Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Clinical FormulationDokument24 SeitenClinical Formulationaimee2oo8100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- ThrombophlebitisDokument3 SeitenThrombophlebitismirrejNoch keine Bewertungen
- RAD: Reactive Attachment Disorder ResourcesDokument8 SeitenRAD: Reactive Attachment Disorder ResourcesveronicaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- NHIC PT & OT Billing and CodingDokument83 SeitenNHIC PT & OT Billing and Codingsbtappouni0% (1)
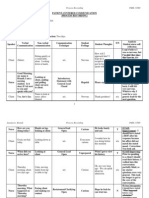
- 360 Process Recording TemplateDokument13 Seiten360 Process Recording Templateapi-252910411100% (9)
- CT Scanning - Techniques and Applications PDFDokument358 SeitenCT Scanning - Techniques and Applications PDFMinionNoch keine Bewertungen
- Enteric-Coated Serratiopeptidase Product InfoDokument2 SeitenEnteric-Coated Serratiopeptidase Product Infoamin138ir0% (2)
- 1 Social Administrative and Management Sciences Q&A Content Ver1Dokument34 Seiten1 Social Administrative and Management Sciences Q&A Content Ver1bhaveshnidhi64100% (1)
- @anesthesia Books 2010 Get Through PDFDokument334 Seiten@anesthesia Books 2010 Get Through PDFMinaz Patel100% (1)
- Genetics Practice NCLEX Questions HandoutDokument6 SeitenGenetics Practice NCLEX Questions HandoutAlvin L. Rozier100% (3)
- A Case Study On Renal CancerDokument30 SeitenA Case Study On Renal CancerAiyish CapunoNoch keine Bewertungen
- Fellowship of Neurocritical Care (FNCC) : Need For The CourseDokument12 SeitenFellowship of Neurocritical Care (FNCC) : Need For The CourseMinaz PatelNoch keine Bewertungen
- Advance Airway Webinar Programme 10AM-4PM ISTDokument1 SeiteAdvance Airway Webinar Programme 10AM-4PM ISTMinaz PatelNoch keine Bewertungen
- Declaration NimhansDokument1 SeiteDeclaration NimhansSoumya BhattacharyaNoch keine Bewertungen
- 11th Master Class on Future of Pain & Palliative MedicineDokument1 Seite11th Master Class on Future of Pain & Palliative MedicineMinaz PatelNoch keine Bewertungen
- Bhalani Ereader Android UG PDFDokument25 SeitenBhalani Ereader Android UG PDFSuyash NawaleNoch keine Bewertungen
- Paed Osce 2 PDFDokument80 SeitenPaed Osce 2 PDFMinaz PatelNoch keine Bewertungen
- Clinical Case ManagementDokument50 SeitenClinical Case ManagementAvinash KumarNoch keine Bewertungen
- Covid 19 - Exam All QuestionsDokument30 SeitenCovid 19 - Exam All QuestionsBeta ReaderNoch keine Bewertungen
- Guidelines on Dead Body ManagementDokument7 SeitenGuidelines on Dead Body ManagementSandeep BansalNoch keine Bewertungen
- PDF Upload-141116Dokument3 SeitenPDF Upload-141116Minaz PatelNoch keine Bewertungen
- QP Code:103101 Reg. No.: PG Degree Supplementary Examinations in Anaesthesiology (MD) October 2019lDokument1 SeiteQP Code:103101 Reg. No.: PG Degree Supplementary Examinations in Anaesthesiology (MD) October 2019lMinaz PatelNoch keine Bewertungen
- Circulation: Consensus ReportsDokument11 SeitenCirculation: Consensus ReportsKarla HernandezNoch keine Bewertungen
- IndianJAnaesth Adult 2017Dokument14 SeitenIndianJAnaesth Adult 2017Minaz PatelNoch keine Bewertungen
- 311 1376 1 PB PDFDokument3 Seiten311 1376 1 PB PDFMinaz PatelNoch keine Bewertungen
- Emergency Checklists PDFDokument28 SeitenEmergency Checklists PDFAnca Florentina NiculaeNoch keine Bewertungen
- @anesthesia - Books 2016 Controlled Drug Delivery SystemsDokument107 Seiten@anesthesia - Books 2016 Controlled Drug Delivery SystemsMinaz PatelNoch keine Bewertungen
- 1324autonomicdysfunc 180617164555Dokument83 Seiten1324autonomicdysfunc 180617164555Minaz PatelNoch keine Bewertungen
- Burns and ICU 2012Dokument5 SeitenBurns and ICU 2012Minaz PatelNoch keine Bewertungen
- 159 Anaesthesia For Children With Obstructive Sleep ApnoeaDokument6 Seiten159 Anaesthesia For Children With Obstructive Sleep ApnoeaMinaz PatelNoch keine Bewertungen
- Parkinsonism PDFDokument3 SeitenParkinsonism PDFNerissaArvianaShintaraNoch keine Bewertungen
- Understanding Takayasu's ArteritisDokument56 SeitenUnderstanding Takayasu's ArteritisMinaz PatelNoch keine Bewertungen
- ASA Physical Status Classification System 2019 PDFDokument2 SeitenASA Physical Status Classification System 2019 PDFMinaz PatelNoch keine Bewertungen
- 7 Paediatric Anatomy Physiology and The Basics of Paediatric AnaesthesiaDokument12 Seiten7 Paediatric Anatomy Physiology and The Basics of Paediatric AnaesthesiakochikaghochiNoch keine Bewertungen
- Solid Renal Mass: Hisham Alkhatib, M.DDokument49 SeitenSolid Renal Mass: Hisham Alkhatib, M.DMinaz PatelNoch keine Bewertungen
- Tracts of Spinal Cord: Dr. Fathima TasneemDokument31 SeitenTracts of Spinal Cord: Dr. Fathima TasneemMinaz PatelNoch keine Bewertungen
- Trauma Approach and ManagementDokument64 SeitenTrauma Approach and ManagementpkmkejuruanmudaNoch keine Bewertungen
- JIPMER2000 Question PapersDokument84 SeitenJIPMER2000 Question PapersAbinaya ThiyagarajanNoch keine Bewertungen
- The Grey Matter: Something in The AirDokument28 SeitenThe Grey Matter: Something in The AirMinaz PatelNoch keine Bewertungen
- OncologyDokument94 SeitenOncologyMinaz Patel50% (2)
- SKN PDFDokument233 SeitenSKN PDFclinic waNoch keine Bewertungen
- Aphasia HandoutDokument24 SeitenAphasia HandoutArielena DuranNoch keine Bewertungen
- Oshin Taylor Social Studies SBADokument29 SeitenOshin Taylor Social Studies SBAJaden100% (1)
- The Squiggle-Drawing Game in Child PsychotherapyDokument12 SeitenThe Squiggle-Drawing Game in Child PsychotherapyCaramel GazelleNoch keine Bewertungen
- How Music Aids in Self ExpressionDokument4 SeitenHow Music Aids in Self ExpressionMARSELL SHARMANoch keine Bewertungen
- Freud - Fetishism (1927e)Dokument6 SeitenFreud - Fetishism (1927e)I Smith100% (1)
- Heart Disease Course PDALongDokument84 SeitenHeart Disease Course PDALongArpanpatelNoch keine Bewertungen
- Drugs ReviewedDokument7 SeitenDrugs ReviewedJamil LorcaNoch keine Bewertungen
- Roxonin LeafletDokument2 SeitenRoxonin LeafletmohammedfirasatNoch keine Bewertungen
- Screenshot 2022-12-14 at 4.16.40 PMDokument1 SeiteScreenshot 2022-12-14 at 4.16.40 PMPrisha SoniNoch keine Bewertungen
- Takayasu ArteritisDokument53 SeitenTakayasu ArteritisSuruchi Jagdish Sharma50% (2)
- Thomas J. Butler PH.D RRT RPFT - Laboratory Exercises For Competency in Respiratory Care-F.a. Davis Company (201Dokument865 SeitenThomas J. Butler PH.D RRT RPFT - Laboratory Exercises For Competency in Respiratory Care-F.a. Davis Company (201Celia Seneh GwandiNoch keine Bewertungen
- Five Theories of Human ExistenceDokument6 SeitenFive Theories of Human ExistenceQuenine BridgeNoch keine Bewertungen
- Clasic MindfullneseDokument15 SeitenClasic Mindfullneseayu yuliantiNoch keine Bewertungen
- Orthopaedic Connection: Hip DislocationDokument2 SeitenOrthopaedic Connection: Hip DislocationTeuku FennyNoch keine Bewertungen
- Safe and Sound Protocol Therapeutic TeachingDokument2 SeitenSafe and Sound Protocol Therapeutic TeachingristeacristiNoch keine Bewertungen
- What Is Mindfulness?Dokument2 SeitenWhat Is Mindfulness?Vaseem SyedNoch keine Bewertungen
- Drugs & Therapy: B U L L E T I NDokument4 SeitenDrugs & Therapy: B U L L E T I NWilliam WongNoch keine Bewertungen
- 7.2 IV InjectionDokument4 Seiten7.2 IV InjectionManisa ParidaNoch keine Bewertungen
- Blood TransfusionDokument7 SeitenBlood TransfusionRebecca JolieNoch keine Bewertungen