Das könnte Ihnen auch gefallen
- IBSL Life - EnglishDokument34 SeitenIBSL Life - EnglishShameer Sahir100% (8)
- NLA Assured Shorthold Tenancy AgreementDokument8 SeitenNLA Assured Shorthold Tenancy AgreementGaurav JainNoch keine Bewertungen
- Employee State Insurance Corporation: Form 12 (Regulation 68) E.S.I. Corporation Accident ReportDokument2 SeitenEmployee State Insurance Corporation: Form 12 (Regulation 68) E.S.I. Corporation Accident ReportVeeruKumarKondepudi67% (3)
- Pre-Employment Medical ExaminationDokument4 SeitenPre-Employment Medical ExaminationRohit Chaudhary100% (1)
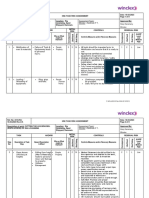
- Cutting Rig Bracing Risk AssessmentDokument9 SeitenCutting Rig Bracing Risk AssessmentHafeez AliNoch keine Bewertungen
- Codification Reference Guide (KPMG) (00663376)Dokument3 SeitenCodification Reference Guide (KPMG) (00663376)bencho10150% (2)
- Form-12 Accident Report From EmployerDokument2 SeitenForm-12 Accident Report From EmployersupriyaNoch keine Bewertungen
- Employee State Insurance Corporation: Form 12 (Regulation 68) E.S.I. Corporation Accident ReportDokument3 SeitenEmployee State Insurance Corporation: Form 12 (Regulation 68) E.S.I. Corporation Accident Reportjaydeepaagja50% (2)
- Employee Medical Incident ReportDokument1 SeiteEmployee Medical Incident ReportAiswarya SukumarNoch keine Bewertungen
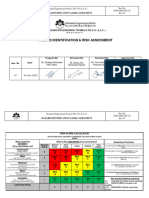
- Hazard Identification and Risk Assessment (Hira)Dokument1 SeiteHazard Identification and Risk Assessment (Hira)dellaadlinaNoch keine Bewertungen
- Risk Assessment Working at HeightsDokument8 SeitenRisk Assessment Working at Heightscontrax8Noch keine Bewertungen
- (Sample) Completion of Works CertificateDokument1 Seite(Sample) Completion of Works CertificateFredrick Omondi OleweNoch keine Bewertungen
- BSD - 019 Bulk EarthworksDokument3 SeitenBSD - 019 Bulk EarthworksZakkaudin KhanNoch keine Bewertungen
- Bidaa Tower Risk Assessment From CALISTO UpdatedDokument5 SeitenBidaa Tower Risk Assessment From CALISTO Updatedirshad gNoch keine Bewertungen
- 9.risk Assessment - Working in PantryDokument2 Seiten9.risk Assessment - Working in PantryManzur AhmadNoch keine Bewertungen
- Report of An Injury or Dangerous Occurrence: Part A Part CDokument2 SeitenReport of An Injury or Dangerous Occurrence: Part A Part CVeronica Navarro CorbiNoch keine Bewertungen
- Risk Assessment for Scaffolding WorkDokument5 SeitenRisk Assessment for Scaffolding WorkAejaz MujawarNoch keine Bewertungen
- 4.risk Assessment For PPM-Water HeaterDokument2 Seiten4.risk Assessment For PPM-Water HeaterManzur AhmadNoch keine Bewertungen
- Accident Incident Report FormDokument3 SeitenAccident Incident Report FormTuan NguyenNoch keine Bewertungen
- Loading and unloading AAc blocksDokument18 SeitenLoading and unloading AAc blocksAmit BhattNoch keine Bewertungen
- Plant and Equipment Risk Assessment Fgoc - NewDokument13 SeitenPlant and Equipment Risk Assessment Fgoc - Newmajid khanNoch keine Bewertungen
- 1.18 Incident Reporting and Investigation ProcedureDokument5 Seiten1.18 Incident Reporting and Investigation ProcedureDayasatee kodyeNoch keine Bewertungen
- 01 WI HSE 001 - Risk Assessment BridgesDokument8 Seiten01 WI HSE 001 - Risk Assessment BridgesMisbah Ul Haq LabeedNoch keine Bewertungen
- RISK-REGISTERDokument2 SeitenRISK-REGISTERعمرو100% (1)
- Working On HeightsDokument5 SeitenWorking On HeightsgrantNoch keine Bewertungen
- CTRA-23-STM-146 - TK - 11-995 - HotWorkDokument3 SeitenCTRA-23-STM-146 - TK - 11-995 - HotWorkMohamed RizwanNoch keine Bewertungen
- FCU Quarterly PPM: Risk Assessment (Ra) FormDokument2 SeitenFCU Quarterly PPM: Risk Assessment (Ra) FormRAJ CHAUDHARYNoch keine Bewertungen
- Risk Assessment - Hot WorkDokument6 SeitenRisk Assessment - Hot Workabdullah ashrafNoch keine Bewertungen
- Updated - Risk Assessment - Preventive Maintenance at REMELT AREADokument13 SeitenUpdated - Risk Assessment - Preventive Maintenance at REMELT AREAKareem MohamedNoch keine Bewertungen
- Risk Assesment Fab - Rev-07Dokument71 SeitenRisk Assesment Fab - Rev-07Nikhil PuthiryNoch keine Bewertungen
- Hiradc - Hot WorkDokument4 SeitenHiradc - Hot WorkAlieya MustafaNoch keine Bewertungen
- Job Safety Analysis (Jsa) N2.Dokument5 SeitenJob Safety Analysis (Jsa) N2.Joseph Paul IlaganNoch keine Bewertungen
- HiraDokument18 SeitenHiraPanchdev KumarNoch keine Bewertungen
- Risk Assessment - Glazing PDFDokument3 SeitenRisk Assessment - Glazing PDFAngel GrospeNoch keine Bewertungen
- Job Cycle Check Plan 2019: Sr. No Work Order # Plant Asset Number Asset DescriptionDokument4 SeitenJob Cycle Check Plan 2019: Sr. No Work Order # Plant Asset Number Asset DescriptionHamza NoumanNoch keine Bewertungen
- RA - Fire Alarm SystemDokument12 SeitenRA - Fire Alarm Systemvelangi rajuNoch keine Bewertungen
- Chaliyama Steel Plant-Rungta Mines Limited Hazard Identification & Risk AssessmentDokument4 SeitenChaliyama Steel Plant-Rungta Mines Limited Hazard Identification & Risk AssessmentCPP EI DSpNoch keine Bewertungen
- Hazard Identification & Risk Assessment FormDokument3 SeitenHazard Identification & Risk Assessment FormChandra Shekar EmaniNoch keine Bewertungen
- OHS-PR-09-03-F02 HIRA - 002 Marking and Layout of Site Being Surveyed Rev. 2021Dokument11 SeitenOHS-PR-09-03-F02 HIRA - 002 Marking and Layout of Site Being Surveyed Rev. 2021MuhammadAsimMuneerNoch keine Bewertungen
- OHS-PR-09-03-F02 HIRA - 005 Access Road and Structure Pad Preparation For Plain AreaDokument10 SeitenOHS-PR-09-03-F02 HIRA - 005 Access Road and Structure Pad Preparation For Plain AreaJaafar LagayanNoch keine Bewertungen
- QHSE Manual: Document NameDokument3 SeitenQHSE Manual: Document NameFarhanNoch keine Bewertungen
- Risk Assessment-Workplace TransportDokument7 SeitenRisk Assessment-Workplace TransportStelaNoch keine Bewertungen
- PPE Survey ResultsDokument2 SeitenPPE Survey Resultsahmed naveed100% (1)
- Visitor Safety BriefingDokument2 SeitenVisitor Safety BriefingDoni TriatmojoNoch keine Bewertungen
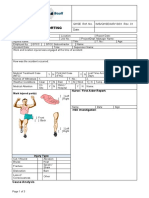
- 31.0.10 LLA - Manual HandlingDokument4 Seiten31.0.10 LLA - Manual HandlingGerritNoch keine Bewertungen
- OHS-PR-09-03-F02 HIRA - 005 Light Materials and Equipment Loading - Unloading Rev. 2021Dokument6 SeitenOHS-PR-09-03-F02 HIRA - 005 Light Materials and Equipment Loading - Unloading Rev. 2021MuhammadAsimMuneerNoch keine Bewertungen
- Accident Incident Report (TLS)Dokument2 SeitenAccident Incident Report (TLS)jonesNoch keine Bewertungen
- Medical History and Evaluation FormDokument22 SeitenMedical History and Evaluation FormJobelle Fernandez-SantosNoch keine Bewertungen
- JSa For Glass FixingDokument17 SeitenJSa For Glass FixingShekh BabulNoch keine Bewertungen
- Risk Assessment - Concrete PouringDokument6 SeitenRisk Assessment - Concrete Pouringabdullah ashrafNoch keine Bewertungen
- 106 - Risk AssessmentDokument6 Seiten106 - Risk AssessmentAravind Sasi Kumar100% (1)
- Monthly Mass Meeting Agenda + Invitation 12 PageDokument1 SeiteMonthly Mass Meeting Agenda + Invitation 12 PageamitNoch keine Bewertungen
- Indian Oil Corporation Limited Job Safety Analysis for Core Cutting WorkDokument11 SeitenIndian Oil Corporation Limited Job Safety Analysis for Core Cutting WorkOmkar Mishra100% (1)
- Daily HSE ReportDokument4 SeitenDaily HSE ReportSayeed MalikNoch keine Bewertungen
- GEN-021 Fact FindingDokument3 SeitenGEN-021 Fact Findingacanbasri1980Noch keine Bewertungen
- Risk Assessment FormDokument4 SeitenRisk Assessment FormFrankie FryNoch keine Bewertungen
- 31.HIRA - Boom Placer OperationDokument3 Seiten31.HIRA - Boom Placer OperationMMRDACA07 SAFETYNoch keine Bewertungen
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADokument2 SeitenIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky Bis100% (1)
- Ra For Hot Work (Welding & Cutting Works)Dokument3 SeitenRa For Hot Work (Welding & Cutting Works)Abrar AhmedNoch keine Bewertungen
- 2.8c Risk Assessment - 023 Scaffolding Erection, Dismantling, Modification Rev. July 2019Dokument9 Seiten2.8c Risk Assessment - 023 Scaffolding Erection, Dismantling, Modification Rev. July 2019Shah MuzzamilNoch keine Bewertungen
- Safety Hazard and Risk Assessment Form - DrillingDokument1 SeiteSafety Hazard and Risk Assessment Form - DrillingWan Aiman Wan Kamarul AzwanNoch keine Bewertungen
- Working at Same Levels (High Risk Areas) RA-R9-01-001-02Dokument1 SeiteWorking at Same Levels (High Risk Areas) RA-R9-01-001-02cmrig74Noch keine Bewertungen
- Hazard Identification and Risk Analysis in Mining: Case Studies of an Iron Ore and Coal MineDokument84 SeitenHazard Identification and Risk Analysis in Mining: Case Studies of an Iron Ore and Coal MineZarimi Ac100% (1)
- A. Factors Are The Numbers That Are Multiplied To Give A ProductDokument1 SeiteA. Factors Are The Numbers That Are Multiplied To Give A ProductsupriyaNoch keine Bewertungen
- Area 2Dokument1 SeiteArea 2supriyaNoch keine Bewertungen
- Area 1Dokument1 SeiteArea 1supriyaNoch keine Bewertungen
- Gaurav SharmaDokument3 SeitenGaurav SharmasupriyaNoch keine Bewertungen
- Rohit Kumar 2023 CVDokument3 SeitenRohit Kumar 2023 CVsupriyaNoch keine Bewertungen
- Naukri SANGAMDWIVEDI (5y 0m)Dokument3 SeitenNaukri SANGAMDWIVEDI (5y 0m)supriyaNoch keine Bewertungen
- ResumeDokument5 SeitenResumesupriyaNoch keine Bewertungen
- 5th Grade Factors and Multiples WorksheetsDokument5 Seiten5th Grade Factors and Multiples WorksheetssupriyaNoch keine Bewertungen
- UPDATED CV-Neeraj KR - Sharma-2021.Dokument5 SeitenUPDATED CV-Neeraj KR - Sharma-2021.supriyaNoch keine Bewertungen
- Subhankar Sarkar (Photo) ExperienceDokument2 SeitenSubhankar Sarkar (Photo) ExperiencesupriyaNoch keine Bewertungen
- Insurance Professional Resume Jaya PammelaDokument2 SeitenInsurance Professional Resume Jaya PammelasupriyaNoch keine Bewertungen
- Curriculum Vitae Renu Pal: (Assistant Architect)Dokument3 SeitenCurriculum Vitae Renu Pal: (Assistant Architect)supriyaNoch keine Bewertungen
- Shivam 5555@yahoo Dotco DotinDokument3 SeitenShivam 5555@yahoo Dotco DotinsupriyaNoch keine Bewertungen
- Lokesh Agarwal resume SEODokument2 SeitenLokesh Agarwal resume SEOsupriyaNoch keine Bewertungen
- India's Wellness Partner Since 2003Dokument2 SeitenIndia's Wellness Partner Since 2003supriyaNoch keine Bewertungen
- WindowDokument1 SeiteWindowsupriyaNoch keine Bewertungen
- Jitendra PalDokument2 SeitenJitendra PalsupriyaNoch keine Bewertungen
- Formula of Simple Future TenseDokument8 SeitenFormula of Simple Future Tensesupriya100% (1)
- Tenses Rules Chart For Class 5Dokument1 SeiteTenses Rules Chart For Class 5supriyaNoch keine Bewertungen
- NCERT Solutions for Class 5 English Ice Cream ManDokument7 SeitenNCERT Solutions for Class 5 English Ice Cream MansupriyaNoch keine Bewertungen
- Chandrashekhar N Patwari: Curriculum VitaeDokument5 SeitenChandrashekhar N Patwari: Curriculum VitaesupriyaNoch keine Bewertungen
- Curriculam Vitae: Ankur Sharma Mechanical Engineer (Design & Process Department)Dokument3 SeitenCurriculam Vitae: Ankur Sharma Mechanical Engineer (Design & Process Department)supriyaNoch keine Bewertungen
- ChapterDokument4 SeitenChaptersupriyaNoch keine Bewertungen
- Increase factory manpower strength notificationDokument1 SeiteIncrease factory manpower strength notificationsupriyaNoch keine Bewertungen
- Deepa ThakurDokument2 SeitenDeepa ThakursupriyaNoch keine Bewertungen
- Shubham RustogiDokument2 SeitenShubham RustogisupriyaNoch keine Bewertungen
- Sudhanshu Kumar: Oldcrete Infra Products RMCDokument2 SeitenSudhanshu Kumar: Oldcrete Infra Products RMCsupriyaNoch keine Bewertungen
- Happy To Help Rs 267.09 19.12.12: Vodafone No. 9962985002Dokument5 SeitenHappy To Help Rs 267.09 19.12.12: Vodafone No. 9962985002supriyaNoch keine Bewertungen
- Rajeev Kumar Jha: E-Mail: Mobile No: +91 8800949284Dokument2 SeitenRajeev Kumar Jha: E-Mail: Mobile No: +91 8800949284supriyaNoch keine Bewertungen
- Ranjan M AnandDokument4 SeitenRanjan M AnandsupriyaNoch keine Bewertungen
- List of Registrars and Their Client CompaniesDokument7 SeitenList of Registrars and Their Client CompaniesSamson SayNoch keine Bewertungen
- Summer Training Report on Training & Development at Principal PNB Mutual FundDokument97 SeitenSummer Training Report on Training & Development at Principal PNB Mutual Fundsksharma55100% (1)
- GST NotesDokument361 SeitenGST NotesDamodar SejpalNoch keine Bewertungen
- Annual Report13Dokument64 SeitenAnnual Report13Hoa PhươngNoch keine Bewertungen
- Standard Form of ContractDokument2 SeitenStandard Form of ContractKanikaNoch keine Bewertungen
- An Investigation On The Determinants of Life Assurance Products Uptake in ZimbabweDokument10 SeitenAn Investigation On The Determinants of Life Assurance Products Uptake in ZimbabweDynamic Research JournalsNoch keine Bewertungen
- Retrospective Why Do CustomerDokument8 SeitenRetrospective Why Do CustomerJar JarNoch keine Bewertungen
- Fidic Red BookDokument24 SeitenFidic Red BookDipankar Dutta100% (1)
- Loadstar Shipping Co Vs Pioneer Asia Insurance - G.R. No. 157481. January 24, 2006Dokument5 SeitenLoadstar Shipping Co Vs Pioneer Asia Insurance - G.R. No. 157481. January 24, 2006Ebbe DyNoch keine Bewertungen
- OAITA's Response Memorandum To ODI Motion For Summary JudgmentDokument18 SeitenOAITA's Response Memorandum To ODI Motion For Summary JudgmentOAITANoch keine Bewertungen
- Data Warehouse TypesDokument6 SeitenData Warehouse TypesCxHNoch keine Bewertungen
- PRO0750 Smart Value Income Plan BrochureDokument10 SeitenPRO0750 Smart Value Income Plan BrochureJignesh PatelNoch keine Bewertungen
- Kairos Academies Food Program Request For ProposalDokument28 SeitenKairos Academies Food Program Request For ProposalGavin SchiffresNoch keine Bewertungen
- Marketing and Sales of Insurance Products: University of Mumbai Project OnDokument6 SeitenMarketing and Sales of Insurance Products: University of Mumbai Project Onyesh cyberNoch keine Bewertungen
- SBI Two Wheeler Insurance Policy DetailsDokument14 SeitenSBI Two Wheeler Insurance Policy Detailsmithalesh kumarNoch keine Bewertungen
- Income TaxationDokument32 SeitenIncome TaxationkarlNoch keine Bewertungen
- Life Insurance Claim Management GuideDokument66 SeitenLife Insurance Claim Management GuideKARAN CHIKATENoch keine Bewertungen
- Pouran Abdipour Converted ResumeDokument2 SeitenPouran Abdipour Converted ResumepouranpouranNoch keine Bewertungen
- About IMT 47 in Motor - Analysis in DetailDokument5 SeitenAbout IMT 47 in Motor - Analysis in DetailNaishadh J Desai AnD'sNoch keine Bewertungen
- Prudential PLCDokument5 SeitenPrudential PLCPedro CáceresNoch keine Bewertungen
- Insurance Surveyors GuideDokument16 SeitenInsurance Surveyors Guideepicky4013Noch keine Bewertungen
- 02 Kanto Region (Kaigofukushishi) 12000014Dokument4 Seiten02 Kanto Region (Kaigofukushishi) 12000014bnp2tkidotgodotidNoch keine Bewertungen
- Business StudiesDokument2 SeitenBusiness StudiesSonal JhaNoch keine Bewertungen
- Brief Scope of WorkDokument19 SeitenBrief Scope of Workapi-369899683% (6)
- Security Bank & Trust Company vs. Cuenca PDFDokument46 SeitenSecurity Bank & Trust Company vs. Cuenca PDFRogie ApoloNoch keine Bewertungen
- Mallya - Notice To RBI GovernorDokument84 SeitenMallya - Notice To RBI GovernorNagaraja Mysuru RaghupathiNoch keine Bewertungen
- D 1 FHDokument12 SeitenD 1 FHfede444Noch keine Bewertungen