Das könnte Ihnen auch gefallen
- Morrell Notes (Updated)Dokument129 SeitenMorrell Notes (Updated)darrentse100% (1)
- 10.21307 - Immunohematology 2022 048 PDFDokument6 Seiten10.21307 - Immunohematology 2022 048 PDFTanupreetNoch keine Bewertungen
- Package Insert - Cobas MPX Test, For Use On The Cobas 6800-8800 SystemsDokument50 SeitenPackage Insert - Cobas MPX Test, For Use On The Cobas 6800-8800 Systemsسعد الطائعNoch keine Bewertungen
- Pathology Outlines - Papillary Carcinoma - GeneralDokument6 SeitenPathology Outlines - Papillary Carcinoma - Generalpatka1rNoch keine Bewertungen
- Practical Hemostasis and ThrombosisVon EverandPractical Hemostasis and ThrombosisNigel S. KeyNoch keine Bewertungen
- Fast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsVon EverandFast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsNoch keine Bewertungen
- PS40 BloodMarrow Booklet 2023Dokument72 SeitenPS40 BloodMarrow Booklet 2023wilkesgillinghamNoch keine Bewertungen
- Blood Transfusion Procedures: January 2011 Review Date: January 2013Dokument55 SeitenBlood Transfusion Procedures: January 2011 Review Date: January 2013goldaNoch keine Bewertungen
- AABB Pediatric Transfusion - Risks and GuidelinesDokument57 SeitenAABB Pediatric Transfusion - Risks and GuidelinesDR.RAJESWARI SUBRAMANIYANNoch keine Bewertungen
- Blood Basics1Dokument6 SeitenBlood Basics1Celina PastorNoch keine Bewertungen
- Blood Safety CPG and Policy Final 10282009 PDFDokument70 SeitenBlood Safety CPG and Policy Final 10282009 PDFdebbie o. azcunaNoch keine Bewertungen
- Aabb PBM WhitepaperDokument18 SeitenAabb PBM WhitepaperdamadolNoch keine Bewertungen
- Bloody Easy 4Dokument82 SeitenBloody Easy 4dubblewalker100% (1)
- Platelet Storage Pool Disorders PDFDokument4 SeitenPlatelet Storage Pool Disorders PDFMano CempakaNoch keine Bewertungen
- Immuno HematologyDokument24 SeitenImmuno HematologyHoraa H AL-marhoonNoch keine Bewertungen
- How I Use Platelet TransfusionsDokument12 SeitenHow I Use Platelet TransfusionsJovanna OrtuñoNoch keine Bewertungen
- Haematologists Toolkit V1b August 16 EoEDokument23 SeitenHaematologists Toolkit V1b August 16 EoELlrss AdnNoch keine Bewertungen
- FFP and Cryoprecipitate FinalDokument6 SeitenFFP and Cryoprecipitate FinalganotNoch keine Bewertungen
- Medication Deferral ListDokument2 SeitenMedication Deferral ListKwiila KaoNoch keine Bewertungen
- Review of Current Transfusion Therapy and Blood Banking PracticesDokument52 SeitenReview of Current Transfusion Therapy and Blood Banking PracticesAmaranto SantosoNoch keine Bewertungen
- Platelet IndicesDokument17 SeitenPlatelet IndicesNarendra Bhattarai0% (1)
- Transfusion Training Checklist May 2015Dokument5 SeitenTransfusion Training Checklist May 2015dheNoch keine Bewertungen
- Guideline Cardiac of WHODokument92 SeitenGuideline Cardiac of WHOFatimah AzzuhraNoch keine Bewertungen
- Normal ValuesDokument18 SeitenNormal ValuesCharmae NaveaNoch keine Bewertungen
- CMQCC - Transfusion in Obstetric HemorrhageDokument10 SeitenCMQCC - Transfusion in Obstetric HemorrhageBerri RahmadhoniNoch keine Bewertungen
- Clinical Manifestations and Diagnosis of The Thalassemias - UpToDateDokument52 SeitenClinical Manifestations and Diagnosis of The Thalassemias - UpToDatesushi37Noch keine Bewertungen
- Red Cell Antibody PanelsDokument40 SeitenRed Cell Antibody Panelsrube10000Noch keine Bewertungen
- PlateletsDokument35 SeitenPlateletsSiĦãm Mỡ100% (1)
- Predanalitika KoagulacijaDokument10 SeitenPredanalitika KoagulacijaAnonymous w4qodCJNoch keine Bewertungen
- The Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CanDokument9 SeitenThe Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CananggaririnNoch keine Bewertungen
- Transfusion: Practices in NicuDokument80 SeitenTransfusion: Practices in NicuPranay MallNoch keine Bewertungen
- 5.Rh Blood Group SystemDokument22 Seiten5.Rh Blood Group Systemjong188Noch keine Bewertungen
- 2022 Book TheEBMTEHACAR-TCellHandbookDokument221 Seiten2022 Book TheEBMTEHACAR-TCellHandbookInchirah Narimane MgdNoch keine Bewertungen
- Management of HyperleukocytosisDokument10 SeitenManagement of HyperleukocytosisNaty AlvarezNoch keine Bewertungen
- FDA Blood Bank & Blood TranfusionDokument44 SeitenFDA Blood Bank & Blood TranfusionDrSyedRashidAliNoch keine Bewertungen
- Approved Nigerian National Blood PolicyDokument24 SeitenApproved Nigerian National Blood PolicyUkaegbu Chibueze JnrNoch keine Bewertungen
- Slide Presentation - Introduction To Immunohematology PDFDokument71 SeitenSlide Presentation - Introduction To Immunohematology PDFRose jane TambasenNoch keine Bewertungen
- XN Series: Case InterpretationDokument41 SeitenXN Series: Case InterpretationTanveerNoch keine Bewertungen
- Clinical Guide To Transfusion - Neonatal and Pediatric Transfusion (Chapter 13)Dokument11 SeitenClinical Guide To Transfusion - Neonatal and Pediatric Transfusion (Chapter 13)Mudzakir TaufiqNoch keine Bewertungen
- Clinical Practice GuidelinesDokument99 SeitenClinical Practice GuidelinesKersti Marzo100% (1)
- Hemabook Chapter 1 18Dokument69 SeitenHemabook Chapter 1 18Dam LNoch keine Bewertungen
- Bloody Easy - Coagulation ExplainedDokument25 SeitenBloody Easy - Coagulation ExplainedDaniela GreereNoch keine Bewertungen
- Blood Component TherapyDokument73 SeitenBlood Component TherapySaikat Prasad DattaNoch keine Bewertungen
- A Methodical Approach To Interpreting The Platelet Parameters of The Complete Blood CountDokument11 SeitenA Methodical Approach To Interpreting The Platelet Parameters of The Complete Blood CountAlex YohanaNoch keine Bewertungen
- Interpretasi Darah RutinDokument22 SeitenInterpretasi Darah Rutinboy jendri huluNoch keine Bewertungen
- Blood Transfusion Services in Sub Saharan Africa: Challenges and ConstraintsVon EverandBlood Transfusion Services in Sub Saharan Africa: Challenges and ConstraintsNoch keine Bewertungen
- Einstein - Resident Manual 2016-2017 10.19.16 PDFDokument69 SeitenEinstein - Resident Manual 2016-2017 10.19.16 PDFcoolradish100% (1)
- Apheresis PrincipleDokument68 SeitenApheresis Principlemelisa asibalNoch keine Bewertungen
- Blood Transfusion On Dialysis Guidelines Aug 2017 PDFDokument5 SeitenBlood Transfusion On Dialysis Guidelines Aug 2017 PDFYolanda IrawatiNoch keine Bewertungen
- Report of Adverse Transfusion Reaction To Blood SuppliersDokument8 SeitenReport of Adverse Transfusion Reaction To Blood SuppliersDominic EmerencianaNoch keine Bewertungen
- Blood and Marrow Transplant Quality Management PlanDokument47 SeitenBlood and Marrow Transplant Quality Management PlansumathiNoch keine Bewertungen
- Basic HaematologyDokument32 SeitenBasic HaematologyAhtshamtaeiq AhtshamtariqNoch keine Bewertungen
- Neonatal HematologyDokument83 SeitenNeonatal HematologyJay-Anne RapanoNoch keine Bewertungen
- C B C I: Omplete Lood Ount NterpretationsDokument44 SeitenC B C I: Omplete Lood Ount NterpretationsridhoniNoch keine Bewertungen
- Transfusion Medicine - 2017 - Robinson - The Administration of Blood Components A British Society For HaematologyDokument19 SeitenTransfusion Medicine - 2017 - Robinson - The Administration of Blood Components A British Society For HaematologyRand AliNoch keine Bewertungen
- Blood Administration: NRS 108 Essec County CollegeDokument22 SeitenBlood Administration: NRS 108 Essec County CollegeDiah Puspita RiniNoch keine Bewertungen
- 3-c TEa Tabel ExtinsDokument36 Seiten3-c TEa Tabel ExtinsJimboreanu György PaulaNoch keine Bewertungen
- (IMMUNOHEMA) Denise M. Harmening - Modern Blood Banking & Transfusion Practices (2019, F.A. Davis)Dokument56 Seiten(IMMUNOHEMA) Denise M. Harmening - Modern Blood Banking & Transfusion Practices (2019, F.A. Davis)Who KnowsNoch keine Bewertungen
- Crossmatching and Issuing Blood Components PDFDokument20 SeitenCrossmatching and Issuing Blood Components PDFdianaNoch keine Bewertungen
- Immuno HematologyDokument35 SeitenImmuno HematologyAlan McLeanNoch keine Bewertungen
- 5th Handbook of Transfusion MedicineDokument186 Seiten5th Handbook of Transfusion MedicineDokter Dhea Danni Agisty100% (1)
- HLC 723GXDokument25 SeitenHLC 723GXسعد الطائعNoch keine Bewertungen
- Sysmex KX 21 Histogram Interpretation HandbookDokument28 SeitenSysmex KX 21 Histogram Interpretation Handbookسعد الطائع100% (4)
- SUIT Protocol Description v10.0Dokument62 SeitenSUIT Protocol Description v10.0سعد الطائعNoch keine Bewertungen
- Advia CP Lis DoclibdDokument132 SeitenAdvia CP Lis Doclibdسعد الطائعNoch keine Bewertungen
- Neutralization, Hemolysis and Complement Fixation: Group 9 Megino, Elvin Maturgo, Kenneth Reyes, Patricia Vergara, CyrilDokument42 SeitenNeutralization, Hemolysis and Complement Fixation: Group 9 Megino, Elvin Maturgo, Kenneth Reyes, Patricia Vergara, CyrilPatty ReyesNoch keine Bewertungen
- Male Reproductive SystemDokument121 SeitenMale Reproductive SystemProf Lina RamliNoch keine Bewertungen
- SS1 2ND Term Animal Husbandry E-NoteDokument23 SeitenSS1 2ND Term Animal Husbandry E-Notekanajoseph2009Noch keine Bewertungen
- Pelvic Organ ProlapseDokument23 SeitenPelvic Organ ProlapseAbdullah Matar100% (2)
- Graded Quiz Unit 6 Attempt ReviewDokument6 SeitenGraded Quiz Unit 6 Attempt ReviewSafwan al ubaiedNoch keine Bewertungen
- Latin 2Dokument29 SeitenLatin 2ShreyaNoch keine Bewertungen
- Carrier-Mediated Dermal DeliveryDokument587 SeitenCarrier-Mediated Dermal DeliveryVanderval SIlva de OliveiraNoch keine Bewertungen
- Human Heart ScienceDokument7 SeitenHuman Heart ScienceJewel Kathryn MorenoNoch keine Bewertungen
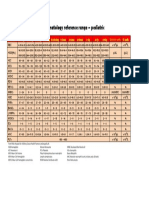
- Hematology Reference RangeDokument1 SeiteHematology Reference RangeNheeya WarzNoch keine Bewertungen
- Bone Marrow and Stem Cell TranspplantDokument28 SeitenBone Marrow and Stem Cell TranspplantVILLEJO JHOVIALENNoch keine Bewertungen
- AUBF - Amniotic Fluid and Semen Study MaterialDokument10 SeitenAUBF - Amniotic Fluid and Semen Study MaterialVienna Jamaica Be Cari-CariNoch keine Bewertungen
- Liver Function TestsDokument28 SeitenLiver Function TestsDr. Ashish Jawarkar100% (3)
- The Theater of Anatomy - The Anatomical Preparations of Honore Fragonard PDFDokument18 SeitenThe Theater of Anatomy - The Anatomical Preparations of Honore Fragonard PDFFrancisco SantosNoch keine Bewertungen
- Study of Plant Cells in Hypertonic Solution: Experiment: PlasmolysisDokument2 SeitenStudy of Plant Cells in Hypertonic Solution: Experiment: PlasmolysisJyoti DahiyaNoch keine Bewertungen
- Hematology PPT 1Dokument287 SeitenHematology PPT 1TarishiMalikNoch keine Bewertungen
- Anatomy of Hepatobiliary SystemDokument46 SeitenAnatomy of Hepatobiliary SystemAyu Tiara FitriNoch keine Bewertungen
- Biology Qns v2Dokument37 SeitenBiology Qns v2randomvidsNoch keine Bewertungen
- Module 27Dokument14 SeitenModule 27Jerico CastilloNoch keine Bewertungen
- Pancreas: Cynthia D. Guy, MD Associate Professor of Pathology DumcDokument56 SeitenPancreas: Cynthia D. Guy, MD Associate Professor of Pathology Dumcionut1ilie-1Noch keine Bewertungen
- Blood ComponentDokument4 SeitenBlood ComponentVictor GonzalesNoch keine Bewertungen
- Functional Matrix HypothesisDokument14 SeitenFunctional Matrix Hypothesispriyab710Noch keine Bewertungen
- Antibody EngineeringDokument14 SeitenAntibody EngineeringJholina Aure ReyesNoch keine Bewertungen
- 21 Plant Structure and FunctionDokument50 Seiten21 Plant Structure and FunctionRoan James OcampoNoch keine Bewertungen
- Lesson 9: Endocrine System: Prepared by Arianne V. JulianDokument34 SeitenLesson 9: Endocrine System: Prepared by Arianne V. JulianGisselleNoch keine Bewertungen
- L5 - BB LecDokument7 SeitenL5 - BB LecJUDEA WILCH ORJENoch keine Bewertungen
- Cells To Tissues To Organs Graphic Organizer ExampleDokument2 SeitenCells To Tissues To Organs Graphic Organizer Exampleapi-431603797Noch keine Bewertungen
- 3rd Week of Development EmbryologyDokument90 Seiten3rd Week of Development EmbryologySomeoneNoch keine Bewertungen
- Lecture 2 Life Science EmbryologyDokument20 SeitenLecture 2 Life Science EmbryologyjoeNoch keine Bewertungen