Das könnte Ihnen auch gefallen
- Conjugated Hyperbilirubinemia in The Neonatal Intensive Care UnitDokument9 SeitenConjugated Hyperbilirubinemia in The Neonatal Intensive Care UnitIvan HoNoch keine Bewertungen
- HyperbilirubinemiaDokument4 SeitenHyperbilirubinemiaJuan Carlos Andrade SalumNoch keine Bewertungen
- The Profile of Bilirubin Level in Healthy Newborn Babies With Jaundice in DR Sardjito Hospital YogyakartaDokument5 SeitenThe Profile of Bilirubin Level in Healthy Newborn Babies With Jaundice in DR Sardjito Hospital YogyakartaErfinaNoch keine Bewertungen
- Gueorguiev 2009Dokument10 SeitenGueorguiev 2009Caroline Ruffo FogassaNoch keine Bewertungen
- Knowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhanaDokument10 SeitenKnowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhananicloverNoch keine Bewertungen
- s.ALP & NNJDokument4 Seitens.ALP & NNJMohammed FareedNoch keine Bewertungen
- A Pilot Study of Expanded Newborn Screening For 573 Genes Related To Severe Inherited Disorders in China: Results From 1,127 NewbornsDokument10 SeitenA Pilot Study of Expanded Newborn Screening For 573 Genes Related To Severe Inherited Disorders in China: Results From 1,127 Newbornssunilpkumar18Noch keine Bewertungen
- Ajpendo 00007 2019Dokument13 SeitenAjpendo 00007 2019Ali MazidiNoch keine Bewertungen
- Hepatic Dysfunction in Paediatric Typhoidal Salmonellosis: Annals of Tropical PaediatricsDokument4 SeitenHepatic Dysfunction in Paediatric Typhoidal Salmonellosis: Annals of Tropical PaediatricsShaznay Dela CruzNoch keine Bewertungen
- Bilirubin Normogram TranscutaneousDokument7 SeitenBilirubin Normogram Transcutaneousapi-236540608Noch keine Bewertungen
- Hyperuricemia Is Associated With Hypertension, Obesity, and Albuminuria in Children With Chronic Kidney DiseaseDokument5 SeitenHyperuricemia Is Associated With Hypertension, Obesity, and Albuminuria in Children With Chronic Kidney DiseaseMuh Husni RifaiNoch keine Bewertungen
- Window of Implantation: Natural Vs Stimulated CyclesDokument30 SeitenWindow of Implantation: Natural Vs Stimulated CyclesagusnestaalbugisyNoch keine Bewertungen
- Do Triple Test Results Predict Risk For Neonatal Hyperbilirubinemia?Dokument5 SeitenDo Triple Test Results Predict Risk For Neonatal Hyperbilirubinemia?ariani khikmatul mazidahNoch keine Bewertungen
- Gestational Diabetes Mellitus in Teenage Pregnancy: A Case-Control StudyDokument3 SeitenGestational Diabetes Mellitus in Teenage Pregnancy: A Case-Control StudySarly FebrianaNoch keine Bewertungen
- Status of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaDokument4 SeitenStatus of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaAgus WijataNoch keine Bewertungen
- 37 FullDokument5 Seiten37 FullPriscilla GeraldineNoch keine Bewertungen
- Tissue-Specific Selection of Stable Reference Genes For Real-Time PCR Normalization in An Obese Rat ModelDokument10 SeitenTissue-Specific Selection of Stable Reference Genes For Real-Time PCR Normalization in An Obese Rat ModelMohammed AlshinqityNoch keine Bewertungen
- Preimplantation Genetic Diagnosis For Aneuploidy Screening in Patients With Unexplained Recurrent MiscarriagesDokument5 SeitenPreimplantation Genetic Diagnosis For Aneuploidy Screening in Patients With Unexplained Recurrent MiscarriagesAkmilia VeraNoch keine Bewertungen
- Effect of Zinc Sulfate on Neonatal JaundiceDokument5 SeitenEffect of Zinc Sulfate on Neonatal JaundiceAbdurrohman IzzuddinNoch keine Bewertungen
- Breast Milk Jaundice BhutaniDokument56 SeitenBreast Milk Jaundice BhutaniViolaNoch keine Bewertungen
- Plasma Levels and Placental Expression of Vaspin in Pregnant Women With Diabetes MellitusDokument7 SeitenPlasma Levels and Placental Expression of Vaspin in Pregnant Women With Diabetes MellitusBala ChandiranNoch keine Bewertungen
- Risk Factors For Hypoxic Ischemic Encephalopathy in ChildrenDokument5 SeitenRisk Factors For Hypoxic Ischemic Encephalopathy in ChildrenSaqib AtherNoch keine Bewertungen
- Pregnancy HypertensionDokument7 SeitenPregnancy HypertensionEgi NabilaNoch keine Bewertungen
- PIIS0015028222000644Dokument7 SeitenPIIS0015028222000644gayathri maranNoch keine Bewertungen
- LKI Perina HDI - 21102021Dokument37 SeitenLKI Perina HDI - 21102021ManusiaNoch keine Bewertungen
- Characteristics and Causes of Diarrhea in Indonesian ChildrenDokument8 SeitenCharacteristics and Causes of Diarrhea in Indonesian ChildrenDrnNoch keine Bewertungen
- Analytical ExpositionDokument9 SeitenAnalytical ExpositionAnnisa FujiantiNoch keine Bewertungen
- Hyperglycemia and Morbidity and Mortality in Extremely Low Birth Weight InfantsDokument7 SeitenHyperglycemia and Morbidity and Mortality in Extremely Low Birth Weight InfantsIvan VeriswanNoch keine Bewertungen
- CRP Pregnancy Cohen 2014Dokument4 SeitenCRP Pregnancy Cohen 2014samiNoch keine Bewertungen
- Jurnal 2 AnakDokument5 SeitenJurnal 2 AnakHafich ErnandaNoch keine Bewertungen
- The Effect of Probiotics in Prevention of Necrotising Enterocolitis in Preterm Neonates in Comparison With Control GroupDokument4 SeitenThe Effect of Probiotics in Prevention of Necrotising Enterocolitis in Preterm Neonates in Comparison With Control GroupchachaNoch keine Bewertungen
- Neonatal Hyperbilirubinemia and Elevated Liver Enzymes Associated With Thyroid Hormone Deficiency in NeonatesDokument4 SeitenNeonatal Hyperbilirubinemia and Elevated Liver Enzymes Associated With Thyroid Hormone Deficiency in NeonatesOlfiany Laurenzia PongohNoch keine Bewertungen
- Effects of Testosterone On Rat Placental DevelopmentDokument8 SeitenEffects of Testosterone On Rat Placental Development1757180967Noch keine Bewertungen
- Indications For Human Albumin Infusion in A NeonatDokument5 SeitenIndications For Human Albumin Infusion in A Neonatasri rachmawatiNoch keine Bewertungen
- Recurrent Parotitis in Children: Case Series and Literature ReviewDokument5 SeitenRecurrent Parotitis in Children: Case Series and Literature ReviewZenitraNoch keine Bewertungen
- 1479 6805 Joe 21 0449Dokument12 Seiten1479 6805 Joe 21 0449Salim MichaelNoch keine Bewertungen
- Prevalence of Prader-Willi Syndrome Among Infants With Hypotonia-2014Dokument4 SeitenPrevalence of Prader-Willi Syndrome Among Infants With Hypotonia-2014nikos.alexandrNoch keine Bewertungen
- Comparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialDokument5 SeitenComparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialVindee VictoryNoch keine Bewertungen
- Triple Marker ReportsDokument5 SeitenTriple Marker ReportsSurendra HolkarNoch keine Bewertungen
- Impact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesDokument8 SeitenImpact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesSri HariNoch keine Bewertungen
- Jurnal Hiperbilirubin 1Dokument7 SeitenJurnal Hiperbilirubin 1tita ismayaNoch keine Bewertungen
- Güven2015 Article GonadotropinReleasingHormoneAnDokument7 SeitenGüven2015 Article GonadotropinReleasingHormoneAnFunnie AdeliaNoch keine Bewertungen
- 18 - Fatema AlSaliti - Thyroid - Graves' DiseaseDokument1 Seite18 - Fatema AlSaliti - Thyroid - Graves' Diseasemohammed makkiNoch keine Bewertungen
- Poster Session V: Study Design: ConclusionDokument1 SeitePoster Session V: Study Design: ConclusionfujimeisterNoch keine Bewertungen
- Cit230 PDFDokument4 SeitenCit230 PDFJoyBoyXNoch keine Bewertungen
- Rahmawati 2019 IOP Conf. Ser. Earth Environ. Sci. 255 012001Dokument6 SeitenRahmawati 2019 IOP Conf. Ser. Earth Environ. Sci. 255 012001Ayu DiantariNoch keine Bewertungen
- OligomenorheaDokument6 SeitenOligomenorhealianaNoch keine Bewertungen
- Profil Kadar Bilirubin Pada Bayi Baru Lahir Sehat DGN Ikterus Di Rs. Dr. Sardjito Yogyakarta (Juliwati Dan Siti Muchayat)Dokument5 SeitenProfil Kadar Bilirubin Pada Bayi Baru Lahir Sehat DGN Ikterus Di Rs. Dr. Sardjito Yogyakarta (Juliwati Dan Siti Muchayat)brojeemNoch keine Bewertungen
- 1 s2.0 S168719792100040X MainDokument4 Seiten1 s2.0 S168719792100040X MainfelipetheNoch keine Bewertungen
- Newborn Screening in India: Focus on Hypothyroidism and DeafnessDokument6 SeitenNewborn Screening in India: Focus on Hypothyroidism and Deafnesssam2000samNoch keine Bewertungen
- Biotin Deficiency in HGDokument5 SeitenBiotin Deficiency in HGNur Aulia Pratiwi SallatuNoch keine Bewertungen
- Journal Fajar Ahmad PrasetyaDokument22 SeitenJournal Fajar Ahmad PrasetyaFajar Ahmad PrasetyaNoch keine Bewertungen
- Amh Serum Dan CairanDokument2 SeitenAmh Serum Dan CairanAnton ArifinNoch keine Bewertungen
- 1471 230X 7 9 PDFDokument5 Seiten1471 230X 7 9 PDFivanhariachandraNoch keine Bewertungen
- Gdiabetes GENESDokument7 SeitenGdiabetes GENESsalman672003Noch keine Bewertungen
- IJP - Volume 5 - Issue 12 - Pages 6189-6194Dokument6 SeitenIJP - Volume 5 - Issue 12 - Pages 6189-6194Yupie Faming JayaNoch keine Bewertungen
- Prenatal Testing For Down Syndrome: Comparison of Screening Practices in The UK and USADokument19 SeitenPrenatal Testing For Down Syndrome: Comparison of Screening Practices in The UK and USAtrevizanNoch keine Bewertungen
- 1607 4536 1 PBDokument7 Seiten1607 4536 1 PBdianNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsVon EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalVon EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNoch keine Bewertungen
- Anamnesis Dan PX Fisik CA ServiksDokument15 SeitenAnamnesis Dan PX Fisik CA ServiksRahma WatiNoch keine Bewertungen
- Somatic Dysfunction in FM PDFDokument25 SeitenSomatic Dysfunction in FM PDFHailey0% (1)
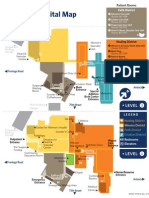
- SMMC District Map Without LogoDokument1 SeiteSMMC District Map Without LogofreedayumNoch keine Bewertungen
- 2018 PMAC Policy - CleanDokument7 Seiten2018 PMAC Policy - CleanHumanRights_PhNoch keine Bewertungen
- Haemtology QuestionDokument5 SeitenHaemtology QuestionKumar KP100% (1)
- SUTGMultiLocJ9981A PDFDokument60 SeitenSUTGMultiLocJ9981A PDFLouis MiuNoch keine Bewertungen
- Issue 22 - The Nurse Advocate - Hamad Medical Corporation - November 2015Dokument20 SeitenIssue 22 - The Nurse Advocate - Hamad Medical Corporation - November 2015Brent ForemanNoch keine Bewertungen
- ABC Medical AbbreviationsDokument158 SeitenABC Medical AbbreviationsXiaxin Liu100% (1)
- Diagnostic Endocrinology Blood Steroid Concentrations in Neutered Male and Female HabbitsDokument4 SeitenDiagnostic Endocrinology Blood Steroid Concentrations in Neutered Male and Female HabbitsThatiana SanchesNoch keine Bewertungen
- 09 Prostate Cancer 2017 WebDokument146 Seiten09 Prostate Cancer 2017 WebDharmesh PatelNoch keine Bewertungen
- Arthroscopic Inlay PCL Reconstruction Using The FlipCutter and PCL TightRopeDokument12 SeitenArthroscopic Inlay PCL Reconstruction Using The FlipCutter and PCL TightRopeNghĩa Nguyễn TrọngNoch keine Bewertungen
- What About Bob (Screenplay)Dokument129 SeitenWhat About Bob (Screenplay)Pragyan ThapaNoch keine Bewertungen
- By: Sir BornieDokument13 SeitenBy: Sir Borniebornie100% (2)
- GonadoDokument32 SeitenGonadoshailendra meena50% (2)
- Plastic Surgery, Popular Culture, and The Cosmetic GazeDokument10 SeitenPlastic Surgery, Popular Culture, and The Cosmetic GazeShelbi DanielleNoch keine Bewertungen
- Summer Training Project ReportDokument59 SeitenSummer Training Project ReportDr. Sunaina Lashkari100% (2)
- LacerationsDokument2 SeitenLacerationsGoldyNoch keine Bewertungen
- DLSHSI ASCPEO Template INSTRUCTIONAL DESIGN FOR CONTINUING DEVELOPMENT PROGRAM ACTIVITYDokument2 SeitenDLSHSI ASCPEO Template INSTRUCTIONAL DESIGN FOR CONTINUING DEVELOPMENT PROGRAM ACTIVITYDustin GrimaresNoch keine Bewertungen
- Lecture 6 Acrylic RPDDokument23 SeitenLecture 6 Acrylic RPDAmmar AldawoodyehNoch keine Bewertungen
- On The Absolute Sincerity of Great PhysiciansDokument2 SeitenOn The Absolute Sincerity of Great PhysiciansJessé de AndradeNoch keine Bewertungen
- Renal Disease in PregnancyDokument32 SeitenRenal Disease in PregnancyHannahKarizaNoch keine Bewertungen
- Form No.1 Birth ReportDokument4 SeitenForm No.1 Birth ReportSruthy SasiNoch keine Bewertungen
- Ijwh 218933 Retained Placenta After Vaginal Delivery Risk Factors and M 2Dokument8 SeitenIjwh 218933 Retained Placenta After Vaginal Delivery Risk Factors and M 2terry mutiaNoch keine Bewertungen
- ACR Recomendations On Exposure TimeDokument9 SeitenACR Recomendations On Exposure TimeMuhammad AreebNoch keine Bewertungen
- EGENS One Step HCG Cassette 2 Page InsDokument3 SeitenEGENS One Step HCG Cassette 2 Page InsAdams FonsecaNoch keine Bewertungen
- Multiple Pregnancy PDFDokument12 SeitenMultiple Pregnancy PDFHaidar AmrNoch keine Bewertungen
- Apollo Hospital Marketing Assignment: 1. Executive SummaryDokument13 SeitenApollo Hospital Marketing Assignment: 1. Executive Summaryraghavi20Noch keine Bewertungen
- Fetal Neurophysiology According To Gestational Age Aida Salihagic Kadic, Maja PredojevicDokument5 SeitenFetal Neurophysiology According To Gestational Age Aida Salihagic Kadic, Maja PredojevicDaniela Isidora San Martin CanalesNoch keine Bewertungen
- MCM 2019 2021 Project Proposal Application - Nur Melani Sari - EditDokument20 SeitenMCM 2019 2021 Project Proposal Application - Nur Melani Sari - EditNur Melani Sari WardaniNoch keine Bewertungen
- Professional Growth and DevelopmentDokument21 SeitenProfessional Growth and Developmentconinitas81% (27)