Das könnte Ihnen auch gefallen
- Systemic Response To Injury and Metabolic SupportDokument118 SeitenSystemic Response To Injury and Metabolic SupportNicole DeverasNoch keine Bewertungen
- The Metabolic and Endocrine Response To TraumaDokument4 SeitenThe Metabolic and Endocrine Response To TraumaSalvador Jimenez MagosNoch keine Bewertungen
- Adrenocorticosteroids: C39 Adrenocorticosteroids & Adrenocortical AntagonistsDokument5 SeitenAdrenocorticosteroids: C39 Adrenocorticosteroids & Adrenocortical AntagonistsHydieNoch keine Bewertungen
- 39 Adrenocorticosteroids and Andrenocortical AntagonistsDokument5 Seiten39 Adrenocorticosteroids and Andrenocortical AntagonistsJENICCA GONoch keine Bewertungen
- 4 Metabolic Response of Tissue To InjuryDokument5 Seiten4 Metabolic Response of Tissue To InjuryZllison Mae Teodoro Mangabat100% (1)
- Metabolic Trauma: (Stress ResponseDokument42 SeitenMetabolic Trauma: (Stress ResponsevisagaNoch keine Bewertungen
- 1.systemic Response To InjuryDokument64 Seiten1.systemic Response To Injuryoliyad alemayehuNoch keine Bewertungen
- Stress Hormones Physiological Stress andDokument7 SeitenStress Hormones Physiological Stress andA1 [2] ضرغام لطيف سلمان داود / مسائيNoch keine Bewertungen
- Systemic Response To Injury IDokument43 SeitenSystemic Response To Injury IPaul BudionganNoch keine Bewertungen
- Surgery NotesDokument9 SeitenSurgery NotesClaire MayNoch keine Bewertungen
- Adrenal Hormones: HydrocortisoneDokument4 SeitenAdrenal Hormones: HydrocortisoneDyanne AguilaNoch keine Bewertungen
- La Respuesta Metabolica y Endocrina Al Trauma 2023Dokument5 SeitenLa Respuesta Metabolica y Endocrina Al Trauma 2023marisol ocampoNoch keine Bewertungen
- GlucocorticoidsDokument2 SeitenGlucocorticoidsBobNoch keine Bewertungen
- Pharmacology A - NSAIDSDokument14 SeitenPharmacology A - NSAIDSselflessdoctorNoch keine Bewertungen
- Hormonal and Metabolic Response To Trauma: Learning ObjectivesDokument3 SeitenHormonal and Metabolic Response To Trauma: Learning ObjectivesderianNoch keine Bewertungen
- Respuesta Metabolica Al Trauma Cap 1 FonsecaDokument6 SeitenRespuesta Metabolica Al Trauma Cap 1 FonsecaJulio Magaña QuiñonesNoch keine Bewertungen
- Systemic Response To InjuryDokument5 SeitenSystemic Response To InjuryJohn Christopher LucesNoch keine Bewertungen
- Anti-Inflammatory DrugsDokument36 SeitenAnti-Inflammatory Drugsnezifzenu2023Noch keine Bewertungen
- Adrenocortical SteroidsDokument63 SeitenAdrenocortical SteroidsmisssarjeeNoch keine Bewertungen
- Opioid and Chemokine Receptor - Nature (2015)Dokument10 SeitenOpioid and Chemokine Receptor - Nature (2015)Hugo FalquetoNoch keine Bewertungen
- L P 3 Analgesics FinalDokument24 SeitenL P 3 Analgesics FinalZakria Al-HadadNoch keine Bewertungen
- Metabolic Response To The Stress of Critical IllnessDokument10 SeitenMetabolic Response To The Stress of Critical IllnessNguyen van ChienNoch keine Bewertungen
- Corticosteroid Adverse Effects - StatPearls - NCBI BookshelfDokument12 SeitenCorticosteroid Adverse Effects - StatPearls - NCBI Bookshelfantonio.mastrangelo.999Noch keine Bewertungen
- Anti Allergic Drugs: Abdullaev Dzhumadil, PharmdDokument21 SeitenAnti Allergic Drugs: Abdullaev Dzhumadil, PharmdRtxGaming Zone 73Noch keine Bewertungen
- Farmakologi Analgetik NSAID (Dr. Atina)Dokument56 SeitenFarmakologi Analgetik NSAID (Dr. Atina)RidhaNoch keine Bewertungen
- 2008 Rubic Et Al.Dokument9 Seiten2008 Rubic Et Al.Shivaprakash Jagalur MuttNoch keine Bewertungen
- PharmaDokument13 SeitenPharmaMARIEMIL FOLLOSONoch keine Bewertungen
- Systemic Response To Injury: Janneth T. Tan, MDDokument38 SeitenSystemic Response To Injury: Janneth T. Tan, MDkira santosNoch keine Bewertungen
- 04.02-01 Endocrine IIDokument6 Seiten04.02-01 Endocrine IIMaikka IlaganNoch keine Bewertungen
- Systemic Response To Injury & Metabolic Support: Josef S. Lim, MD, FPSGS, FPCS, PalesDokument132 SeitenSystemic Response To Injury & Metabolic Support: Josef S. Lim, MD, FPSGS, FPCS, PalesCoy NuñezNoch keine Bewertungen
- Pharma Topic 2 NotesDokument8 SeitenPharma Topic 2 NotesAshley Franceska CansanayNoch keine Bewertungen
- Chapter 36 - Adrenocortical AgentsDokument3 SeitenChapter 36 - Adrenocortical Agentskdayeon018Noch keine Bewertungen
- In Vitro Antioxidant and Anti-Inflammatory Potential ofDokument13 SeitenIn Vitro Antioxidant and Anti-Inflammatory Potential ofSabrina JonesNoch keine Bewertungen
- Articulos de HipertensionDokument18 SeitenArticulos de HipertensionUlises RaceNoch keine Bewertungen
- 文献研读 - 总结Dokument25 Seiten文献研读 - 总结s21514.laiNoch keine Bewertungen
- Anti Inflammatory and Immuno Supressive Effects of GlucocorticoidsDokument50 SeitenAnti Inflammatory and Immuno Supressive Effects of GlucocorticoidssiddardhaNoch keine Bewertungen
- Metabolic Response To The Stress of Critical IllnessDokument10 SeitenMetabolic Response To The Stress of Critical IllnessValentina bustamanteNoch keine Bewertungen
- AP Biology Endocrine Systems-0Dokument14 SeitenAP Biology Endocrine Systems-0Aamer AlmansourNoch keine Bewertungen
- The Immune System: Basis of So Much Health and Disease: 9. Control of Inflammation and ImmunityDokument5 SeitenThe Immune System: Basis of So Much Health and Disease: 9. Control of Inflammation and ImmunityDiyaa SakrNoch keine Bewertungen
- KortikosteroidDokument13 SeitenKortikosteroidayu dewiNoch keine Bewertungen
- Jais e Bruning (2017) Hypothalamic Inflammation in Obesity and Metabolic DiseaseDokument10 SeitenJais e Bruning (2017) Hypothalamic Inflammation in Obesity and Metabolic DiseaseAna Flávia SordiNoch keine Bewertungen
- Pcol MidtermsDokument13 SeitenPcol MidtermsJoyce VillanuevaNoch keine Bewertungen
- Mekanisme Kerja Hormon Dan ReseptorDokument44 SeitenMekanisme Kerja Hormon Dan ReseptorOriza Rifki RamadanNoch keine Bewertungen
- NIH Public Access: The Surgically Induced Stress ResponseDokument14 SeitenNIH Public Access: The Surgically Induced Stress ResponseBayu TrigunaNoch keine Bewertungen
- Autacoid EicosanoidDokument33 SeitenAutacoid EicosanoidAlunaficha Melody KiraniaNoch keine Bewertungen
- Nutrisi Pada Pasien Critical Ill: Oleh: Dr. SusmiatiDokument54 SeitenNutrisi Pada Pasien Critical Ill: Oleh: Dr. SusmiatiUmmu TitoNoch keine Bewertungen
- Systemic Effects of Surgical Stress:: Dr. H.R.Bhardwaj: Asif AliDokument23 SeitenSystemic Effects of Surgical Stress:: Dr. H.R.Bhardwaj: Asif Alimanzoor bhatNoch keine Bewertungen
- 1 Metabolic Response To InjuryDokument15 Seiten1 Metabolic Response To InjuryDelete AccountNoch keine Bewertungen
- Respuesta Humana Al EstresDokument10 SeitenRespuesta Humana Al EstresmorbreirNoch keine Bewertungen
- Adrenocortical Hormones: Learning ObjectivesDokument3 SeitenAdrenocortical Hormones: Learning ObjectivesMarlin Berliannanda TawayNoch keine Bewertungen
- Functional Anatomy of The Adrenal GlandDokument9 SeitenFunctional Anatomy of The Adrenal GlandPaula SchaeferNoch keine Bewertungen
- Modul Muskuloskeletal - NSAIDs 2017Dokument56 SeitenModul Muskuloskeletal - NSAIDs 2017khairunnisanurainiNoch keine Bewertungen
- Adrenal Fatigue: Enhancing Quality of Life For Patients With A Functional DisorderDokument6 SeitenAdrenal Fatigue: Enhancing Quality of Life For Patients With A Functional Disordercraig10140% (1)
- DzikirDokument76 SeitenDzikirkhairunnisanurainiNoch keine Bewertungen
- 655 FullDokument16 Seiten655 FullGhina nurulNoch keine Bewertungen
- Reviewer - MNT For Metabolic StressDokument14 SeitenReviewer - MNT For Metabolic StressimjuuNoch keine Bewertungen
- 1 PDFDokument11 Seiten1 PDFJoeljar Enciso SaraviaNoch keine Bewertungen
- Basic Biology and Clinical Aspects of InflammationVon EverandBasic Biology and Clinical Aspects of InflammationNoch keine Bewertungen
- Adult History Taking and Physical ExaminationDokument6 SeitenAdult History Taking and Physical ExaminationDoc Prince Caballero100% (1)
- Bone Growth and Growth Pattern in ChildhoodDokument6 SeitenBone Growth and Growth Pattern in ChildhoodDoc Prince CaballeroNoch keine Bewertungen
- Talk It Out Before You Say I DoDokument6 SeitenTalk It Out Before You Say I DoDoc Prince CaballeroNoch keine Bewertungen
- Panunumpa NG Propesyonal PDFDokument2 SeitenPanunumpa NG Propesyonal PDFAngelo Bonje100% (1)
- Medical Problems in AdolescentsDokument3 SeitenMedical Problems in AdolescentsDoc Prince CaballeroNoch keine Bewertungen
- CPR With AedDokument37 SeitenCPR With AedDoc Prince CaballeroNoch keine Bewertungen
- New Guidelines in Attendance Tracker SubmissionDokument1 SeiteNew Guidelines in Attendance Tracker SubmissionDoc Prince CaballeroNoch keine Bewertungen
- Grief, Mourning and BereavementDokument5 SeitenGrief, Mourning and BereavementDoc Prince Caballero100% (1)
- The Midlife: Henrietta V. Cabado-Española, MD, FPPADokument7 SeitenThe Midlife: Henrietta V. Cabado-Española, MD, FPPADoc Prince CaballeroNoch keine Bewertungen
- GI Disorders During Newborn PeriodDokument5 SeitenGI Disorders During Newborn PeriodDoc Prince CaballeroNoch keine Bewertungen
- GI Disorders During Newborn PeriodDokument5 SeitenGI Disorders During Newborn PeriodDoc Prince CaballeroNoch keine Bewertungen
- Children and Death: Dr. Chua 07/25/2013 Group 6 - Witwew!Dokument6 SeitenChildren and Death: Dr. Chua 07/25/2013 Group 6 - Witwew!Doc Prince CaballeroNoch keine Bewertungen
- Neonatal ResuscitationDokument5 SeitenNeonatal ResuscitationDoc Prince CaballeroNoch keine Bewertungen
- Current Status of The Filipino YouthDokument10 SeitenCurrent Status of The Filipino YouthDoc Prince CaballeroNoch keine Bewertungen
- Initial Care of Newborn & Newborn Screening Group 5 (Joy Marie Pillado's Conflicted Copy 2013-06-25)Dokument4 SeitenInitial Care of Newborn & Newborn Screening Group 5 (Joy Marie Pillado's Conflicted Copy 2013-06-25)Doc Prince CaballeroNoch keine Bewertungen
- Antepartum Fetal MonitoringDokument9 SeitenAntepartum Fetal MonitoringDoc Prince CaballeroNoch keine Bewertungen
- Initial Care of Newborn & Newborn Screening Group 5 (Joy Marie Pillado's Conflicted Copy 2013-06-25)Dokument4 SeitenInitial Care of Newborn & Newborn Screening Group 5 (Joy Marie Pillado's Conflicted Copy 2013-06-25)Doc Prince CaballeroNoch keine Bewertungen
- Ballard Scoring: Component Description How To IllicitDokument4 SeitenBallard Scoring: Component Description How To IllicitDoc Prince CaballeroNoch keine Bewertungen
- Principles of ImmunizationDokument4 SeitenPrinciples of ImmunizationDoc Prince CaballeroNoch keine Bewertungen
- Breastfeeding: Incisors)Dokument4 SeitenBreastfeeding: Incisors)Doc Prince CaballeroNoch keine Bewertungen
- Early and Middle AdulthoodDokument6 SeitenEarly and Middle AdulthoodDoc Prince CaballeroNoch keine Bewertungen
- The Midlife: Henrietta V. Cabado-Española, MD, FPPADokument7 SeitenThe Midlife: Henrietta V. Cabado-Española, MD, FPPADoc Prince CaballeroNoch keine Bewertungen
- Current Status of The Filipino YouthDokument10 SeitenCurrent Status of The Filipino YouthDoc Prince CaballeroNoch keine Bewertungen
- Surgical Problems in NewbornsDokument7 SeitenSurgical Problems in NewbornsDoc Prince CaballeroNoch keine Bewertungen
- Early Onset SchizophreniaDokument3 SeitenEarly Onset SchizophreniaDoc Prince CaballeroNoch keine Bewertungen
- MenopauseDokument9 SeitenMenopauseDoc Prince CaballeroNoch keine Bewertungen
- Neonatal JaundiceDokument6 SeitenNeonatal JaundiceDoc Prince CaballeroNoch keine Bewertungen
- Aural Toilet Guideline1Dokument2 SeitenAural Toilet Guideline1Ariska Peradilla100% (1)
- OB Tickler 1 PDFDokument22 SeitenOB Tickler 1 PDFAnonymous de6SlW1Noch keine Bewertungen
- Evaluation Checklist Case 7 Bronchial AsthmaDokument7 SeitenEvaluation Checklist Case 7 Bronchial AsthmaChristian MendiolaNoch keine Bewertungen
- MemantineDokument7 SeitenMemantineroboNoch keine Bewertungen
- Paket 2 OkDokument5 SeitenPaket 2 OkBerna TodingNoch keine Bewertungen
- Compare Prokaryotes and Eukaryotes: Gram +ve Gram - Ve Peptidoglycan Layer Teichoic Acid Surface AntigenDokument12 SeitenCompare Prokaryotes and Eukaryotes: Gram +ve Gram - Ve Peptidoglycan Layer Teichoic Acid Surface AntigenAamir BugtiNoch keine Bewertungen
- PhilHealth Circular No. 14 S. 2018 - CF4Dokument3 SeitenPhilHealth Circular No. 14 S. 2018 - CF4Toche Doce100% (1)
- Ebook - Yoga - The Science of BreathDokument2 SeitenEbook - Yoga - The Science of BreathGabriel CiocanNoch keine Bewertungen
- Battle Mind An OverviewDokument7 SeitenBattle Mind An OverviewUzair UmairNoch keine Bewertungen
- Business Proposal SampleDokument3 SeitenBusiness Proposal SampleIan TattaoNoch keine Bewertungen
- AJODO 1993 Facial Keys To Orth DX and TX Plann Part I ARNETTDokument14 SeitenAJODO 1993 Facial Keys To Orth DX and TX Plann Part I ARNETTCarito Aguirre Lindo100% (1)
- Immediate Care of The NewbornDokument4 SeitenImmediate Care of The NewbornMichelle GambolNoch keine Bewertungen
- Pedia Small Notebook Edited PDFDokument17 SeitenPedia Small Notebook Edited PDFAshNoch keine Bewertungen
- 5 Meo DMTDokument18 Seiten5 Meo DMTJimmy Contreras Rey100% (1)
- Chalcone Synthesis, Structure DiversityDokument13 SeitenChalcone Synthesis, Structure DiversityDini Elsi ANoch keine Bewertungen
- Lesson Plan For Anatomy and PhysiologyDokument7 SeitenLesson Plan For Anatomy and PhysiologyJamie Bagundol100% (1)
- What Is Speech TherapyDokument42 SeitenWhat Is Speech Therapyiamoliver_31Noch keine Bewertungen
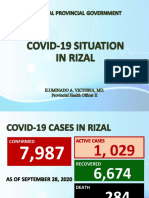
- Covid19 Situation in RizalDokument23 SeitenCovid19 Situation in RizalToni Quitalig GamezNoch keine Bewertungen
- Health Sector EHSMS Requirements-June 2012Dokument31 SeitenHealth Sector EHSMS Requirements-June 2012Aya MahmoudNoch keine Bewertungen
- Manual Neo 900Dokument76 SeitenManual Neo 900Bismarck Pablo Ibañez Piotti67% (3)
- 2015 Case 6 MBUDokument12 Seiten2015 Case 6 MBUDinesh TiwariNoch keine Bewertungen
- Disease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sDokument84 SeitenDisease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sclubstar100% (4)
- Prescription - Apollo 2471688806157843Dokument2 SeitenPrescription - Apollo 2471688806157843shahidliftsNoch keine Bewertungen
- Homeostatic Effect of Laughter On Diabetic Cardiovascular Complications: The Myth Turned To FactDokument9 SeitenHomeostatic Effect of Laughter On Diabetic Cardiovascular Complications: The Myth Turned To FactNona HenNoch keine Bewertungen
- Raku Fire Dragon Way PDFDokument17 SeitenRaku Fire Dragon Way PDFmonipiron100% (4)
- Risk Factors Pathophysiology and Management of HypertensionDokument13 SeitenRisk Factors Pathophysiology and Management of HypertensionDominggas RusunwullyNoch keine Bewertungen
- Counseling Parents About Cochlear ImplantsDokument6 SeitenCounseling Parents About Cochlear ImplantsJordan HansonNoch keine Bewertungen
- 6 Metronidazole Drug StudyDokument4 Seiten6 Metronidazole Drug Studyshadow gonzalezNoch keine Bewertungen
- Pebc Evaluating Exam Sample QuestionDokument50 SeitenPebc Evaluating Exam Sample QuestionZain zanzoonNoch keine Bewertungen
- Sources of Homeopathic DrugsDokument35 SeitenSources of Homeopathic Drugsnadiida83% (6)
- DR Irza Wahid - Annemia Approach - 139Dokument60 SeitenDR Irza Wahid - Annemia Approach - 139single_ladyNoch keine Bewertungen
- DafpusDokument4 SeitenDafpusSyarifah Aini KhairunisaNoch keine Bewertungen