Das könnte Ihnen auch gefallen
- Treating ADHD PDFDokument257 SeitenTreating ADHD PDFHamdon Hamad80% (5)
- Narcissistic Personality Disorder Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis - UpToDateDokument16 SeitenNarcissistic Personality Disorder Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis - UpToDatechysa100% (2)
- Conversion Disorder, Functional Neurological Symptom Disorder, and Chronic Pain - Comorbidity, Assessment, and TreatmentDokument10 SeitenConversion Disorder, Functional Neurological Symptom Disorder, and Chronic Pain - Comorbidity, Assessment, and TreatmentViviana CalderónNoch keine Bewertungen
- Endocrinology and Metabolism Clinics-Lípidos 2009Dokument234 SeitenEndocrinology and Metabolism Clinics-Lípidos 2009Tony Miguel Saba SabaNoch keine Bewertungen
- Erc Cap PDFDokument299 SeitenErc Cap PDFSilvia Ramos YllescasNoch keine Bewertungen
- Lipids Module 4Dokument16 SeitenLipids Module 4angelmedurNoch keine Bewertungen
- Androgen Deprivation TherapyDokument27 SeitenAndrogen Deprivation TherapyJane DayNoch keine Bewertungen
- 2 Metabolic - Syndrom - Sherling DHDokument3 Seiten2 Metabolic - Syndrom - Sherling DHM JNoch keine Bewertungen
- New Insights Into The Statin-Cholesterol Controversy: Timothy M. Marshall, PH.DDokument5 SeitenNew Insights Into The Statin-Cholesterol Controversy: Timothy M. Marshall, PH.DFathurrahman AndiyogaNoch keine Bewertungen
- Intensive Statin Therapy - A Sea Change in Cardiovascular PreventionDokument3 SeitenIntensive Statin Therapy - A Sea Change in Cardiovascular Preventionsyaiful rinantoNoch keine Bewertungen
- Dislipidemia Ann Int Med Jun 2023Dokument17 SeitenDislipidemia Ann Int Med Jun 2023pepegiovanny100% (1)
- Busting The Myth of Saturated Fat in Heart Disease British Medical Journal 2013Dokument2 SeitenBusting The Myth of Saturated Fat in Heart Disease British Medical Journal 2013jackjensen2852Noch keine Bewertungen
- Risk Related To Hormone Therapy and Cardiovascular Disease in WomenDokument44 SeitenRisk Related To Hormone Therapy and Cardiovascular Disease in Womenosama saeedNoch keine Bewertungen
- Hypertriglyceridemia - Common Causes, Prevention and Treatment StrategiesDokument10 SeitenHypertriglyceridemia - Common Causes, Prevention and Treatment Strategiesfaqihu rizkyNoch keine Bewertungen
- Published,, Noval Anti-Cancer TherapiesDokument10 SeitenPublished,, Noval Anti-Cancer Therapiesshayma rafatNoch keine Bewertungen
- Efek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularDokument6 SeitenEfek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularAndrie WigunaNoch keine Bewertungen
- Nihms 1020972Dokument11 SeitenNihms 1020972Carlos Alfredo Pedroza MosqueraNoch keine Bewertungen
- Cardiovascular Safety Profile of Currently Available Diabetic DrugsDokument17 SeitenCardiovascular Safety Profile of Currently Available Diabetic Drugsvina_nursyaidahNoch keine Bewertungen
- Atherogenic Dyslipidemia in Patients With Established Coronary Artery DiseaseDokument6 SeitenAtherogenic Dyslipidemia in Patients With Established Coronary Artery DiseasebilahalvirayuNoch keine Bewertungen
- Management of Hypertriglyceridemia: Vinaya SimhaDokument19 SeitenManagement of Hypertriglyceridemia: Vinaya SimhaKarina IlesNoch keine Bewertungen
- Exercício em Pacientes Com CâncerDokument20 SeitenExercício em Pacientes Com CâncerDrDermeval Reis JuniorNoch keine Bewertungen
- Cuadro de Horarios Paa RellenarDokument7 SeitenCuadro de Horarios Paa RellenarLuis ChangaNoch keine Bewertungen
- New England Journal Medicine: The ofDokument5 SeitenNew England Journal Medicine: The ofAri Hidriansyah AtmajaNoch keine Bewertungen
- Circulation 2012 Berger 491 500Dokument11 SeitenCirculation 2012 Berger 491 500Nurul Azmi Rosmala PutriNoch keine Bewertungen
- Overcoming Toxicity and Side-Effects of 2014Dokument14 SeitenOvercoming Toxicity and Side-Effects of 2014Andi MuftyNoch keine Bewertungen
- How Statistical Deception Created The Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular DiseaseDokument11 SeitenHow Statistical Deception Created The Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular DiseaseodhiseoNoch keine Bewertungen
- Vascular Medicine UpdatesDokument19 SeitenVascular Medicine Updatessam samiNoch keine Bewertungen
- Medical Optimization of The Peripheral Artery Disease PatientDokument11 SeitenMedical Optimization of The Peripheral Artery Disease Patientafso afsoNoch keine Bewertungen
- Management of Hypertriglyceridemia: Vinaya SimhaDokument19 SeitenManagement of Hypertriglyceridemia: Vinaya SimhaJose S. M. TorrezNoch keine Bewertungen
- Thiazides and Diabetes: Pharmacist'S Letter / Prescriber'S LetterDokument2 SeitenThiazides and Diabetes: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- Jurnal 4 WordDokument20 SeitenJurnal 4 WordSri MaryatiNoch keine Bewertungen
- A Systematic Review and Meta-Analysis of Ayurvedic Herbal Preparations For HypercholesterolemiaDokument24 SeitenA Systematic Review and Meta-Analysis of Ayurvedic Herbal Preparations For HypercholesterolemiaSotiris AnagnostopoulosNoch keine Bewertungen
- MRC-BHF Heart Protection Study PDFDokument16 SeitenMRC-BHF Heart Protection Study PDFArif KurniadiNoch keine Bewertungen
- Stroke Prevention: Multimedia Library ReferencesDokument17 SeitenStroke Prevention: Multimedia Library Referencesmochamad rizaNoch keine Bewertungen
- Update On The Pathophysiology and Medical Treatment of Peripheral Artery DiseaseDokument20 SeitenUpdate On The Pathophysiology and Medical Treatment of Peripheral Artery DiseaseRumah Sakit J. H. Awaloei ManadoNoch keine Bewertungen
- Manejo de La HipertrigliceridemiaDokument19 SeitenManejo de La HipertrigliceridemiaJulissa Del Carmen Cruz PintoNoch keine Bewertungen
- Evidence Based Cardiology 4th EdDokument424 SeitenEvidence Based Cardiology 4th EdROGER LUDEÑA SALAZARNoch keine Bewertungen
- Pharmacological Treatment of HyperlipiedmiaDokument8 SeitenPharmacological Treatment of HyperlipiedmiajeffaguilarNoch keine Bewertungen
- Alternative and Complementary Medicine For Preventing and Treating Cardiovascular DiseaseDokument72 SeitenAlternative and Complementary Medicine For Preventing and Treating Cardiovascular Diseaseangeli2230Noch keine Bewertungen
- 10 1016@j Jaccao 2020 04 007Dokument10 Seiten10 1016@j Jaccao 2020 04 007ramangNoch keine Bewertungen
- Pathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCDokument42 SeitenPathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCCalvin LitraNoch keine Bewertungen
- DyslipidemiaManagement Continuum 2011Dokument13 SeitenDyslipidemiaManagement Continuum 2011Zuleika DöObsönNoch keine Bewertungen
- Pathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCDokument42 SeitenPathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCSherleen HeiNoch keine Bewertungen
- Diet 4 Stroke PreventionDokument7 SeitenDiet 4 Stroke PreventionNila AuthoriaNoch keine Bewertungen
- Safety and Efficacy of Statin TherapyDokument13 SeitenSafety and Efficacy of Statin TherapyAlexa ArceNoch keine Bewertungen
- Dislipidemia ACP 2017Dokument16 SeitenDislipidemia ACP 2017José Luis PradoNoch keine Bewertungen
- Potential Clinical Benefits of D-Ribose in Ischemic Cardiovascular DiseaseDokument11 SeitenPotential Clinical Benefits of D-Ribose in Ischemic Cardiovascular DiseaseNabilaNoch keine Bewertungen
- Harmonizing The Metabolic SyndromeDokument7 SeitenHarmonizing The Metabolic SyndromeCarlos_RuedasNoch keine Bewertungen
- Ban JASH2009Dokument15 SeitenBan JASH2009Adek FahmialdiNoch keine Bewertungen
- 2018 Dislipidemia-RevisaDokument16 Seiten2018 Dislipidemia-RevisaLuminita HutanuNoch keine Bewertungen
- Vitamin DDokument12 SeitenVitamin DLia NadaNoch keine Bewertungen
- Lipid Management in Patients With Endocrine Disorders An EndocrineDokument70 SeitenLipid Management in Patients With Endocrine Disorders An Endocrinealialison7666Noch keine Bewertungen
- Diretriz - Dislipidemia EndocrinologiaDokument70 SeitenDiretriz - Dislipidemia EndocrinologiaSamara QueirozNoch keine Bewertungen
- Ades-The Treatment of Obesity in Cardiac Rehabilitation 2021Dokument7 SeitenAdes-The Treatment of Obesity in Cardiac Rehabilitation 2021markwsheppardhotmail.comNoch keine Bewertungen
- Hta TtoDokument13 SeitenHta TtoAmelia RiveraNoch keine Bewertungen
- Riddell PDFDokument24 SeitenRiddell PDFMartha Yaneth VelasquezNoch keine Bewertungen
- 1 s2.0 S0002870320302143 MainDokument9 Seiten1 s2.0 S0002870320302143 MaindeepNoch keine Bewertungen
- VITAMINA D y Riesgo CardiovascularDokument12 SeitenVITAMINA D y Riesgo CardiovascularAngusNoch keine Bewertungen
- The Guidelines Battle On Starting Statins: Clinical DecisionsDokument7 SeitenThe Guidelines Battle On Starting Statins: Clinical DecisionsPedro MontañoNoch keine Bewertungen
- Treatment of HypertensionDokument23 SeitenTreatment of HypertensionRABIATUL ADAWIYAHNoch keine Bewertungen
- Update On Anti Platelet TherapyDokument4 SeitenUpdate On Anti Platelet TherapyhadilkNoch keine Bewertungen
- Atp 3 Upd 04Dokument13 SeitenAtp 3 Upd 04api-3696252Noch keine Bewertungen
- Long Term Testosterone Therapy Improves Liver Parameters and Steatosis in Hypogonadal Men A Prospective Controlled Registry StudyDokument12 SeitenLong Term Testosterone Therapy Improves Liver Parameters and Steatosis in Hypogonadal Men A Prospective Controlled Registry StudyKodagnanaso kodagNoch keine Bewertungen
- Unveiling the Unseen: A Journey Into the Hearts Labyrinth SeanVon EverandUnveiling the Unseen: A Journey Into the Hearts Labyrinth SeanNoch keine Bewertungen
- DC DC Converter BOMDokument1 SeiteDC DC Converter BOMFady HachemNoch keine Bewertungen
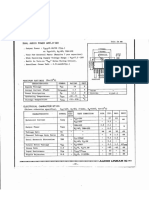
- TA7230PDokument4 SeitenTA7230PFady HachemNoch keine Bewertungen
- An920 DDokument40 SeitenAn920 DFady HachemNoch keine Bewertungen
- Application Note AN4105Dokument23 SeitenApplication Note AN4105Fady HachemNoch keine Bewertungen
- BD438Dokument5 SeitenBD438Fady HachemNoch keine Bewertungen
- AN954Dokument14 SeitenAN954Fady HachemNoch keine Bewertungen
- Fly Back ConverterDokument1 SeiteFly Back ConverterFady HachemNoch keine Bewertungen
- Smps v2.1 SCHDokument1 SeiteSmps v2.1 SCHFady Hachem0% (1)
- Very Good: L 535.9 H The Core Is..Dokument1 SeiteVery Good: L 535.9 H The Core Is..Fady HachemNoch keine Bewertungen
- Prot BRD CMDokument1 SeiteProt BRD CMFady HachemNoch keine Bewertungen
- SMPS SchematicDokument1 SeiteSMPS SchematicFady HachemNoch keine Bewertungen
- 2N60 PDFDokument7 Seiten2N60 PDFFady HachemNoch keine Bewertungen
- Byv52 200Dokument7 SeitenByv52 200Fady HachemNoch keine Bewertungen
- Ir 21531Dokument1 SeiteIr 21531Fady HachemNoch keine Bewertungen
- Application Note AN4105Dokument23 SeitenApplication Note AN4105Fady HachemNoch keine Bewertungen
- PT Cpi Web Evaluation: 1. Professional Practice - SafetyDokument6 SeitenPT Cpi Web Evaluation: 1. Professional Practice - Safetyapi-468012516Noch keine Bewertungen
- André 2018 ReviewDokument9 SeitenAndré 2018 ReviewAndry Wahyudi AgusNoch keine Bewertungen
- Mwanza College of Health and Allied Sciense: (Mwachas)Dokument8 SeitenMwanza College of Health and Allied Sciense: (Mwachas)Moses FrancoNoch keine Bewertungen
- Related LiteratureDokument16 SeitenRelated LiteratureivahcamilleNoch keine Bewertungen
- EgyptJSurg392455-2016706 053607Dokument6 SeitenEgyptJSurg392455-2016706 053607rendi wibowoNoch keine Bewertungen
- Abnormal Child Psychology 6th Edition Mash Wolfe Test BankDokument25 SeitenAbnormal Child Psychology 6th Edition Mash Wolfe Test BankJudithHollandxdwj100% (49)
- Jurnal Terindeks ScopusDokument8 SeitenJurnal Terindeks ScopusAyu Sisca PrastiwiNoch keine Bewertungen
- Annotated BibliographyDokument4 SeitenAnnotated Bibliographyapi-284834629Noch keine Bewertungen
- IRDA Claim FormDokument4 SeitenIRDA Claim FormSatya SundarNoch keine Bewertungen
- Obsesiv CompulsivDokument2 SeitenObsesiv CompulsivGaby GavrilasNoch keine Bewertungen
- Systematic Review of Effect of Involuntary Treatment For People With Anorexia Nervosa, and An Analysis of Patient CharacteristicsDokument10 SeitenSystematic Review of Effect of Involuntary Treatment For People With Anorexia Nervosa, and An Analysis of Patient CharacteristicsCarla MesquitaNoch keine Bewertungen
- JMM 29 119Dokument8 SeitenJMM 29 119subanant11Noch keine Bewertungen
- Journal of A Ffective Disorders: Ling-Yi Wang, Jen-Huai Chiang, Shih-Fen Chen, Yu-Chih ShenDokument7 SeitenJournal of A Ffective Disorders: Ling-Yi Wang, Jen-Huai Chiang, Shih-Fen Chen, Yu-Chih Shennermal93Noch keine Bewertungen
- KJFM 19 0081Dokument9 SeitenKJFM 19 0081Shelviana ShelvianaNoch keine Bewertungen
- CAC Basic Guide v1.10 - 11072021 3Dokument10 SeitenCAC Basic Guide v1.10 - 11072021 3Atikah NorzetNoch keine Bewertungen
- Ryan Et Al 2023 Adhd and Anxiety Symptom Comorbidity From An Event Segmentation LensDokument14 SeitenRyan Et Al 2023 Adhd and Anxiety Symptom Comorbidity From An Event Segmentation LensCarlos ReyesNoch keine Bewertungen
- Test 1 All NotesDokument41 SeitenTest 1 All NotesLizethNoch keine Bewertungen
- Chapter 37: Dialysis Decisions in The Elderly Patient With Advanced CKD and The Role of Nondialytic TherapyDokument8 SeitenChapter 37: Dialysis Decisions in The Elderly Patient With Advanced CKD and The Role of Nondialytic Therapykhangha.ptNoch keine Bewertungen
- UntitledDokument12 SeitenUntitledRicardo Andres Bowen HolguinNoch keine Bewertungen
- Jaa 178927 Approaches To The Assessment of Severe Asthma Barriers and PDFDokument17 SeitenJaa 178927 Approaches To The Assessment of Severe Asthma Barriers and PDFNikki LangatoNoch keine Bewertungen
- Godi Szilard PHD DolgozatDokument103 SeitenGodi Szilard PHD DolgozatHry EzaNoch keine Bewertungen
- WCW - Guide For The Management of Obesity in The Primary Care SettingDokument15 SeitenWCW - Guide For The Management of Obesity in The Primary Care SettingCristina Saldias PorrasNoch keine Bewertungen
- Breaking The Relapse Cycle - FSM Research 2019Dokument70 SeitenBreaking The Relapse Cycle - FSM Research 2019Marcelle BugreNoch keine Bewertungen
- What Are The True Goals of Social WorkDokument4 SeitenWhat Are The True Goals of Social WorkfrancesNoch keine Bewertungen
- Manual For Documenting Diagnosis in Per-Pd 301 - 2013 PDFDokument33 SeitenManual For Documenting Diagnosis in Per-Pd 301 - 2013 PDFNeeta AnandaNoch keine Bewertungen
- Recognizing and Reporting Red Flags For The Physical Therapist Assistant 1stDokument52 SeitenRecognizing and Reporting Red Flags For The Physical Therapist Assistant 1stsummer.yates611100% (40)