaDokument47 SeitenDrug Approval System in MalaysiaAnu PariyarathNoch keine Bewertungen
- Desk Study For AIDS Medicines and Diagnostic Services: October 10, 2005Dokument37 SeitenDesk Study For AIDS Medicines and Diagnostic Services: October 10, 2005inayat1Noch keine Bewertungen
- Pharmacovigilance in India - A PerspectiveDokument4 SeitenPharmacovigilance in India - A PerspectiveVijay Venkatraman JanarthananNoch keine Bewertungen
- HQ2010V13SP16Dokument10 SeitenHQ2010V13SP16DharmendraNoch keine Bewertungen
- PIDS: Assessment of The COMPACK ProgramDokument6 SeitenPIDS: Assessment of The COMPACK ProgramAt Day's WardNoch keine Bewertungen
- National Infection Prevention and Control Board Assurance FrameworkDokument55 SeitenNational Infection Prevention and Control Board Assurance FrameworkhebasnmcNoch keine Bewertungen
- Impurity Profiling of Pharmaceuticals PDFDokument15 SeitenImpurity Profiling of Pharmaceuticals PDFvikram kushwahaNoch keine Bewertungen
- English Annual Report 2021-22Dokument172 SeitenEnglish Annual Report 2021-22Ashish SharmaNoch keine Bewertungen
- Achieving ''Zero'' Defects For Visible Particles in InjectablesDokument13 SeitenAchieving ''Zero'' Defects For Visible Particles in InjectablesmmmmmNoch keine Bewertungen
- Ao 2011-0009Dokument21 SeitenAo 2011-0009Joline UrbinaNoch keine Bewertungen
- Overview of Pharmacovigilance and Good Distribution Practices: Program and Activities in IndonesiaDokument32 SeitenOverview of Pharmacovigilance and Good Distribution Practices: Program and Activities in IndonesiaPutri DtwinsNoch keine Bewertungen
- Big Data Highlights Issue 4 - enDokument7 SeitenBig Data Highlights Issue 4 - entiecvuibatngoNoch keine Bewertungen
- Seminar DR Rowa Final2 Edit ReemDokument31 SeitenSeminar DR Rowa Final2 Edit ReemMustafa IdaisNoch keine Bewertungen
- Indian Pharmacopoeia Commission Structure and Role in Formulation of IP and NFI PDFDokument5 SeitenIndian Pharmacopoeia Commission Structure and Role in Formulation of IP and NFI PDFArunabh ArandharaNoch keine Bewertungen
- M-E Systems AssessmentDokument28 SeitenM-E Systems AssessmentShahid NadeemNoch keine Bewertungen
- SADR Investigation SOPDokument8 SeitenSADR Investigation SOPNaakor LaryeaNoch keine Bewertungen
- Drantonamrcontrolinthe PhilippinesDokument27 SeitenDrantonamrcontrolinthe PhilippinesJuhne del ReyNoch keine Bewertungen
- PV Guidance DocumentDokument54 SeitenPV Guidance DocumentRenneyNoch keine Bewertungen
- English Annual Report 2020-21-0Dokument151 SeitenEnglish Annual Report 2020-21-0mohitNoch keine Bewertungen
- FDA Pesticides in Food Compliance GuideDokument40 SeitenFDA Pesticides in Food Compliance Guidekristy yolibeth lopez banegasNoch keine Bewertungen
- National Medication Errors Reporting System at Ministry of Health in Saudi ArabiaDokument6 SeitenNational Medication Errors Reporting System at Ministry of Health in Saudi ArabiaEman MohamedNoch keine Bewertungen
- Safety: Medicines in Public Health ProgrammesDokument61 SeitenSafety: Medicines in Public Health Programmeswiwit0490Noch keine Bewertungen
- Indian Pharmacopoeia Commission Structure and Role in Formulation of IP and NFI PDFDokument5 SeitenIndian Pharmacopoeia Commission Structure and Role in Formulation of IP and NFI PDFRajesh KumarNoch keine Bewertungen
- Pharmacovigilance: Need and Future Prospective in Herbal and Ayurvedic MedicinesDokument5 SeitenPharmacovigilance: Need and Future Prospective in Herbal and Ayurvedic MedicinesBhavana GangurdeNoch keine Bewertungen
- The Phil Med Policy (Tabular Summary) Shayne ManeseDokument39 SeitenThe Phil Med Policy (Tabular Summary) Shayne ManesePaolo ZacariasNoch keine Bewertungen
- E004227 FullDokument14 SeitenE004227 Fullannisa nasiraNoch keine Bewertungen
- The Periodic Safety Update Report As A Pharmacovigilance ToolDokument10 SeitenThe Periodic Safety Update Report As A Pharmacovigilance ToolNova AmaliaNoch keine Bewertungen
- Regulatory Control of Generic Medicine in MalaysiaDokument45 SeitenRegulatory Control of Generic Medicine in MalaysiaLong ChongNoch keine Bewertungen
- His Module Week 5Dokument5 SeitenHis Module Week 5Gia Janella SemillaNoch keine Bewertungen
- Accelerating Access To Quality Products in Low and Middle Income CountriesDokument14 SeitenAccelerating Access To Quality Products in Low and Middle Income CountriesFasika MeketeNoch keine Bewertungen
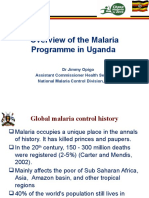
- Malaria Control in UgandaDokument26 SeitenMalaria Control in UgandaIT ManagerNoch keine Bewertungen
- Methadone Low Res 09-06-12 PDFDokument54 SeitenMethadone Low Res 09-06-12 PDFFitri N JannahNoch keine Bewertungen
- Pharmacovigilance: Masterkey To Drug Safety Monitoring and Its Status in IndiaDokument4 SeitenPharmacovigilance: Masterkey To Drug Safety Monitoring and Its Status in IndiaSejal khumanNoch keine Bewertungen
- Schedule YDokument43 SeitenSchedule YVaibhav ThoratNoch keine Bewertungen
- Annual Report 2019-20 PDFDokument158 SeitenAnnual Report 2019-20 PDFpaulNoch keine Bewertungen
- Comparison of PV in Japan and GermanyDokument28 SeitenComparison of PV in Japan and GermanySutirtho MukherjiNoch keine Bewertungen
- Adverse Drug Reaction Reporting System in PakistanDokument31 SeitenAdverse Drug Reaction Reporting System in Pakistansara raeesNoch keine Bewertungen
- WHO Drug Information 2000Dokument66 SeitenWHO Drug Information 2000Rajib ChowdhuryNoch keine Bewertungen
- MateriDokument25 SeitenMateriRefki Okta TriadiNoch keine Bewertungen
- MODULE 1 Overview of The InstitutionDokument45 SeitenMODULE 1 Overview of The InstitutionShannen CostoNoch keine Bewertungen
- African Development Bank: Departement AhhdDokument17 SeitenAfrican Development Bank: Departement AhhdPam ExquisitesNoch keine Bewertungen
- Pharmaceutical Review PolicyDokument30 SeitenPharmaceutical Review PolicyMahathi DepuruNoch keine Bewertungen
- Pharmacy CUM L - IVDokument87 SeitenPharmacy CUM L - IVMoges GuangulNoch keine Bewertungen
- World Health Organization: WHO/EMC/BAC/98.6Dokument5 SeitenWorld Health Organization: WHO/EMC/BAC/98.6gabriela_mariangela5929Noch keine Bewertungen
- Standards, Toolkits and Guidance To Advance Regulator PrioritiesDokument16 SeitenStandards, Toolkits and Guidance To Advance Regulator PrioritieshuykhiemNoch keine Bewertungen
- CAPPM - Guidekubes-CurrentDokument10 SeitenCAPPM - Guidekubes-CurrentchanderjagdishNoch keine Bewertungen
- Pharmacovigilance: A Worldwide Master Key For Drug Safety MonitoringDokument6 SeitenPharmacovigilance: A Worldwide Master Key For Drug Safety MonitoringAbbey Joy CollanoNoch keine Bewertungen
- Equity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiDokument34 SeitenEquity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiEjemai EboreimeNoch keine Bewertungen
- Food Control System Assessment Tool: Dimension B – Control FunctionsVon EverandFood Control System Assessment Tool: Dimension B – Control FunctionsNoch keine Bewertungen
- Food Control System Assessment Tool: Introduction and GlossaryVon EverandFood Control System Assessment Tool: Introduction and GlossaryNoch keine Bewertungen
- Legal Writing Notes KoDokument28 SeitenLegal Writing Notes KoMaria roxanne HernandezNoch keine Bewertungen
- 5.2 Renal Masses and Congenital AnomaliesDokument9 Seiten5.2 Renal Masses and Congenital AnomaliesMaria roxanne HernandezNoch keine Bewertungen
- Legal Research Notes KoDokument14 SeitenLegal Research Notes KoMaria roxanne HernandezNoch keine Bewertungen
- Amo - Registration Form.7.18.19Dokument1 SeiteAmo - Registration Form.7.18.19Maria roxanne HernandezNoch keine Bewertungen
- JB Al Khuwair In-Store CSAT Survey Consolidator Ver 3Dokument2.278 SeitenJB Al Khuwair In-Store CSAT Survey Consolidator Ver 3Maria roxanne HernandezNoch keine Bewertungen
- Amo - Registration Form.7.18.19Dokument1 SeiteAmo - Registration Form.7.18.19Maria roxanne HernandezNoch keine Bewertungen
- WHRB4.4 GovernanceDokument1 SeiteWHRB4.4 GovernanceMaria roxanne HernandezNoch keine Bewertungen
- WHRB4.1 FinancingDokument1 SeiteWHRB4.1 FinancingMaria roxanne HernandezNoch keine Bewertungen
- WHRB4.3 RegulationDokument1 SeiteWHRB4.3 RegulationMaria roxanne HernandezNoch keine Bewertungen
- Health Research Brief: Combatting Stubborn Pathogens: Strengthening Surveillance On Antimicrobial ResistanceDokument2 SeitenHealth Research Brief: Combatting Stubborn Pathogens: Strengthening Surveillance On Antimicrobial ResistanceMaria roxanne HernandezNoch keine Bewertungen
- LAMAGNA, Rose Solangon Re: Appointment University President Age Limit Query X - X Resolution NoDokument4 SeitenLAMAGNA, Rose Solangon Re: Appointment University President Age Limit Query X - X Resolution NoMaria roxanne HernandezNoch keine Bewertungen
- ResearchDokument6 SeitenResearchDomNoch keine Bewertungen
- Tama Naaaaaaa NiiiiiiiiiiiDokument123 SeitenTama Naaaaaaa NiiiiiiiiiiiLeslie Ann Pulvera MesolisNoch keine Bewertungen
- 9.2. Sampling Distributions: Properties ofDokument9 Seiten9.2. Sampling Distributions: Properties ofchalachew77Noch keine Bewertungen
- 1 Defining Social Sciences PDFDokument2 Seiten1 Defining Social Sciences PDFCarla villalva100% (2)
- 2549 5147 1 SM PDFDokument8 Seiten2549 5147 1 SM PDFNurul AisyahNoch keine Bewertungen
- AnovaDokument47 SeitenAnovaagumasNoch keine Bewertungen
- How Organizational Culture Shapes CompetitiveDokument14 SeitenHow Organizational Culture Shapes CompetitiveHao Wu100% (1)
- 3 Types of Nursing Research PDFDokument2 Seiten3 Types of Nursing Research PDFPxPPxH ChanNoch keine Bewertungen
- Online Drug Trade - A Threat To Pharmaceutical IndustryDokument6 SeitenOnline Drug Trade - A Threat To Pharmaceutical Industrydr duglusNoch keine Bewertungen
- Locating Credible Databases and ResearchDokument7 SeitenLocating Credible Databases and ResearchTrex WritersNoch keine Bewertungen
- Factors Affecting The English Proficiency of Grade 10 Students at Manggitahan National High School"Dokument42 SeitenFactors Affecting The English Proficiency of Grade 10 Students at Manggitahan National High School"Ben MoradoNoch keine Bewertungen
- CVDokument3 SeitenCVAbdullah Al MamunNoch keine Bewertungen
- Sampling Technique and Data Collection Method in Qualitative ResearchDokument2 SeitenSampling Technique and Data Collection Method in Qualitative ResearchErica NapigkitNoch keine Bewertungen
- Sleep Deprivation and Its Effect On The Productivity of Selected Grade 10 StudentsDokument50 SeitenSleep Deprivation and Its Effect On The Productivity of Selected Grade 10 StudentslindrendonNoch keine Bewertungen
- Thesis On Road Accident in GhanaDokument5 SeitenThesis On Road Accident in Ghanaafcnftqep100% (2)
- Experimental Psychology and The Scientific Method: Instructor: Mr. Omar T. BualanDokument22 SeitenExperimental Psychology and The Scientific Method: Instructor: Mr. Omar T. BualanAndrea JonNoch keine Bewertungen
- 8th FLC Booklet PDFDokument93 Seiten8th FLC Booklet PDFBelinda AngelNoch keine Bewertungen
- Curriculum and Instruction Thesis TopicsDokument7 SeitenCurriculum and Instruction Thesis Topicsvaj0demok1w2100% (2)
- Social Studies Lesson Plan 6Dokument2 SeitenSocial Studies Lesson Plan 6api-296600328Noch keine Bewertungen
- Brainstorming For Research TopicsDokument18 SeitenBrainstorming For Research TopicsMa. Aiza SantosNoch keine Bewertungen
- Delta MethodDokument11 SeitenDelta MethodRaja Fawad ZafarNoch keine Bewertungen
- EPRI Repair & Replacement Apps Center - Socket Weld Repair Issues 1013562Dokument20 SeitenEPRI Repair & Replacement Apps Center - Socket Weld Repair Issues 1013562Claudia Mms100% (1)
- Performance Evaluation Form: Work PlanningDokument2 SeitenPerformance Evaluation Form: Work Planningsusheelkumar5Noch keine Bewertungen
- Kurva Kalibrasi (Soal AAS) : JawabanDokument5 SeitenKurva Kalibrasi (Soal AAS) : JawabanDoni DermawanNoch keine Bewertungen
- Awareness and Perception of HousewivesDokument9 SeitenAwareness and Perception of HousewivesChrislyn CalinggalNoch keine Bewertungen
- ChebyshevDokument3 SeitenChebyshevMajid Khammas NeamahNoch keine Bewertungen
- Identity Theory and Personality Theory: Mutual Relevance - Sheldon StrykerDokument24 SeitenIdentity Theory and Personality Theory: Mutual Relevance - Sheldon StrykerRemyNoch keine Bewertungen