Das könnte Ihnen auch gefallen
- Antidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsDokument3 SeitenAntidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsCarina ColtuneacNoch keine Bewertungen
- Antidepressant Therapy Algorithm PDFDokument12 SeitenAntidepressant Therapy Algorithm PDFiwul kiwul KriwulNoch keine Bewertungen
- 1: Adhd: Scientific Name Dose CommentsDokument4 Seiten1: Adhd: Scientific Name Dose CommentsSadiq Abdo92Noch keine Bewertungen
- Psych DrugsDokument3 SeitenPsych DrugsSwarna BanikNoch keine Bewertungen
- Antidepressant ChartDokument7 SeitenAntidepressant Chartinher1tance100% (4)
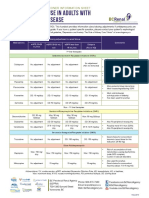
- Antidepressant Use in Adults With Chronic Kidney DiseaseDokument1 SeiteAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDokument6 SeitenAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonNoch keine Bewertungen
- Shortened REM Latency and Increased REM: Previous AttemptDokument19 SeitenShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNoch keine Bewertungen
- Pharmacotherapy in PschiatryDokument8 SeitenPharmacotherapy in PschiatryygfhdgNoch keine Bewertungen
- The RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathDokument2 SeitenThe RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathRahul RaiNoch keine Bewertungen
- Just Getting The Main RX Names Down : Antidepressants Mood StabilizersDokument1 SeiteJust Getting The Main RX Names Down : Antidepressants Mood StabilizersCarlos Eduardo LinaresNoch keine Bewertungen
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDokument8 SeitenCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniNoch keine Bewertungen
- Treatment Modalities For Mood DisordersDokument55 SeitenTreatment Modalities For Mood DisordersGlory MimiNoch keine Bewertungen
- AntipsychoticsDokument10 SeitenAntipsychoticswawing16Noch keine Bewertungen
- Pharmacology - (5) Psychotic DrugsDokument8 SeitenPharmacology - (5) Psychotic DrugsSamantha DiegoNoch keine Bewertungen
- Geriatric Giants - DR SeymourDokument108 SeitenGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Preferentially Block Uptake of 5-HT Preferentially Block Uptake of NADokument3 SeitenPreferentially Block Uptake of 5-HT Preferentially Block Uptake of NAThư Phạm100% (1)
- A Roadmap TO Psychiatric ResidencyDokument21 SeitenA Roadmap TO Psychiatric Residencycatalin_ilie_5Noch keine Bewertungen
- Psychiatry EoY History SampleDokument11 SeitenPsychiatry EoY History SampleNicholasNoch keine Bewertungen
- Neuroleptic Malignant SyndromeDokument11 SeitenNeuroleptic Malignant SyndromeRhomizal MazaliNoch keine Bewertungen
- Current Clinical Strategies: Handbook of Psychiatric DrugsDokument72 SeitenCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116Noch keine Bewertungen
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDokument29 SeitenPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNoch keine Bewertungen
- (PSYCH) 4.01 Forensic Psychiatry - Dr. Cruz PDFDokument6 Seiten(PSYCH) 4.01 Forensic Psychiatry - Dr. Cruz PDFMon Kristoper CastilloNoch keine Bewertungen
- 504 - Pediatric Psychopharmacology - General PrinciplesDokument54 Seiten504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroNoch keine Bewertungen
- Antidepressant DrugsDokument21 SeitenAntidepressant DrugsKashis SharmaNoch keine Bewertungen
- Psych History Format 2017Dokument2 SeitenPsych History Format 2017Anne SisonNoch keine Bewertungen
- Drugs For NeurolepticsDokument1 SeiteDrugs For Neurolepticssyamil_daudNoch keine Bewertungen
- PA 644 - M2 LecturesDokument412 SeitenPA 644 - M2 LectureskatNoch keine Bewertungen
- Template Clerking PsychiatryDokument2 SeitenTemplate Clerking Psychiatrymunii28Noch keine Bewertungen
- Psychotropic Medication ReviewDokument7 SeitenPsychotropic Medication ReviewAakash Shah100% (1)
- Pharmacology (1) - 104-122Dokument19 SeitenPharmacology (1) - 104-122Dental LecturesMMQNoch keine Bewertungen
- Translate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeDokument76 SeitenTranslate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeHadi GunaNoch keine Bewertungen
- Sudden Onset (Within 2 Weeks) of at Least One of TheDokument2 SeitenSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNoch keine Bewertungen
- Psychiatry Capstone 43020 Agitation PsychopharmacologyDokument20 SeitenPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470Noch keine Bewertungen
- Substance Use DisordersDokument28 SeitenSubstance Use DisordersAbdul NazarNoch keine Bewertungen
- Neuro Psych - Antiepileptic Drug ChartDokument5 SeitenNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- Table 1: Substrates of Cytochrome P450 (CYP) EnzymesDokument6 SeitenTable 1: Substrates of Cytochrome P450 (CYP) EnzymesNurul Kamilah SadliNoch keine Bewertungen
- Psychotropics NotesDokument5 SeitenPsychotropics NotesJulianna Rheaven JoreNoch keine Bewertungen
- Antidepressants and Mood StabilizersDokument4 SeitenAntidepressants and Mood Stabilizers우정은Noch keine Bewertungen
- Psych Notes Case FilesDokument5 SeitenPsych Notes Case FilesMitz JuneNoch keine Bewertungen
- Handbook of Psychiatric DrugsDokument68 SeitenHandbook of Psychiatric Drugsbson100% (13)
- UWorld - Psych Review Charts (From Questions)Dokument47 SeitenUWorld - Psych Review Charts (From Questions)uowhywxuuiragjadchNoch keine Bewertungen
- Laboratory Monitoring When Prescribing PsychotropicsDokument5 SeitenLaboratory Monitoring When Prescribing PsychotropicswaleskacrzNoch keine Bewertungen
- Neuroleptics & AnxiolyticsDokument65 SeitenNeuroleptics & AnxiolyticsAntonPurpurovNoch keine Bewertungen
- Adhd Toolkit MedicationsDokument1 SeiteAdhd Toolkit MedicationsreneezNoch keine Bewertungen
- Immediate Release - (Methylphenidate)Dokument4 SeitenImmediate Release - (Methylphenidate)MaryNguyenNoch keine Bewertungen
- CHT Psyc AntidepressantDokument3 SeitenCHT Psyc AntidepressantRicardo Lugon ArantesNoch keine Bewertungen
- Benzodiazepine Equivalents DassaDokument2 SeitenBenzodiazepine Equivalents DassaPsikiater PanturaNoch keine Bewertungen
- Glossary of Psychiatric TermsDokument42 SeitenGlossary of Psychiatric TermsÏtz ShãrîNoch keine Bewertungen
- Psychopharmacology in PsychiatryDokument94 SeitenPsychopharmacology in PsychiatryOslo SaputraNoch keine Bewertungen
- Drug List Psych Optho NeuroDokument22 SeitenDrug List Psych Optho NeuroAshley BarrileNoch keine Bewertungen
- TCPR Jan 07 AntidepDokument8 SeitenTCPR Jan 07 AntidepdcarlatNoch keine Bewertungen
- Why Psychiatry? Some Thoughts For Medical Students.Dokument3 SeitenWhy Psychiatry? Some Thoughts For Medical Students.Davin TanNoch keine Bewertungen
- Mental HealthDokument178 SeitenMental HealthGarry GuiteNoch keine Bewertungen
- Anxiety/Depression: S AlprazolamDokument2 SeitenAnxiety/Depression: S AlprazolamleesaNoch keine Bewertungen
- Warnick-Prescribing Meds For Anxiety and Depression PlenaryDokument33 SeitenWarnick-Prescribing Meds For Anxiety and Depression PlenaryAKNTAI002Noch keine Bewertungen
- Handy Summary Chart Comparing The Main Medications For PsychosisDokument3 SeitenHandy Summary Chart Comparing The Main Medications For Psychosisrowanpurdy100% (2)
- Lamotrigine in Psychiatric DisordersDokument10 SeitenLamotrigine in Psychiatric DisordersastrogliaNoch keine Bewertungen
- Antipsychotics Guidelines PDFDokument31 SeitenAntipsychotics Guidelines PDFZulvikar Umasangadji100% (1)
- Introduction of Woman Role in SocietyDokument12 SeitenIntroduction of Woman Role in SocietyApple DogNoch keine Bewertungen
- The Big M Method: Group BDokument7 SeitenThe Big M Method: Group BWoo Jin YoungNoch keine Bewertungen
- Cover PageDokument10 SeitenCover PageAvijit GhoshNoch keine Bewertungen
- (Official) AVTC5 - Unit 1 - Before ClassDokument11 Seiten(Official) AVTC5 - Unit 1 - Before ClassNhân NguyễnNoch keine Bewertungen
- Branch & Category Wise Opening & Closing Rank of JEE (Main) 2019Dokument46 SeitenBranch & Category Wise Opening & Closing Rank of JEE (Main) 2019soni dwivediNoch keine Bewertungen
- FRQ Vocabulary ReviewDokument1 SeiteFRQ Vocabulary ReviewDrew AbbottNoch keine Bewertungen
- D4462045416 PDFDokument3 SeitenD4462045416 PDFSamir MazafranNoch keine Bewertungen
- Learning Activity No.2Dokument1 SeiteLearning Activity No.2Miki AntonNoch keine Bewertungen
- High School Department PAASCU Accredited Academic Year 2017 - 2018Dokument6 SeitenHigh School Department PAASCU Accredited Academic Year 2017 - 2018Kevin T. OnaroNoch keine Bewertungen
- Marisa Wolf Final New ResumeDokument2 SeitenMarisa Wolf Final New Resumeapi-403499166Noch keine Bewertungen
- Project in Precal: Mary Joyce MolinesDokument11 SeitenProject in Precal: Mary Joyce MolinesJaja KeykNoch keine Bewertungen
- Christine Remembered That Today Is The Birthday of Her BossDokument1 SeiteChristine Remembered That Today Is The Birthday of Her BossA.Noch keine Bewertungen
- 02-Fundamentals of Engineering EconomyDokument14 Seiten02-Fundamentals of Engineering EconomyLin Xian XingNoch keine Bewertungen
- Учебный предметDokument2 SeitenУчебный предметorang shabdizNoch keine Bewertungen
- REM630 Broch 756825 LRENdDokument6 SeitenREM630 Broch 756825 LRENdsihamuNoch keine Bewertungen
- TRUMPF Marking Laser BrochureDokument48 SeitenTRUMPF Marking Laser BrochureKKM SBNoch keine Bewertungen
- Charging Station For E-Vehicle Using Solar With IOTDokument6 SeitenCharging Station For E-Vehicle Using Solar With IOTjakeNoch keine Bewertungen
- AMC Middle Primary Years 3 and 4 - SolutionsDokument6 SeitenAMC Middle Primary Years 3 and 4 - SolutionsSherry JiangNoch keine Bewertungen
- GCGM PDFDokument11 SeitenGCGM PDFMiguel Angel Martin100% (1)
- 04 DosimetryDokument104 Seiten04 DosimetryEdmond ChiangNoch keine Bewertungen
- IAU Logbook Core 6weeksDokument7 SeitenIAU Logbook Core 6weeksbajariaaNoch keine Bewertungen
- Pamphlet On Arrangement of Springs in Various Casnub Trolleys Fitted On Air Brake Wagon PDFDokument9 SeitenPamphlet On Arrangement of Springs in Various Casnub Trolleys Fitted On Air Brake Wagon PDFNiKhil GuPtaNoch keine Bewertungen
- Different Art TechniquesDokument39 SeitenDifferent Art TechniquesRommel LegaspiNoch keine Bewertungen
- Test Bank For Body Structures and Functions 11th Edition Ann ScottDokument27 SeitenTest Bank For Body Structures and Functions 11th Edition Ann Scottpellucidutter.uka6lr100% (38)
- State of The Art in Research On MicrogridsDokument36 SeitenState of The Art in Research On MicrogridsDulal MannaNoch keine Bewertungen
- Practical Research 2Dokument16 SeitenPractical Research 2Benedict Coloma BandongNoch keine Bewertungen
- UVEX - Helmets & Eyewear 2009Dokument19 SeitenUVEX - Helmets & Eyewear 2009Ivica1977Noch keine Bewertungen
- Web Programming: GET / HTTP/1.1 ..Dokument16 SeitenWeb Programming: GET / HTTP/1.1 ..Alecu IlieNoch keine Bewertungen
- CrumpleZonesSE (Edit)Dokument12 SeitenCrumpleZonesSE (Edit)Dah Unknown MarksmenNoch keine Bewertungen
- Potassium Permanganate CARUSOL CarusCoDokument9 SeitenPotassium Permanganate CARUSOL CarusColiebofreakNoch keine Bewertungen