Das könnte Ihnen auch gefallen
- Dialysis Guide 2012Dokument12 SeitenDialysis Guide 2012nadhifNoch keine Bewertungen
- Jama Sha 2019 It 190019Dokument2 SeitenJama Sha 2019 It 190019xtineNoch keine Bewertungen
- Shahar Nissan2020Dokument7 SeitenShahar Nissan2020orelysNoch keine Bewertungen
- Immunization Guide by Dr Shibambu PatrickDokument48 SeitenImmunization Guide by Dr Shibambu PatrickPatrick ShibambuNoch keine Bewertungen
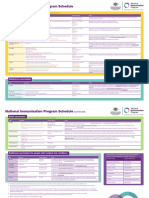
- National Immunisation Program ScheduleDokument2 SeitenNational Immunisation Program Schedulesophile660Noch keine Bewertungen
- Preventing and Treating Infections in Children With Asplenia or HypospleniaDokument5 SeitenPreventing and Treating Infections in Children With Asplenia or HypospleniaAmélieNoch keine Bewertungen
- Adult ScheduleDokument3 SeitenAdult ScheduleerilarchiNoch keine Bewertungen
- Calendario Vacunacion Adultos 2010Dokument4 SeitenCalendario Vacunacion Adultos 2010JOSERUPOLONoch keine Bewertungen
- Febrile Seizure Risk After Vaccination in Children 6 To 23 MonthsDokument12 SeitenFebrile Seizure Risk After Vaccination in Children 6 To 23 MonthsrfNoch keine Bewertungen
- Almostadoctor - Co.uk-Vaccination Schedule UKDokument6 SeitenAlmostadoctor - Co.uk-Vaccination Schedule UKIbrahim FoondunNoch keine Bewertungen
- Adult VaccinesDokument3 SeitenAdult VaccinesJohn DoeNoch keine Bewertungen
- Immune Responses To Measles and Mumps Vaccination of Infants at 6, 9, and 12 MonthsDokument10 SeitenImmune Responses To Measles and Mumps Vaccination of Infants at 6, 9, and 12 MonthsManiru Aliyu GiganeNoch keine Bewertungen
- Pertussis Fact Sheet: National Centre For Immunisation Research and SurvelianceDokument4 SeitenPertussis Fact Sheet: National Centre For Immunisation Research and SurveliancePaul GallagherNoch keine Bewertungen
- Acog Committee Opinion: Maternal ImmunizationDokument4 SeitenAcog Committee Opinion: Maternal Immunizationfelix camposNoch keine Bewertungen
- Vaccinations in PregnancyDokument137 SeitenVaccinations in PregnancyAmine YounisNoch keine Bewertungen
- Immunization DR T V RaoDokument68 SeitenImmunization DR T V Raotummalapalli venkateswara rao100% (1)
- Varicella Post-ProphylaxisDokument2 SeitenVaricella Post-ProphylaxisAngelaTrinidadNoch keine Bewertungen
- Varicella Vaccine Effectiveness Over 10 Years in Australia - 2019 - Journal ofDokument6 SeitenVaricella Vaccine Effectiveness Over 10 Years in Australia - 2019 - Journal ofNihad MalikzadeNoch keine Bewertungen
- Vaccinations for Pregnant Women: Which Are SafeDokument1 SeiteVaccinations for Pregnant Women: Which Are SafeShama Gautam PatelNoch keine Bewertungen
- MMR 2 Vaccine InsertDokument11 SeitenMMR 2 Vaccine InsertJonNoch keine Bewertungen
- Children's Medicines: What Parents Need to Know About VaccinesDokument16 SeitenChildren's Medicines: What Parents Need to Know About VaccinesJonathanNoch keine Bewertungen
- Immunization Review GPDokument46 SeitenImmunization Review GPKishore ChandkiNoch keine Bewertungen
- Adult ScheduleDokument3 SeitenAdult SchedulelcmurilloNoch keine Bewertungen
- VaccinesDokument8 SeitenVaccinesRayNoch keine Bewertungen
- A Vaccine For MalariaDokument2 SeitenA Vaccine For MalariaArcciPradessatamaNoch keine Bewertungen
- EPI Vaccines Revised Oct 2010Dokument18 SeitenEPI Vaccines Revised Oct 2010Jei JayNoch keine Bewertungen
- Monkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowDokument7 SeitenMonkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowariniNoch keine Bewertungen
- 7-18yr Schedule For Immunizations, CDC 2008Dokument1 Seite7-18yr Schedule For Immunizations, CDC 2008Tracy100% (1)
- Epi Brochure (Calalang)Dokument2 SeitenEpi Brochure (Calalang)Nickaela CalalangNoch keine Bewertungen
- Partial CHN211 Week 7Dokument16 SeitenPartial CHN211 Week 7Via Kristel ZapantaNoch keine Bewertungen
- Acellular Pertussis Vaccine Effectiveness Over Time: ObjectivesDokument11 SeitenAcellular Pertussis Vaccine Effectiveness Over Time: Objectives[JC]Noch keine Bewertungen
- Hoes 2022Dokument11 SeitenHoes 2022contreraz7Noch keine Bewertungen
- 9.2018. Updates On Tdap Vaccination During PregnancyDokument2 Seiten9.2018. Updates On Tdap Vaccination During Pregnancyrosatikah ahmadNoch keine Bewertungen
- Acellular Pertussis Vaccine Effectiveness Over Time: ObjectivesDokument11 SeitenAcellular Pertussis Vaccine Effectiveness Over Time: ObjectivesLee제노Noch keine Bewertungen
- Summary of Key Points WHO Position Paper On Vaccines Against Diphtheria, August 2017Dokument12 SeitenSummary of Key Points WHO Position Paper On Vaccines Against Diphtheria, August 2017Bill BillyNoch keine Bewertungen
- VacinationDokument10 SeitenVacinationMostafa Ibrahim AhmedNoch keine Bewertungen
- Maternal VaccinationDokument16 SeitenMaternal VaccinationAnonymous l6Q1ROq2Noch keine Bewertungen
- Immunization and Prophylaxis: Childhood Immunization Has Reduced The Impact - Active Immunization Is TheDokument18 SeitenImmunization and Prophylaxis: Childhood Immunization Has Reduced The Impact - Active Immunization Is TheCabdiNoch keine Bewertungen
- Vaccinations For Pregnant Women: Vaccine Do You Need It During Your Pregnancy?Dokument1 SeiteVaccinations For Pregnant Women: Vaccine Do You Need It During Your Pregnancy?sangmavideo officialNoch keine Bewertungen
- Schaefer 2017Dokument6 SeitenSchaefer 2017hasemana hasemanaNoch keine Bewertungen
- Immunisation Schedule July 2018Dokument5 SeitenImmunisation Schedule July 2018evatangNoch keine Bewertungen
- Mourtzoukou Et Al-2008-British Journal of SurgeryDokument8 SeitenMourtzoukou Et Al-2008-British Journal of SurgeryTony AdeosunNoch keine Bewertungen
- Community Health Nursing Expanded Program On ImmunizationDokument11 SeitenCommunity Health Nursing Expanded Program On ImmunizationRaymond EdgeNoch keine Bewertungen
- Adult ImmunizationDokument6 SeitenAdult ImmunizationAmit GoelNoch keine Bewertungen
- Vaccine Indication and ContraindicationDokument34 SeitenVaccine Indication and ContraindicationMusa yohanaNoch keine Bewertungen
- Nejm VaricellaDokument9 SeitenNejm VaricellaadityailhamNoch keine Bewertungen
- 1 Immunization جمعت كل مهم هناDokument13 Seiten1 Immunization جمعت كل مهم هناReem 10Noch keine Bewertungen
- HexaximeDokument12 SeitenHexaximekanharitNoch keine Bewertungen
- Immunizations To Be Taken On Gandako'S First VisitDokument5 SeitenImmunizations To Be Taken On Gandako'S First VisitKryzza LeizellNoch keine Bewertungen
- fimmu-11-00555Dokument14 Seitenfimmu-11-00555Paula VargasNoch keine Bewertungen
- Stay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartDokument4 SeitenStay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartcircularreasoningNoch keine Bewertungen
- Varicella During Pregnancy: A Case ReportDokument3 SeitenVaricella During Pregnancy: A Case ReportCosmin RăileanuNoch keine Bewertungen
- Immunization ScheduleDokument2 SeitenImmunization ScheduleTracy100% (1)
- The Optimal Strategy For Pertussis Vaccination: A Systematic Review and Meta-Analysis of Randomized Control Trials and Real-World DataDokument26 SeitenThe Optimal Strategy For Pertussis Vaccination: A Systematic Review and Meta-Analysis of Randomized Control Trials and Real-World DataIdmNoch keine Bewertungen
- Rotavirus Vaccines For Infants - 2019 - UptodateDokument26 SeitenRotavirus Vaccines For Infants - 2019 - Uptodatewinnie MontalvoNoch keine Bewertungen
- 2 Review Diphtheria Results April2017 Final Clean PDFDokument20 Seiten2 Review Diphtheria Results April2017 Final Clean PDFchameleonNoch keine Bewertungen
- Vaccination of HIV Infected Children 2018Dokument4 SeitenVaccination of HIV Infected Children 2018alpha.blocker11Noch keine Bewertungen
- IAHS Immunization in TanzaniaDokument5 SeitenIAHS Immunization in TanzaniaMasali MacdonaNoch keine Bewertungen
- Health Advice and Immunizations for TravelersVon EverandHealth Advice and Immunizations for TravelersNoch keine Bewertungen
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsVon EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsBewertung: 5 von 5 Sternen5/5 (9)
- List of Medical Tests For Saudi Visa - Life in Saudi ArabiaDokument9 SeitenList of Medical Tests For Saudi Visa - Life in Saudi Arabiakillerhigh100% (2)
- FECALYSIS, Perianal SwabDokument20 SeitenFECALYSIS, Perianal SwabMarron MonsaludNoch keine Bewertungen
- Icmr PPT (1) VidhiDokument32 SeitenIcmr PPT (1) VidhiVidhi GuptaNoch keine Bewertungen
- NicuuuuDokument17 SeitenNicuuuuJyoti Prem UttamNoch keine Bewertungen
- Ocd, Normal IntrusionsDokument3 SeitenOcd, Normal Intrusionscitalac69Noch keine Bewertungen
- Acute Rehabilitation Program After Laparoscopic Colectomy Using Intravenous LidocaineDokument6 SeitenAcute Rehabilitation Program After Laparoscopic Colectomy Using Intravenous LidocaineKu Badlisyah Ku AzizNoch keine Bewertungen
- Promoting Hygiene Through Complete BathingDokument12 SeitenPromoting Hygiene Through Complete BathingErlangga PratamaNoch keine Bewertungen
- Biology Chapter 40-1 Infectious DiseasesDokument23 SeitenBiology Chapter 40-1 Infectious Diseasesapi-239353579Noch keine Bewertungen
- Master Techniques in Surgery Esophageal Surgery 20 PDFDokument598 SeitenMaster Techniques in Surgery Esophageal Surgery 20 PDFDima Nestor100% (2)
- Nursing care plan SARSDokument5 SeitenNursing care plan SARSRhea Princess Tadeo88% (8)
- Pelvic Floor Distress Inventory Questionnaire - Short Form 20Dokument2 SeitenPelvic Floor Distress Inventory Questionnaire - Short Form 20Dana Ysabelle Ibarra100% (1)
- cc1 LecDokument18 Seitencc1 LecRayvince LopezNoch keine Bewertungen
- Keshe Resmi Agri Kalemi Kullanim Klavuzu - EsraIDokument2 SeitenKeshe Resmi Agri Kalemi Kullanim Klavuzu - EsraIilkerNoch keine Bewertungen
- Care of Clients With Physiologic and Psychosocial Alterations - Doc Version 1Dokument46 SeitenCare of Clients With Physiologic and Psychosocial Alterations - Doc Version 1CLAIRE VillaviejaNoch keine Bewertungen
- Esophageal CancerDokument40 SeitenEsophageal Cancerapi-282115150Noch keine Bewertungen
- Kaolin - Pectin v2 FINALDokument2 SeitenKaolin - Pectin v2 FINALAFNoch keine Bewertungen
- Stepladder Plating Following Lower Subapical and Geniop - 2022 - Advances in OraDokument2 SeitenStepladder Plating Following Lower Subapical and Geniop - 2022 - Advances in OraГне ДзжNoch keine Bewertungen
- TergecefDokument2 SeitenTergecefianecunar100% (3)
- NCP For StrokeDokument4 SeitenNCP For StrokeJASON OGALESCONoch keine Bewertungen
- DR Sunil Maheshwari Orthopedician Ahmedabad - GooDokument1 SeiteDR Sunil Maheshwari Orthopedician Ahmedabad - GooPratik TakNoch keine Bewertungen
- Dermatologic PharmacologyDokument88 SeitenDermatologic PharmacologyAlunaficha Melody KiraniaNoch keine Bewertungen
- TLE Beauty Care Pretest Grade910Dokument4 SeitenTLE Beauty Care Pretest Grade910KENT REEVE ROSALNoch keine Bewertungen
- Drug StudyDokument5 SeitenDrug StudyRai D. MacapantonNoch keine Bewertungen
- CH 13 EXCRETION IN HUMANS - QuestionsDokument10 SeitenCH 13 EXCRETION IN HUMANS - QuestionsPranitha RaviNoch keine Bewertungen
- Gram Positive Cocci (GPC) Gram Neg (Rods GNR) Anaerobes Atypicals Classification AntibioticDokument2 SeitenGram Positive Cocci (GPC) Gram Neg (Rods GNR) Anaerobes Atypicals Classification AntibioticRami RaedNoch keine Bewertungen
- 6 Pack Sept 2013-OEC-Shock-Chapter 10 - NSPDokument23 Seiten6 Pack Sept 2013-OEC-Shock-Chapter 10 - NSPDonavon GaudetteNoch keine Bewertungen
- HOW TO USE SACRED CODES FOR HEALING AND PROSPERITYDokument14 SeitenHOW TO USE SACRED CODES FOR HEALING AND PROSPERITYnikanor1100% (2)
- Emergency Care For Patients With Hemophilia FINALDokument28 SeitenEmergency Care For Patients With Hemophilia FINALebillNoch keine Bewertungen
- Abdominal Sepsis.15Dokument8 SeitenAbdominal Sepsis.15Dario Xavier Achachi MelendezNoch keine Bewertungen
- Wound HealingDokument23 SeitenWound Healingkhadija HabibNoch keine Bewertungen