Das könnte Ihnen auch gefallen
- Introduction To Neurosurgical Subspecialties Trauma and Critical Care NeurosurgeryDokument26 SeitenIntroduction To Neurosurgical Subspecialties Trauma and Critical Care NeurosurgeryMuhammad Azhary LazuardyNoch keine Bewertungen
- Pinealoblastoma With Shunt Metastasis: A Case Report: e Ea e yDokument4 SeitenPinealoblastoma With Shunt Metastasis: A Case Report: e Ea e yMuhammad Azhary LazuardyNoch keine Bewertungen
- Emergency Presentation of Neurosurgical ConditionsDokument5 SeitenEmergency Presentation of Neurosurgical ConditionsMuhammad Azhary LazuardyNoch keine Bewertungen
- Kumpulan Soal 1Dokument25 SeitenKumpulan Soal 1Muhammad Azhary LazuardyNoch keine Bewertungen
- Bandung ISPN Course 2019 Final ReportDokument19 SeitenBandung ISPN Course 2019 Final ReportMuhammad Azhary LazuardyNoch keine Bewertungen
- Neurosurgical Patties: Adhesion and Damage MitigationDokument8 SeitenNeurosurgical Patties: Adhesion and Damage MitigationMuhammad Azhary LazuardyNoch keine Bewertungen
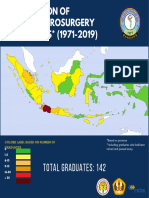
- Total Graduates: 142: Colors Label Based On Number of GraduatesDokument1 SeiteTotal Graduates: 142: Colors Label Based On Number of GraduatesMuhammad Azhary LazuardyNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- CPRDokument9 SeitenCPRHervina MahmudNoch keine Bewertungen
- Surgical AsepsisDokument2 SeitenSurgical AsepsisCheryl PorpayasNoch keine Bewertungen
- Daftar Harga Pengujian Dan Kalibrasi Alat KesehatanDokument3 SeitenDaftar Harga Pengujian Dan Kalibrasi Alat KesehatanVIDYA VIRA PAKSYA PUTRANoch keine Bewertungen
- ColostomyDokument11 SeitenColostomyRiddhi Mehta0% (1)
- Spinal Coding HandoutDokument66 SeitenSpinal Coding HandoutagnaveenanNoch keine Bewertungen
- Kopkash 2018Dokument6 SeitenKopkash 2018Yefry Onil Santana MarteNoch keine Bewertungen
- 4 - Trunk Part 1Dokument32 Seiten4 - Trunk Part 1Jihuhn YuNoch keine Bewertungen
- Description: Congestive Heart FailureDokument22 SeitenDescription: Congestive Heart FailurePinklet Arleena CubianNoch keine Bewertungen
- Introduction To Oral Surgery & ExodontiaDokument14 SeitenIntroduction To Oral Surgery & ExodontiaBashir KhanNoch keine Bewertungen
- Posterior Abdominal WallDokument125 SeitenPosterior Abdominal Wallarjun.k5796Noch keine Bewertungen
- Physiology CVS MCQ (Dr. Nassar)Dokument23 SeitenPhysiology CVS MCQ (Dr. Nassar)زياد سعيدNoch keine Bewertungen
- Normal & Abnormal LabourDokument5 SeitenNormal & Abnormal Labourra100% (1)
- Digestive System KrvaDokument57 SeitenDigestive System KrvaFercilyn MarbanNoch keine Bewertungen
- Canalplasty For ExostosisDokument9 SeitenCanalplasty For ExostosisAlbert GheorgheNoch keine Bewertungen
- SKILL 13-7 Changing and Emptying An Ostomy Appliance Goal: The Stoma Appliance Is Applied Correctly To The Skin To Allow Stool To Drain FreelyDokument3 SeitenSKILL 13-7 Changing and Emptying An Ostomy Appliance Goal: The Stoma Appliance Is Applied Correctly To The Skin To Allow Stool To Drain FreelyHarley Justiniani Dela CruzNoch keine Bewertungen
- ResumeDokument2 SeitenResumeapi-406491631Noch keine Bewertungen
- The Diagnosis and Management of Anorectal Disorders PDFDokument60 SeitenThe Diagnosis and Management of Anorectal Disorders PDFArizal Abdullah100% (1)
- Assessment and Management of Preoperative AnxietyDokument6 SeitenAssessment and Management of Preoperative AnxietyFiorel Loves EveryoneNoch keine Bewertungen
- AnestheticsDokument11 SeitenAnestheticsKalidasan KrishnaNoch keine Bewertungen
- Banana Leaf DressingDokument4 SeitenBanana Leaf Dressingapi-3801331Noch keine Bewertungen
- Nissen Wrap ComplicationsDokument13 SeitenNissen Wrap ComplicationsJalal Abu HalimahNoch keine Bewertungen
- Case Analysis (Physical Assessment)Dokument4 SeitenCase Analysis (Physical Assessment)angelsykeNoch keine Bewertungen
- Subdural InjectionDokument5 SeitenSubdural InjectionMarcoMadueñoMejíaNoch keine Bewertungen
- Paediatric RadiographyDokument102 SeitenPaediatric RadiographyMunish Dogra100% (1)
- O&G CompendiumDokument676 SeitenO&G Compendiumwalefamous100% (1)
- Bovie International Product Catalog 55 275 001 r0Dokument42 SeitenBovie International Product Catalog 55 275 001 r0Heidi BlueNoch keine Bewertungen
- Laporan Mingguan Kamar OperasiDokument14 SeitenLaporan Mingguan Kamar Operasisri puji hartiniNoch keine Bewertungen
- Pig Heart DissectionDokument6 SeitenPig Heart DissectionNathalia Uhna BalboaNoch keine Bewertungen
- Topik 14. Medical Equipment VocabularyDokument8 SeitenTopik 14. Medical Equipment VocabularyYunita HarahapNoch keine Bewertungen
- Cesarean Scar Pregnancies and Their ManagementDokument7 SeitenCesarean Scar Pregnancies and Their ManagementClinton SitanggangNoch keine Bewertungen